(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Oral Abstract Session: Genitourinary Cancer—Prostate, Testicular, and Penile. Dr. Ana Aparicio presented C3NIRA: A Randomized phase II study of carboplatin-cabazitaxel-cetrelimab (anti-PD-1) induction followed by niraparib +/- cetrelimab maintenance in men with aggressive variant prostate cancers (AVPC).
Aggressive Variant Prostate Cancer (AVPC) encompasses a heterogeneous group of tumors with varying responses to androgen receptor (AR) blockade. These are broadly classified into three subtypes: androgen addicted, which are highly responsive to AR-targeted therapies; androgen enabled, which rely partly on AR signaling; and androgen indifferent, which account for approximately 20% of cases and represent the most lethal subset. The androgen indifferent group is particularly challenging due to its resistance to standard AR therapies and the current lack of effective treatment strategies or robust predictive biomarkers, highlighting a critical area of unmet need in prostate cancer care.

Dr. Aparicio and colleagues outlined a set of clinical and molecular features used to identify patients with androgen indifferent prostate cancer, known as the AVPC criteria. These include:
- Small cell carcinoma morphology
- Visceral metastases only
- Lytic bone metastases
- Bulky lymph nodes or prostate mass
- Low PSA level relative to overall tumor volume
- Elevated serum carcinoembryonic antigen (CEA) or lactate dehydrogenase (LDH)
- Primary castration resistance
- Concurrent alterations in TP53, RB1, and PTEN
- Radiographic (RECIST) progression with PSA <1 ng/mL
The C-COLA trial (NCT03263650) was a two-part study in AVPC assessing chemotherapy induction followed by PARP inhibitor maintenance. Initially, 96 patients were treated with six cycles of carboplatin plus cabazitaxel. Of these, 35 (36%) experienced progression and 7 (7%) discontinued due to toxicity or other reasons. The remaining patients were randomized 2:1 to maintenance with olaparib (n=36) or observation (n=18). While the trial did not reach statistical significance (HR 0.61; 90% CI 0.36–1.03; p=0.12), there was a numerical improvement in median progression-free survival (mPFS) from randomization in the olaparib arm (4.9 months vs 2.3 months). This trial laid the groundwork for C3NIRA.

Dr Aparicio highlighted that in a translational analysis from the C-COLA trial, paired pre- and post-chemotherapy biopsies revealed distinct immune pathway dynamics between responders and non-responders. In prolonged responders, inflammatory immune pathways such as interferon responses and allograft rejection were upregulated following chemotherapy, suggesting an enhanced antitumor immune environment. In contrast, these same pathways were downregulated in chemotherapy progressors. Additionally, a post hoc analysis of DDR mutations (n=63) suggested that the presence of pathogenic alterations may correlate with longer progression-free and overall survival after chemotherapy, further supporting the rationale for PARP inhibitor maintenance in this setting.

The hypothesis for the C3NIRA trial is that adding PD-1 inhibition to chemotherapy induction and PARP inhibitor maintenance can enhance immune-mediated anti-tumor responses and prolong the duration of benefit in men with AVPC.
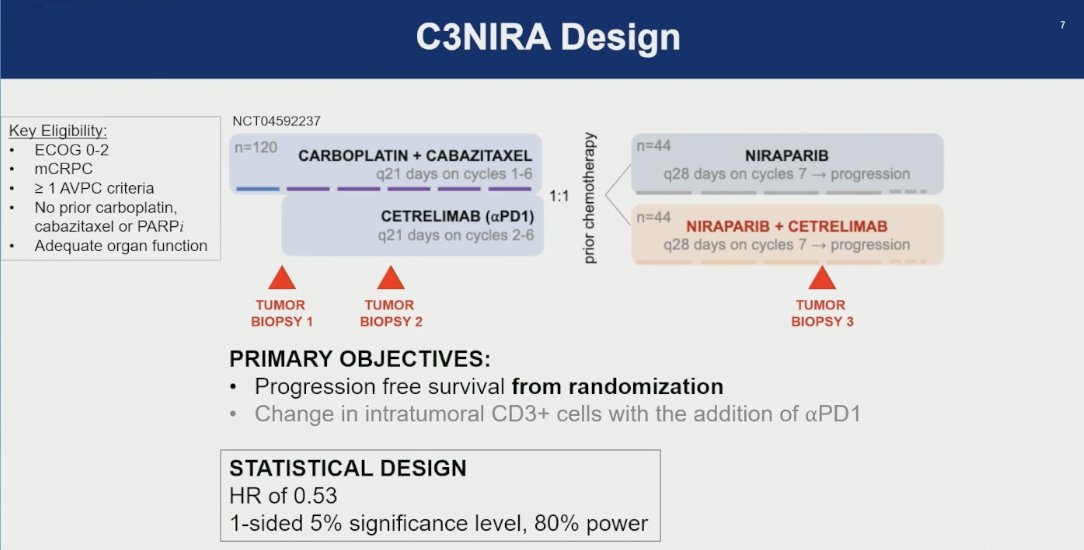
The C3NIRA trial (NCT04592237) is an investigator-initiated phase II study evaluating the addition of αPD1 (cetrelimab) to carboplatin and cabazitaxel induction followed by niraparib ± cetrelimab maintenance in patients with mCRPC and ≥1 AVPC criteria. Eligible patients had ECOG 0–2, no prior exposure to PARPi, cabazitaxel, or carboplatin, and adequate organ function. Participants first receive 6 cycles of induction chemotherapy (carboplatin + cabazitaxel), with cetrelimab given on cycles 2–6, and are then randomized 1:1 to maintenance with either niraparib alone or niraparib + cetrelimab. Tumor biopsies are obtained at three time points baseline, after chemotherapy, and during maintenance to assess intratumoral CD3+ T-cell infiltration. The trial’s co-primary endpoints are PFS from randomization and changes in intratumoral CD3+ cells.
A total of 120 patients were treated with induction chemotherapy between January 2021 and May 2024. Among them, 25% had received prior chemotherapy, 27% had liver metastases, and baseline PSA levels were relatively low, with a median of 7.5 ng/mL

Unfortunately, cetrelimab (αPD1) did not overcome chemotherapy resistance in patients with AVPC. Among those treated, 35.8% experienced progression, 12.5% discontinued due to toxicity, and 1.7% withdrew for other reasons resulting in high dropout and reduced post-induction randomization numbers (N=30 in each arm) as shown below.

Notably, Baseline Clinicopathological Features did not categorically. distinguish Randomized from Non-Randomized Patients as shown below.

Despite the small sample size, the addition of cetrelimab (αPD1) to niraparib maintenance following induction significantly improved both progression-free and overall survival in men with AVPC. Median PFS from randomization was 8.8 months in the niraparib + cetrelimab arm compared to 3.3 months with niraparib alone (HR 0.50, 90% CI: 0.30–0.82; p=0.02). Median OS was also notably longer with combination therapy at 24.3 months versus 10.2 months with niraparib alone (HR 0.51, 90% CI: 0.29–0.89; p=0.04).

A total of 64 grade ≤2 toxicities and 45 grade ≥3 toxicities were documented during induction, including two cases of grade 5 neutropenic sepsis, as illustrated in the table below.

During the maintenance phase, a higher number of adverse events were numerically observed in the Niraparib + Cetrelimab group compared to Niraparib alone. However, the incidence of grade ≥3 AEs was similar between both treatment arms

The preliminary correlative analyses from the C3NIRA trial suggest that immune activation aligns with clinical response. Patients classified as prolonged responders showed a higher frequency of CD8⁺GZMB⁺ effector T cells and a reduction in CD4⁺FoxP3⁺ regulatory T cells following induction chemotherapy with carboplatin, cabazitaxel, and cetrelimab. In contrast, chemotherapy progressors demonstrated the opposite pattern.

A post hoc analysis of clinically available germline mutations (n=92) revealed that most patients did not harbor detectable alterations. Among those with known pathogenic DNA damage repair (DDR) mutations, notable variants included ATM c.2T>C, several BRCA2 mutations (c.4965C>G, c.5655C>A, c.7485dup), CHEK2 c.1583_1620dup, and PMS2 mutations (c.137G>T and a deletion of exon 8). Importantly, somatic mutation data are still pending and were not included in this preliminary report.

Dr. Aparicio concluded her presentation by emphasizing several key takeaways:
- The AVPC (Aggressive Variant Prostate Cancer) criteria offer a useful framework for developing therapies for biologically distinct prostate cancer subsets.
- Adding α-PD1 inhibition to platinum-taxane induction, followed by PARP inhibitor maintenance, showed meaningful clinical benefit in a subset of men with AVPC.
- This approach carries a notable risk of toxicity, highlighting the need for careful patient selection.
- On-treatment tumor biopsy analysis provides insights that may help guide future rational combination strategies
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.