(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to a New Frontiers in Prostate-Specific Membrane Antigen (PSMA) Radioligand Therapy. Dr. Atish Choudhury discussed the BULLSEYE trial, which was presented earlier by Dr. Bastiaan Privé, and whether it was time to ‘break up’ with androgen deprivation therapy (ADT) in favor of radioligand therapies.
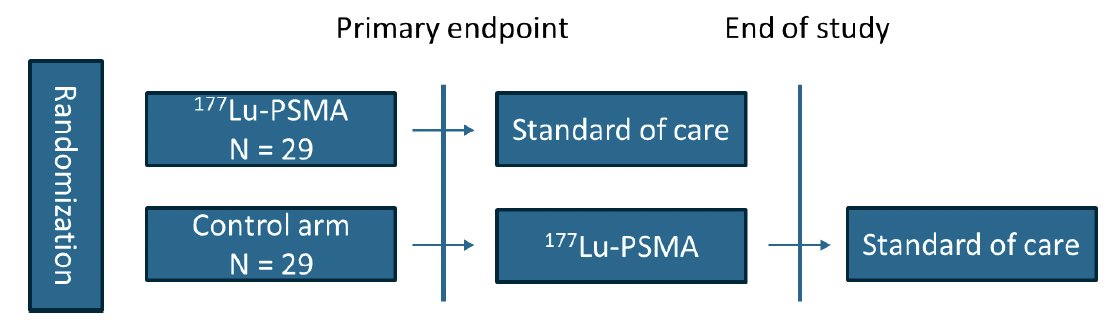
BULLESEYE is an international, open label, randomized trial of 2 (+2) cycles of 7.4 GBq 177Lu-PSMA-617 versus ‘standard of care’ of watchful waiting (i.e., postponing ADT). The study included 58 patients who were randomized 1:1. Eligible patients were those with:
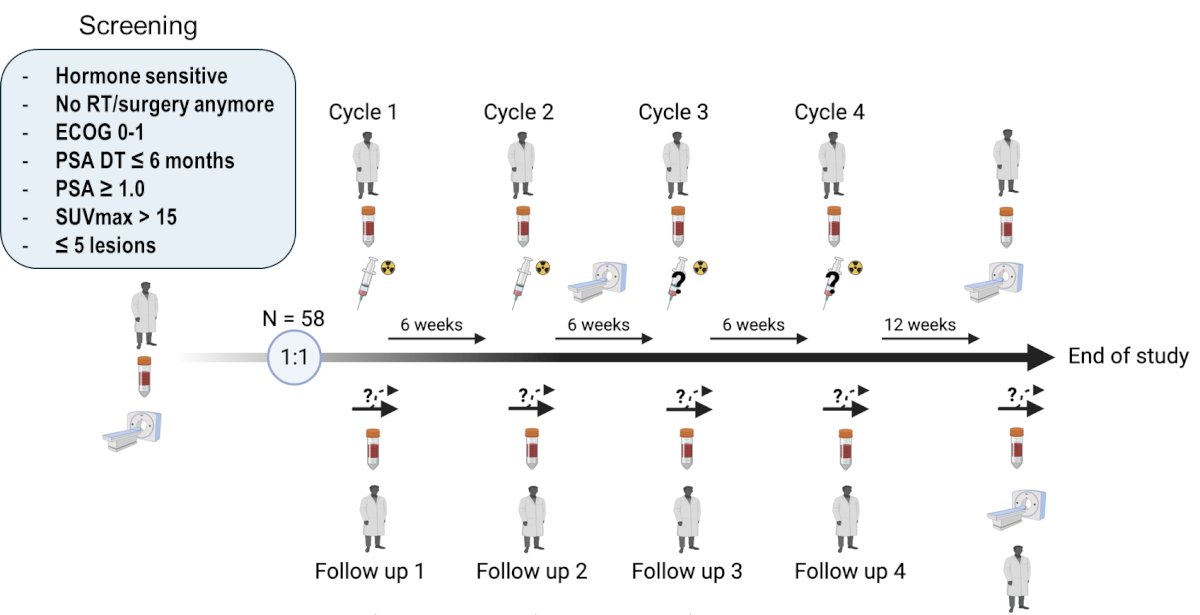
- Hormone sensitive disease
- Not eligible/ideal candidates for further pelvic radiotherapy or surgery
- PSA doubling time ≤6 months
- PSA ≥1
- SUVmax >15
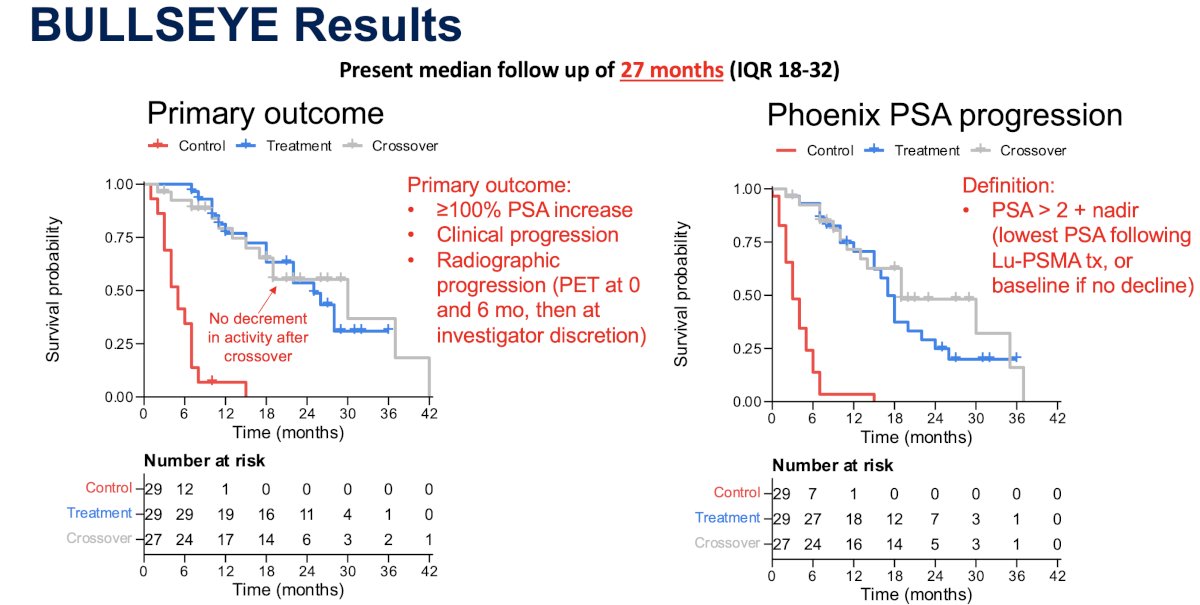
The primary study objective was disease progression, defined as a 100% increase in serum PSA levels or radiographic or clinical progression.
The trial schema with screening/follow up visits is illustrated below:
Dr. Choudhury highlighted several key features of this trial:
- This trial included a high-risk cohort of patients with a PSA doubling time ≤6 months
- The cut-off of ≤5 lesions was per PSMA PET – no conventional imaging correlate was available.
- Besides an SUVmax of >15, no biomarker selection was incorporated into the eligibility criteria
- Local treatment of oligometastases with radiotherapy or surgery was deemed not feasible due to prior treatment, the location of the metastatic lesions, or if the patient refused these treatments
- Patients in the control arm did not receive treatment for 30 weeks

At a median follow-up of 27 months, patients in the 177Lu-PSMA-617 intervention arm had superior progression-free and time to PSA progression survivals, compared to those in the control arm. However, following progression, patients in the control arm were allowed to crossover to receive 177Lu-PSMA-617, and when considering timing of receipt of 177Lu-PSMA-617 as the follow-up start time, there were no differences between the crossed over patients in the control arm and those in the intervention arm, suggesting no decrement in activity after crossover.
Of the 57 patients who received 177Lu-PSMA-617, 14 (24%) experienced a complete biochemical response (i.e., <0.1 ng/ml). Of these 14 patients, 9 had an ongoing complete response at the study cut-off date (median follow-up 27 months). Dr. Choudhury noted that identifying potential complete responders a priori is critical for optimal patient selection.
Notable grade 2 adverse events were as follows:
- Dry mouth (7%) – moderate symptoms; oral intake alterations (e.g., copious water, other lubricants, diet limited to purees and/or soft, moist foods); unstimulated saliva 0.1 to 0.2 ml/min
- Fatigue (4%) – fatigue not relieved by rest; limiting instrumental activities of daily living
- Nausea (9%) – oral intake decreased without significant weight loss, dehydration or malnutrition
Strengths and limitations of this study were as follows:
- Strengths:
- Study addresses a clinically/biologically important question
- Focus on patient-centered goal of delaying ADT use
- Randomized study design
- Limitations
- Small sample size with short follow-up
- Randomization of high-risk patients to no treatment for 30 weeks
- Non-standardized entry criteria and clinical endpoints
- Lack of conventional imaging component
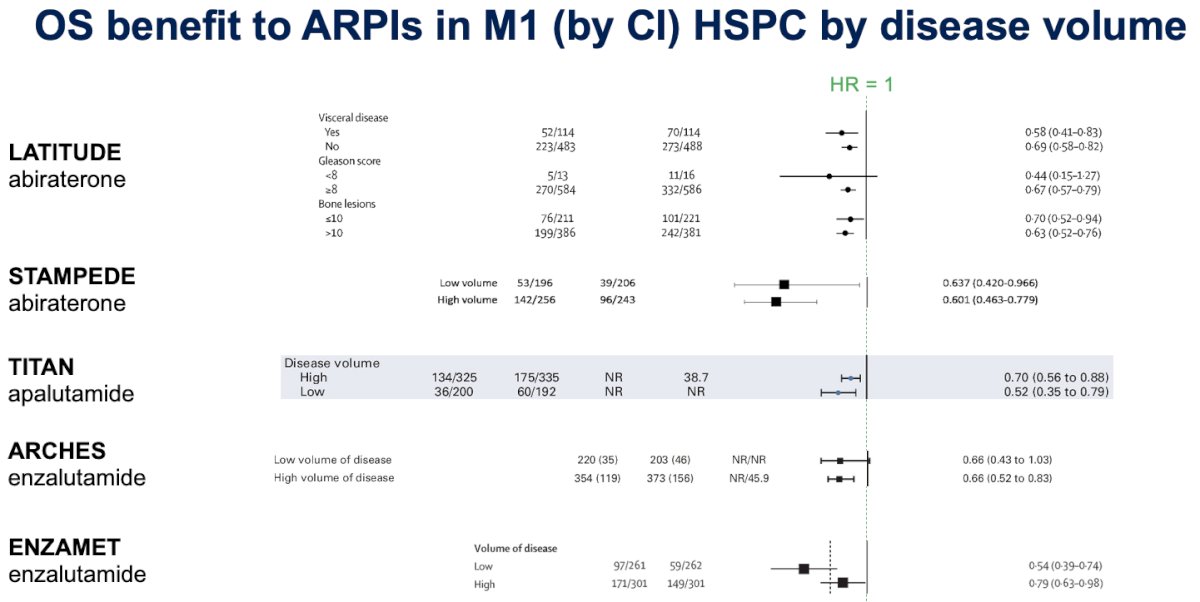
Should we forgo ADT in favor of radioligand therapy for patients with oligorecurrent mHSPC? While ADT is associated with adverse effects, including increased risks of cardiovascular disease, depression, fatigue, etc., we know that these adverse effects can be managed with medical/lifestyle interventions, are often reversible, and their overall goal is to prolong survival while minimizing lifetime adverse events and decrease the symptom burden from the cancer and its treatment. Hormone intensification with androgen receptor pathway inhibitors (ARPIs) has long been shown to improve overall survival in the 1st line mHPSC treatment setting.
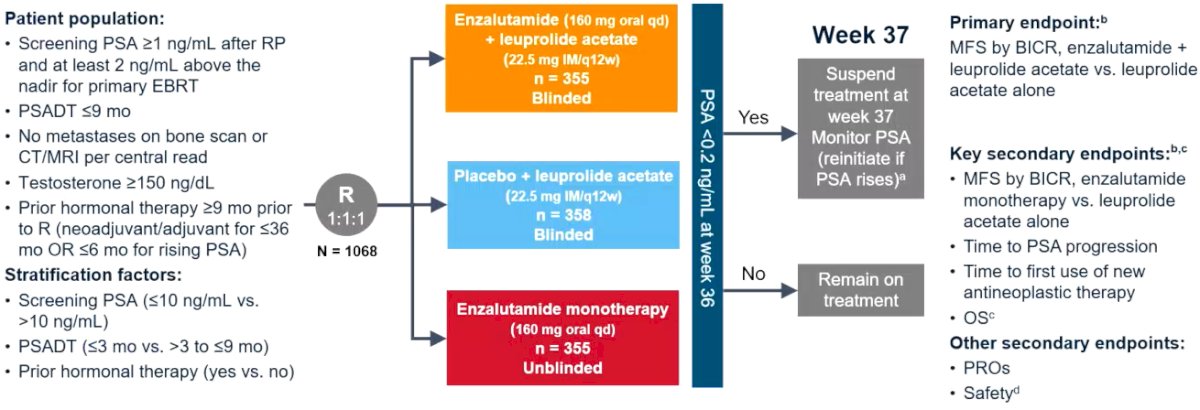
What other treatment options are available in the high-risk biochemically recurrent setting? EMBARK was a randomized phase III trial of biochemically recurrent prostate cancer patients who had evidence of high-risk disease, defined as PSA doubling time ≤9 months and a PSA level of ≥2 ng/mL above nadir following radiation therapy or ≥1 ng/mL after radical prostatectomy, with or without postoperative radiation therapy. In contrast to BULLSEYE, which included patients with ≤5 metastatic lesions on PSMA PET/CT, eligible patients for EMBARK had no evidence of metastasis on conventional imaging. Patients underwent 1:1:1 randomization as follows:
- Enzalutamide 160 mg + leuprolide acetate (blinded arm)
- Placebo + leuprolide acetate (blinded arm)
- Enzalutamide monotherapy (unblinded arm)
Notably, EMBARK was not only a trial of systemic therapy intensification, but also evaluated treatment de-intensification based on the 36-week serum PSA level, as follows:
- PSA <0.2: Treatment was suspended at week 37, and PSA was monitored with treatment reinitiated if PSA rose again
- PSA >0.2: Treatment was continued
The primary study endpoint was metastasis-free survival, assessed via blinded independent central review, in the enzalutamide + leuprolide versus leuprolide arms only. The study design is summarized below:
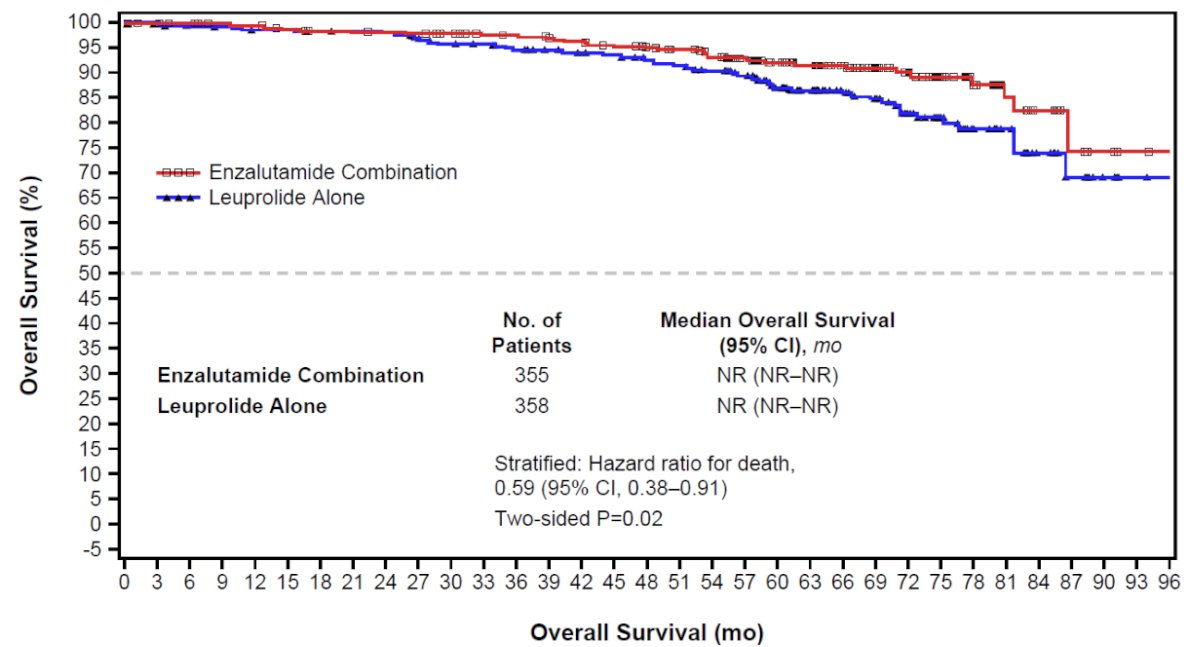
At a median follow-up of 60.7 months, patients in the combination arm of enzalutamide + leuprolide had significantly superior 5-year metastasis free survival rates (87.3% versus 71.4%; HR: 0.42, 95% CI: 0.30–0.61, p<0.001).1

PRESTO (AFT-19) was an open-label, randomized phase III trial of post-radical prostatectomy biochemically recurrent patients with a PSA doubling time ≤9 months, a serum PSA level ≥0.5 ng/ml, and, similar to EMBARK, no evidence of metastases on conventional imaging. Metastases on PSMA PET/CT or Fluciclovine F18 (Axumin®) PET were permitted. 533 patients underwent 1:1:1 randomization to a 52-week finite treatment course of:
- ADT monotherapy
- ADT + apalutamide
- ADT + apalutamide + abiraterone acetate/prednisone
With regards to the primary study endpoint of PSA progression-free survival (PSA-PFS), defined as serum PSA >0.2 ng/mL after treatment completion, both experimental arms significantly prolonged PSA-PFS, compared with the control arm:
- ADT + apalutamide: median, 24.9 months versus 20.3 months for ADT (HR: 0.52, 95% CI: 0.35–0.77, p=0.00047)
- ADT + apalutamide + abiraterone acetate/prednisone: median, 26 months versus 20 months (HR: 0.48, 95% CI: 0.32–0.71, p=0.00008)2
With regards to quality-of-life outcomes with treatment selection in the high-risk biochemically recurrent setting, Dr. Choudhury noted that there were no differences in the mean global health and fatigue scores between patients in the intervention and control arms of BULLSEYE.

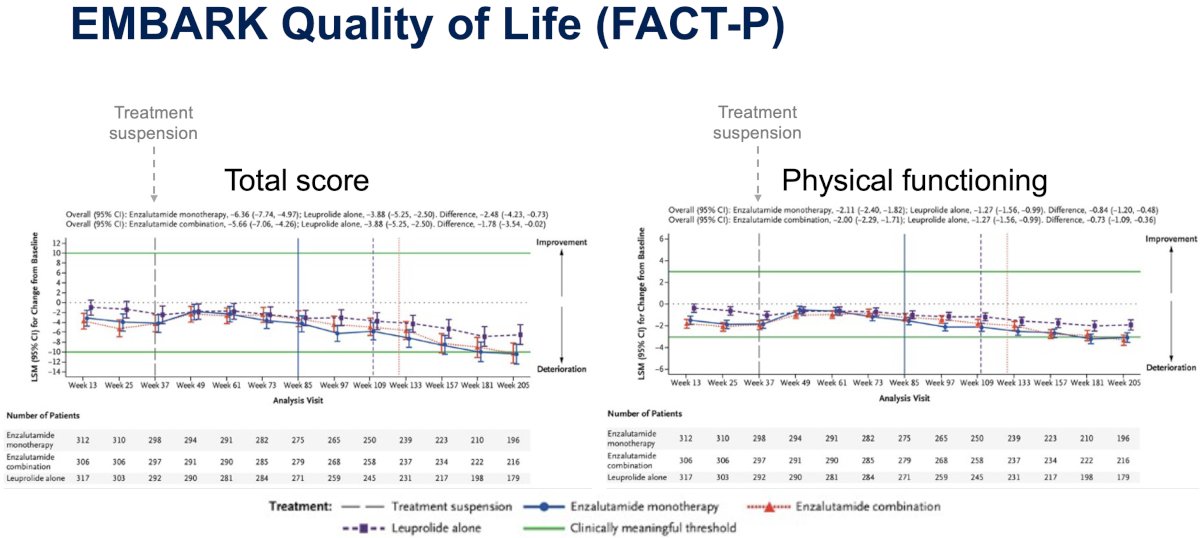
Similarly, quality-of-life, assessed using the FACT-P questionnaire, was similar for EMBARK patients across the ADT control, enzalutamide monotherapy, and enzalutamide + ADT arms.
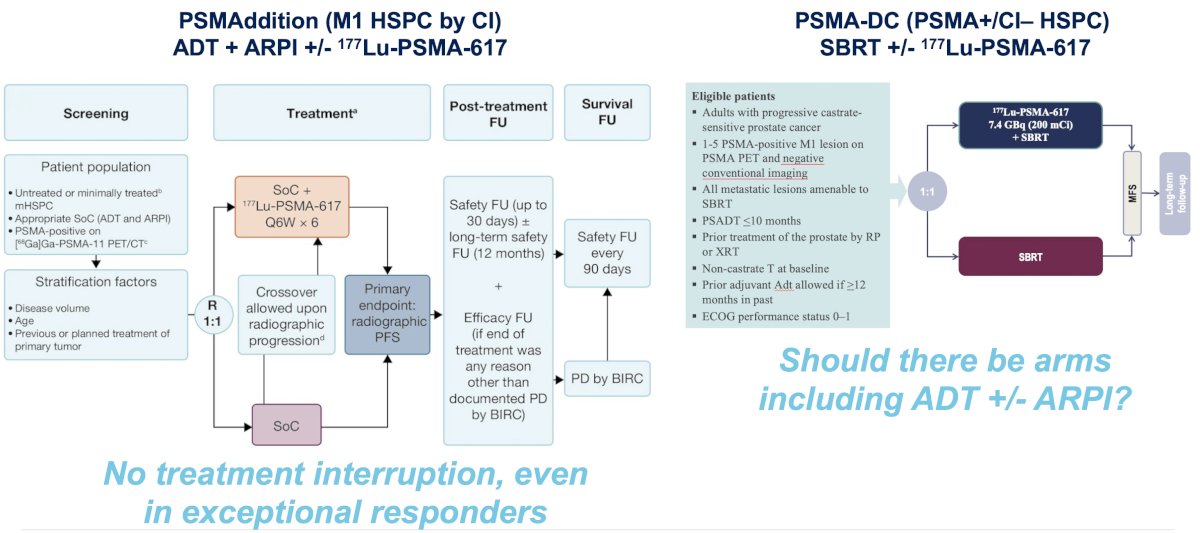
Notable ongoing clinical trials of 177Lu-PSMA-617 therapy in mHSPC include:
- PSMAddition: ADT + an androgen receptor pathway inhibitor +/- 177Lu-PSMA-617 in mHSPC patient by conventional imaging
- PSMA-DC: SBRT +/- 177Lu-PSMA-617 in PSMA-positive, conventional imaging-negative mHSPC
While these ongoing trials are promising and the results are eagerly awaited, notable limitations are as follows:
- PSMAddition: No treatment interruption, even in exceptional responders
- PSMA-DC: Should there be an arm incorporating ADT +/- an ARPI?
Is it time to break up with ADT? Dr. Choudhury argued that not yet, and, at least, not in everyone. Upfront ADT-free strategies warrant further study in randomized trials that incorporate:
- Prostate cancer-related clinical endpoints (radiographic progression-free survival [rPFS], OS)
- Non-prostate cancer related clinical endpoints (non-cancer specific survival, cardiovascular events, falls/fractures, metabolic changes, secondary malignancies)
- Patient-centered endpoints (quality-of-life, ADT-free survival, lifetime ADT exposure, capture lifetime symptom burden from cancer/treatment)
He argued that molecular/genomic biomarkers should be integrated into trial design to identify predictive markers for benefit (or lack of benefit) from ADT-free strategies.
His key takeaway points/conclusions were as follows:
- Intensified ADT remains the favored standard of care for low volume M1 mHSPC by conventional imaging, and a reasonable standard of care for high-risk biochemically recurrent patients, irrespective of PSMA PET findings
- 177Lu-PSMA-617 is safe and well-tolerated in oligometastatic mHSPC defined by PSMA PET imaging, with clinical activity allowing delay in ADT that warrants further study.
- Clinical features, patient preferences, and potentially molecular biomarkers may help guide optimal patient selection for upfront ADT-free strategies.
Presented by: Atish Dipankar Choudhury, MD, PhD, Assistant Professor of Medicine, Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Freedland SJ, de Almeida Luiz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2023; 389(16): 1453–65.
- Aggarwal R, Heller G, Hillman DW, et al. PRESTO: A Phase III, Open-Label Study of Intensification of Androgen Blockade in Patients With High-Risk Biochemically Relapsed Castration-Sensitive Prostate Cancer (AFT-19). J Clin Oncol. 2024; 42(10): 1114–23.