(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Poster Session: Genitourinary Cancer - Prostate, Testicular, and Penile Cancer. Dr. Alan Bryce presented Poster 5041: Cardiovascular (CV) event risk in patients with metastatic castration-resistant prostate cancer (mCRPC) treated with enzalutamide (ENZA) or abiraterone acetate (AA) in the United States (US).
Dr. Bryce and colleagues presented a real-world, comparative causal inference study evaluating cardiovascular (CV) risk among chemotherapy-naïve patients with metastatic castration-resistant prostate cancer (mCRPC) treated with abiraterone acetate (AA) or enzalutamide. Prior studies have suggested that AA may be associated with a higher risk of CV event-related hospitalizations compared to enzalutamide in this population.1
To further investigate this, the investigators analyzed a large US database to assess CV event risk following treatment initiation and stratified outcomes based on patients’ history of cardiovascular disease (CVD). Using US Medicare fee-for-service claims from January 2010 to December 2022, the investigators identified chemotherapy-naïve patients aged ≥65 years with mCRPC who initiated treatment with enzalutamide or abiraterone acetate between September 2014 and May 2017.
The primary endpoint was the incidence of 4-point major adverse cardiovascular events (MACE-4), defined as a composite of acute myocardial infarction (AMI), stroke, unstable angina or revascularization, and heart failure. Additional outcomes included atrial fibrillation (AFib), venous thromboembolism (VTE), and all-cause mortality.
The study population consisted of chemotherapy-naïve patients aged ≥65 years with mCRPC, identified from the CMS Medicare fee-for-service database. All patients-initiated treatment with either Enzalutamide or Abiraterone acetate (AA) between September 10, 2014, and May 31, 2017, and were followed through December 31, 2022. Patients were stratified by CV risk, based on the presence or absence of prior CVD.
To adjust for baseline differences, patient groups were propensity score matched (PSM), with covariate balance assessed using standardized mean differences (SMD). Cause-specific Cox proportional hazards models were employed to compare CV risk between intention-to-treat cohorts, accounting for death as a competing risk. Subgroup analyses were stratified by history of CVD. A sensitivity analysis was also performed using a 5-point MACE definition (MACE-4 plus cardiovascular-related death)
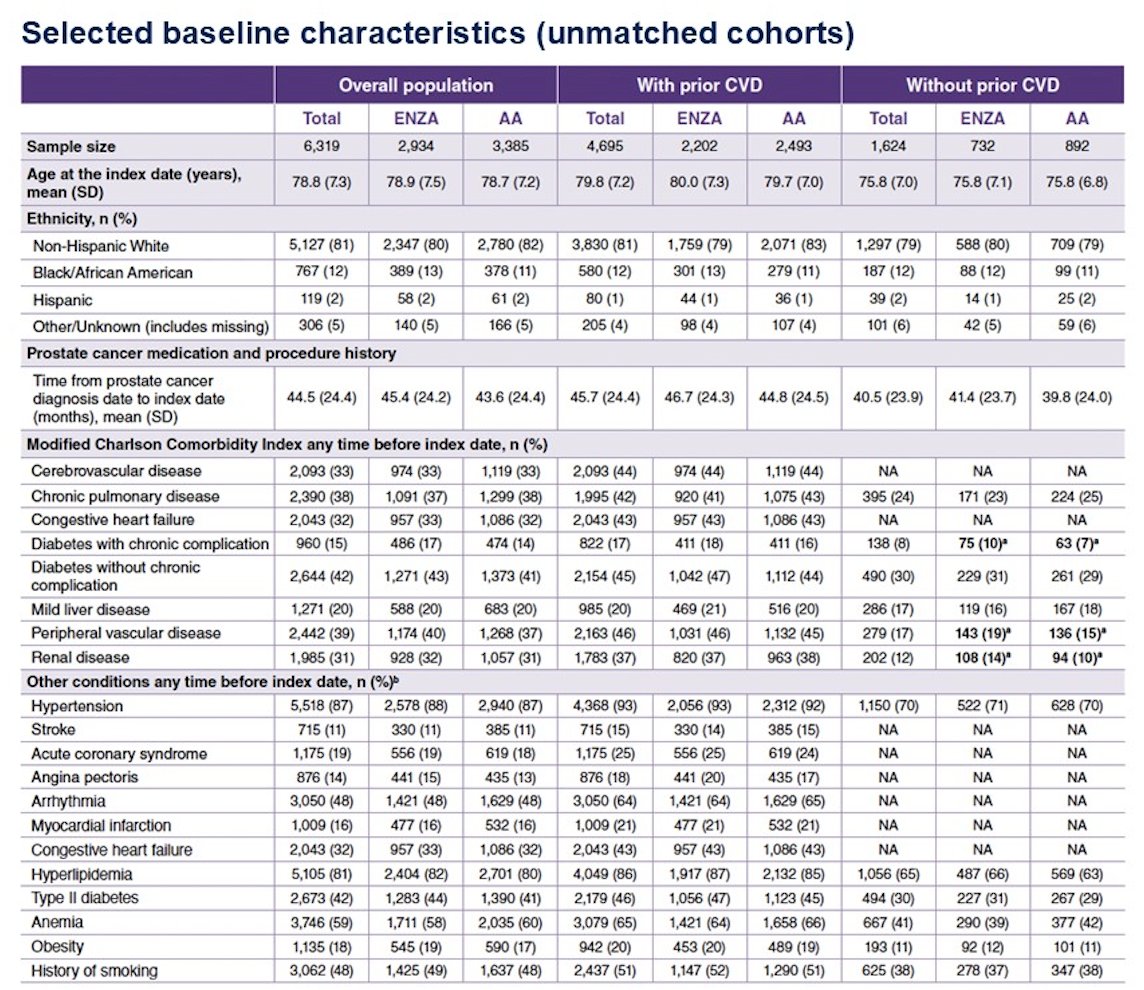
A total of 6,319 patients with mCRPC were included in the study (Enzalutamide: n=2,934; AA: n=3,385). Baseline characteristics were well balanced between treatment groups in the overall population and among patients with prior CVD (SMD < 0.1). Among patients without prior CVD, those treated with ENZA had a higher prevalence of renal disease (SMD = 0.127), peripheral vascular disease (SMD = 0.113), and diabetes with chronic complications (SMD = 0.113). Baseline characteristics of the unmatched cohorts are shown below.
After propensity score matching, 2,913 patients were included in each treatment group. Baseline characteristics were well balanced between cohorts and by CV risk group.
Patients treated with abiraterone had a significantly higher risk of experiencing major adverse cardiovascular events (MACE-4), particularly unstable angina or revascularization, compared to those treated with enzalutamide. The abiraterone cohort also had a higher incidence of atrial fibrillation and venous thromboembolism. These findings remained consistent across subgroups stratified by CVD history and were confirmed in sensitivity analyses using the expanded MACE-5 definition.
Additionally, all-cause mortality was significantly higher among patients treated with AA regardless of CVD history. In those with prior CVD, the hazard ratio was 1.14 (95% CI: 1.07–1.21; P=0.0001), and in those without CVD, HR was 1.13 (95% CI: 1.07–1.19; P=0.0001) as illustrated below.

Dr. Bryce concluded with the following key takeaways:
- This matched analysis of US Medicare beneficiaries showed a higher risk of 4-point MACE, atrial fibrillation, and venous thromboembolism in patients with mCRPC treated with abiraterone acetate compared to enzalutamide.
- These increased risks were consistent in both the overall cohort and in patients with a history of cardiovascular disease.
- All-cause mortality was also higher in patients receiving abiraterone, regardless of cardiovascular history.
- The baseline comorbidities and the overall findings highlight the need to carefully consider cardiovascular risk when selecting systemic therapies for patients with mCRPC.
Presented by: Alan Haruo Bryce, MD, Chief Clinical Officer, City of Hope Cancer Center Pheonix, Phoenix, AZ
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References: