(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a prostate, testicular, and penile cancers poster session. Dr. Dana Rathkopf presented the results of a real-world analysis of patient characteristics, treatment patterns, and overall survival in metastatic hormone-sensitive prostate cancer (mHSPC) by PTEN mutational status.
Overall, the survival outcomes for metastatic prostate cancer remain poor (5‑year overall survival [OS]: 38%), with an estimated median OS of 30 months for mHSPC patients.1,2 Genomic alterations of phosphatase and tensin homologue (PTEN), such as mutations or deletions, occur more frequently in the metastatic setting and can be one mechanism leading to reduced or absent PTEN function.3-5 Multiple mechanisms can affect PTEN function; thus, genomic alterations may not directly correlate with the level of PTEN protein deficiency.6 Loss of function of the PTEN gene is associated with an increased risk of recurrence and poor clinical outcomes in patients with metastatic prostate cancer.6
Patient characteristics and survival outcomes for patients with mHSPC with PTEN-altered tumors receiving standard of care therapies have not been well investigated in a real-world setting.
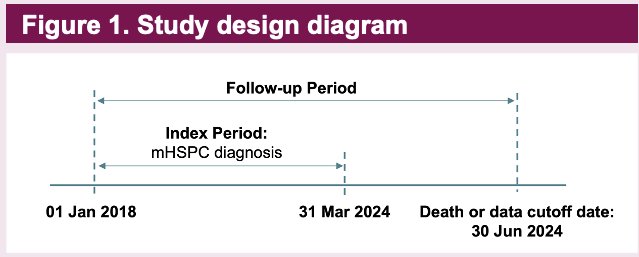
This longitudinal cohort study used secondary data from the US-based FH-FMI CGDB database (cutoff date: 30 Jun 2024).7-10 Eligible male patients had a diagnosis of mHSPC between January 1, 2018, and March 31, 2024. Patients who received an investigational drug prior to their mHSPC diagnosis were excluded. Eligible patients were required to have ≥1 solid tissue specimen that underwent comprehensive genomic profiling (CGP) with a panel that included a valid result for PTEN.
The PTEN-altered group included patients with a tumor harboring a homozygous deletion (copy number variant = 0) or mutation (known or likely pathogenic short variant alterations or rearrangements). All other patients were included in the PTEN-non-altered group.
Patient characteristics and treatment patterns were descriptively analysed. Kaplan-Meier estimates for real-world OS (rwOS; unadjusted) by PTEN status were estimated for all patients, by treatment type in the 1st line mHSPC setting, and for the de novo subgroup (i.e. patients with M1 stage at initial diagnosis). Kaplan-Meier survival estimates were adjusted for left truncation using the risk set adjustment method. Kaplan-Meier curves were truncated at 60 months.
Among the 1,630 mHSPC patients included, 1,508 patients had ≥1 mHSPC solid tissue collection date for the final analytic sample. Of the 1,508 patients, 34.2% had tumors with PTEN alterations. The mean age at diagnosis was 68.8 years. 67% of patients had Gleason Score 8–10 disease, and nearly 70% had de novo mHSPC.
The PTEN-altered group had a lower proportion of Black or African American patients (6.2% vs. 13.6%) and a lower median PSA level at diagnosis (45.7 vs. 68.7 ng/ml), compared to the PTEN-non-altered group.
Homologous recombination repair mutations (i.e., BRCA1/2 and non-BRCA) were less frequent in PTEN-altered tumors; TP53 and RB1 mutations were more frequent in PTEN-altered tumors, compared to PTEN-non-altered tumors (TP53: 48.3% vs. 33.1%; RB1: 9.9% vs. 4.4%).

The most common 1st line treatments received by patients with both PTEN- and non-PTEN-altered were ADT monotherapy and ADT + an androgen receptor pathway inhibitor (ARPI).
Overall, patients with PTEN-altered tumors had worse rwOS outcomes (median, 33.4 versus 43.5 months).

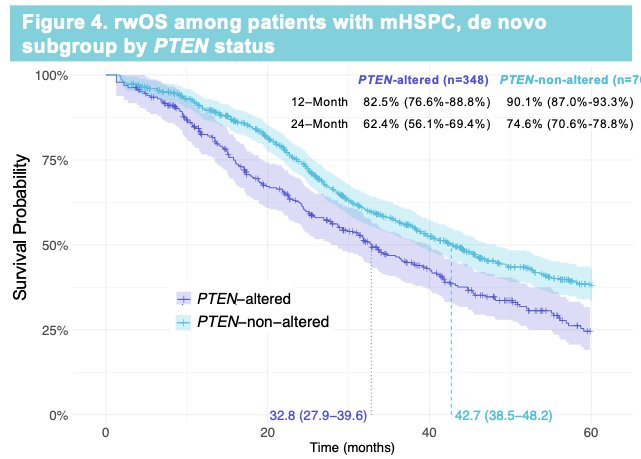
A similar trend was observed when analysis was restricted to patients with de novo mHSPC (32.8 versus 42.7 months, respectively).
Patients with PTEN-altered tumors treated with an ARPI, docetaxel, or ADT alone in the 1st line mHSPC setting appeared to have worse rwOS than those without PTEN alterations.

Dr. Rathkkopf concluded as follows:
- This study found that, among patients with mHSPC, worse survival outcomes were observed in patients with tumors harbouring PTEN alterations relative to patients with tumors without PTEN alterations.
- Future survival analyses will account for potential differences between PTEN groups, such as patient race and the co-occurrence of other biomarker alterations.
Presented by: Dana E. Rathkopf, MD, Medical Oncologist, Associate Chair, Junior Faculty Development, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Surveillance, Epidemiology, and End Results (SEER) Program. Cancer of the prostate – cancer stat facts. National Cancer Institute. Accessed April 22, 2025.
- Schoen MW, Fenton JJ, Makarov DV, et al. Trends in the use of genomic classifiers to guide prostate cancer management in the United States. JAMA Netw Open. 2024;7(3):e241970.
- Roychowdhury S, Iyer MK, Robinson DR, et al. Personalized oncology through integrative high-throughput sequencing: a pilot study. J Clin Oncol. 2013;31(15):1866–1873.
- de Bono JS, Armstrong AJ, Morris MJ, et al. Novel androgen receptor pathway inhibitors in metastatic prostate cancer: a 2024 update. Eur Urol. 2024. doi:10.1016/j.eururo.2024.12.015.
- Turnham DJ, Aguiar DJ, Eckert LB, et al. The role of MAPK signaling pathways in prostate cancer progression and therapy resistance. Cells. 2020;9(11):2342.
- Jamaspishvili T, Kaffenberger SD, Ross AE, et al. Clinical implications of PTEN loss in prostate cancer. Nat Rev Urol. 2018;15:222–234.