(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Rana McKay discussing the molecular and clinical characterization of KLK2 mRNA expression in prostate cancer. KLK2 is an androgen-regulated gene that plays a critical role in prostate cancer biology.
It exists in both secreted and membrane-associated forms, with the latter being a potential therapeutic target in prostate cancer, which has been demonstrated in preclinical and early clinical studies. Given the development of KLK-2 targeted therapies, the investigators sought to characterize the molecular and clinical features associated with KLK2 mRNA expression in prostate cancer.
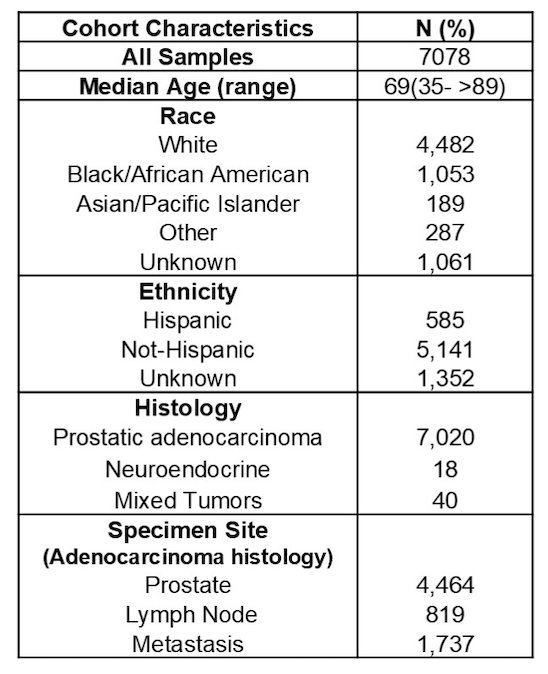
NextGen sequencing of DNA (592-gene/whole exome) and RNA (whole transcriptome) was performed on prostate cancer specimens (n = 7,078). From this, adenocarcinoma histology (n = 7,020) was used exclusively for this analysis. KLK2-High/Low expression was defined as >75th /<25th quartile RNA transcripts per million (TPM). Castrate resistant prostate cancer (CRPC) and hormone sensitive prostate cancer (HSPC) were defined based on ADT duration prior to tissue collection: HSPC < 3 and CRPC ≥ 3 months from ADT start. Overall survival was defined as the time of collection or first androgen receptor pathway inhibitor to death/last follow-up.
Specimens were derived from primary prostate (n = 4,464, 63.1%), lymph nodes (n = 819, 11.6%) or other metastatic sites (n = 1,737, 24.5%):
Higher KLK2 was observed in tumors from Black versus White patients (8.88 versus 8.75 log2[TPM+1], p < 0.001):
![Higher KLK2 was observed in tumors from Black versus White patients (8.88 versus 8.75 log2[TPM+1], p < 0.001):](/images/com-doc-importer/215-asco-2025/asco-2025-molecular-and-clinical-characterization-of-klk2-mrna-expression-in-prostate-cancer/image-1.jpg)
KLK2 was enriched in adenocarcinoma versus mixed versus neuroendocrine prostate cancer (8.79 versus 7.58 versus 0.33 log2[TPM+1], p < 0.001):
![KLK2 was enriched in adenocarcinoma versus mixed versus neuroendocrine prostate cancer (8.79 versus 7.58 versus 0.33 log2[TPM+1], p < 0.001):](/images/com-doc-importer/215-asco-2025/asco-2025-molecular-and-clinical-characterization-of-klk2-mrna-expression-in-prostate-cancer/image-2.jpg)
Relative to primary tumors (8.93 log2[TPM+1]), KLK2 varied by metastatic site, with lowest expression in gastrointestinal (7.46 Log2[TPM+1], p < 0.001), liver (7.88 log2[TPM+1], p < 0.001), and CNS (8.25 log2[TPM+1], p < 0.001) metastatic sites.
In primary tumors, high KLK2 associated positively with SPOP and negatively with PI3K/PTEN, TP53, and RB1 alterations. Across primary, lymph node, and distant metastatic tumors, high KLK2 associated positively with androgen receptor signaling and negatively with neuroendocrine prostate cancer signaling (all p < 0.001). KLK2 strongly correlated with KLK3 (PSA) expression (R = 0.87):
KLK2 expression was higher in HSPC (n = 1504) versus CRPC (n = 4519) tumors (1.78 Log2[TPM+1], p < 0.001). Among HSPC, KLK2-high tumors had decreased TP53, RB1, AKT1, BRCA1 and increased SPOP, CTNNB1, PTEN, BRCA2 mutations. CRPC tumors with high KLK2 had decreased RB1, TP53, PIK3CA and increased RAD54L and ATM mutations compared to low tumors:
![KLK2 expression was higher in HSPC (n = 1504) versus CRPC (n = 4519) tumors (1.78 Log2[TPM+1], p < 0.001). Among HSPC, KLK2-high tumors had decreased TP53, RB1, AKT1, BRCA1 and increased SPOP, CTNNB1, PTEN, BRCA2 mutations. CRPC tumors with high KLK2 had decreased RB1, TP53, PIK3CA and increased RAD54L and ATM mutations compared to low tumors:](/images/com-doc-importer/215-asco-2025/asco-2025-molecular-and-clinical-characterization-of-klk2-mrna-expression-in-prostate-cancer/image-4.jpg)
High KLK2 was also associated with improved overall survival from collection time (median 69.7 versus 35.9 months, p < 0.001) and first androgen receptor pathway inhibitor initiation (median 48.9 versus 39.5 months, p < 0.001). KLK2-high HSPC and CRPC tumors had improved overall survival compared to low tumors (median 82.0 HSPC KLK2-high versus 54.3 HSPC KLK2-low versus 23.7 CRPC KLK2-high versus 16.3 CRPC KLK2-low months, q < 0.01). The combination of KLK2-high/AR-high was associated with increased overall survival compared to KLK2-high/AR-low, KLK2-low/AR-high, and KLK2-low/AR-low tumors (median 70.8 versus 48.8 versus 43.5 versus 20.8 months, respectively, p < 0.001):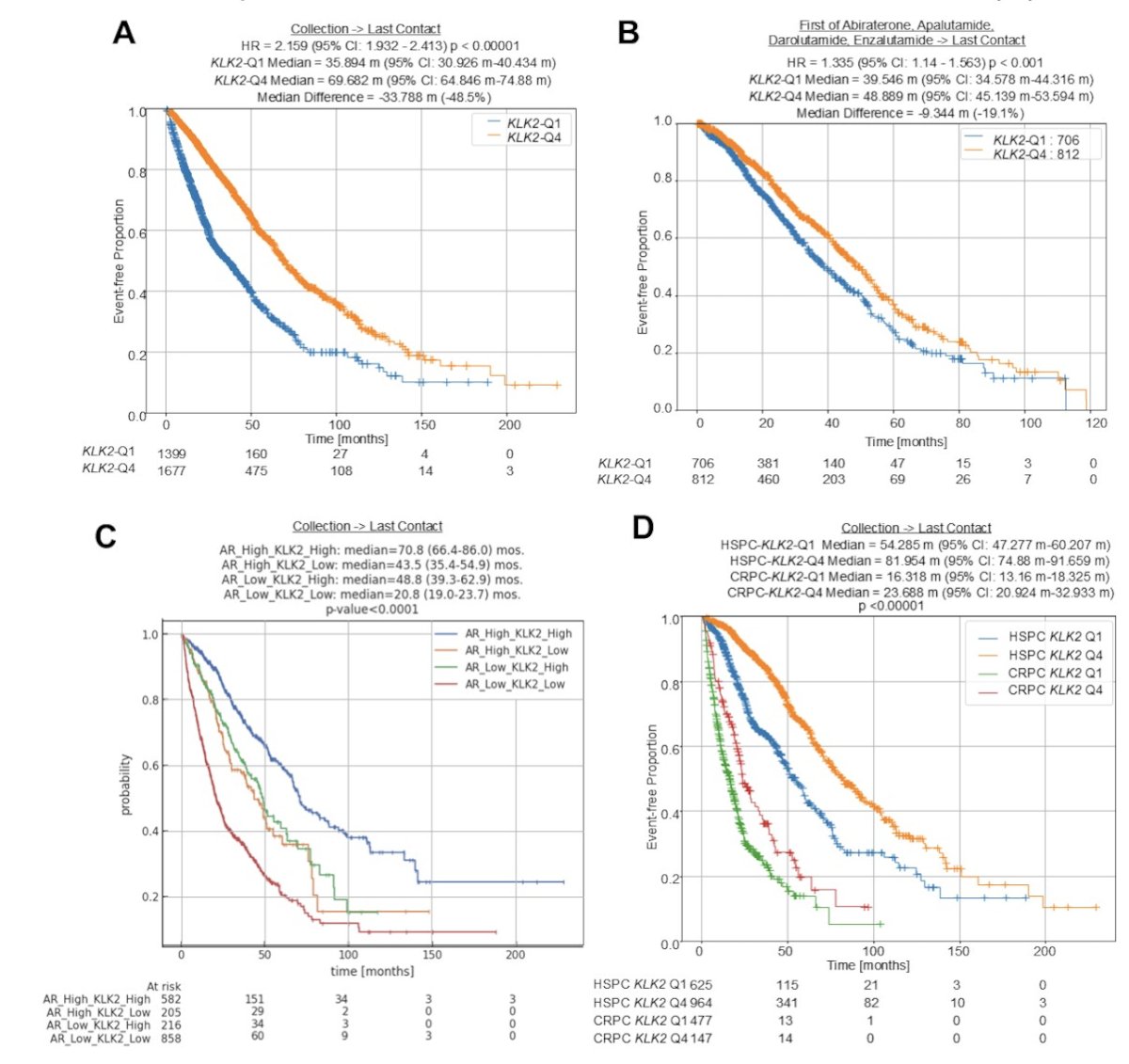
Dr. McKay concluded her presentation discussing the molecular and clinical characterization of KLK2 mRNA expression in prostate cancer with the following take-home points:
- This large-scale clinic-genomic analysis reveals distinct patterns of KLK2 expression in prostate cancer
- Significantly higher KLK2 expression is observed in black or African American patients, and lower expression in white patients
- Patients with high KLK2 expression had better outcomes compared to those with low KLK2 expression
- Tumors with high KLK2 are molecularly distinct, providing insights for unique therapeutic strategies in this group
Presented by: Rana McKay, MD, Moores Cancer Center, University of California, San Diego, La Jolla, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.