(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer rapid oral abstract session and a presentation by Dr. Rikke Eefsen discussing the CheckPRO trial, a randomized phase 2 trial of nivolumab and ipilimumab with or without stereotactic body radiation therapy in metastatic castration-resistant prostate cancer (mCRPC). mCRPC is among the leading causes of cancer related mortality in men worldwide, with treatment options including chemotherapy and androgen receptor pathway inhibitors. However, prostate cancer is considered an immunosuppressive “cold” tumor. As of today, immune checkpoint inhibitors (trials: CheckMate-650, KEYNOTE-199, ICE-PAC, etc) have not demonstrated effect in patients with mCRPC. The use of stereotactic body radiation therapy may increase the expression of tumor associated antigens and enhance potential immune responses following systemic therapy.
Patients with mCRPC, who had previously progressed on at least one taxane regimen and one androgen receptor pathway inhibitor, were screened for the CheckPRO trial. Eligible patients were randomized to receive either ipilimumab 1 mg/kg and nivolumab 3 mg/kg every 4 weeks for the first 12 weeks followed by nivolumab monotherapy 480 mg every 4 weeks for up to 52 weeks (Arm B), or the same immune checkpoint inhibitor with stereotactic body radiation therapy to a metastasis, 24 Gy in 3 fractions (Arm A):
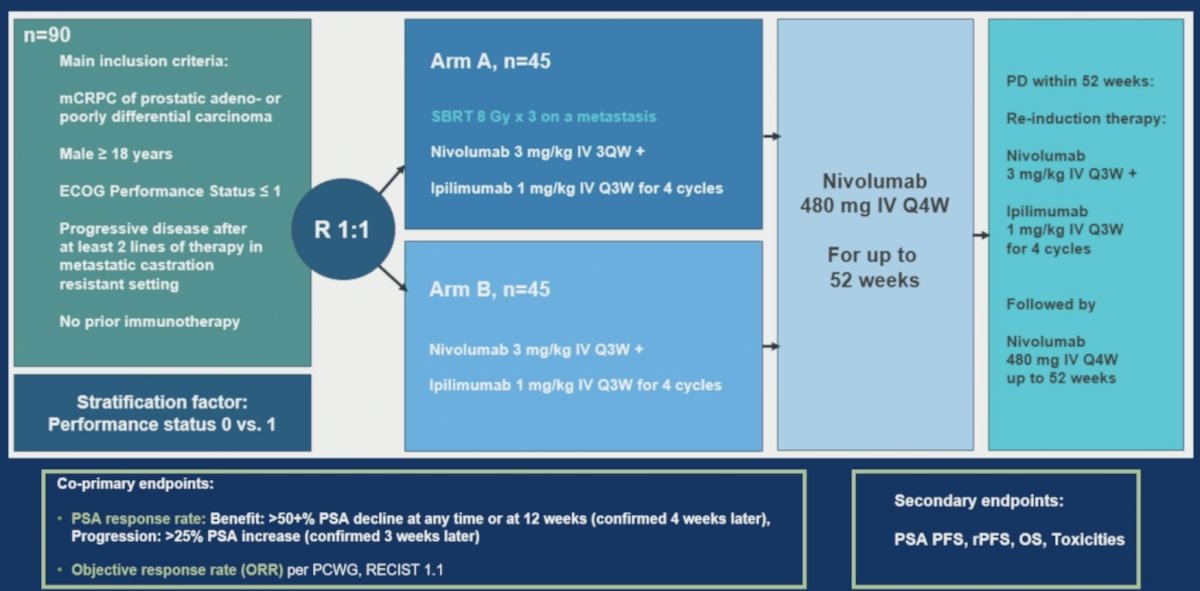
The co-primary endpoints were PSA response rate, defined as a ≥50% decline in PSA compared to baseline, confirmed after ≥4 weeks, and objective response rate according to modified RECIST 1.1 and PCWG3. Secondary endpoints included overall survival, radiologic progression free survival, and toxicity.
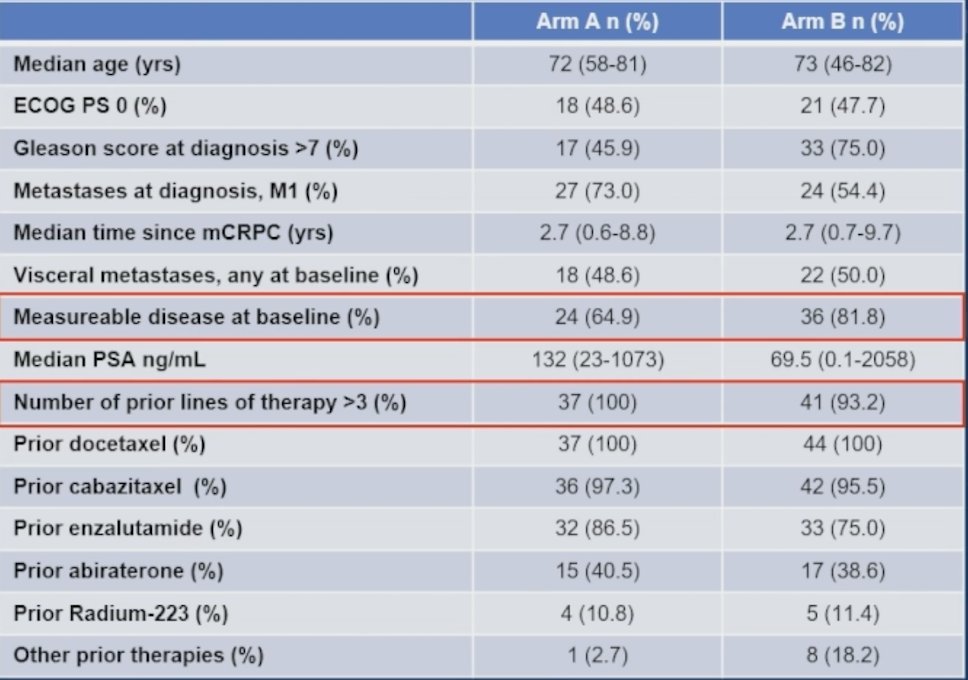
Between November 2019 and January 2024, 91 patients were randomized in the CheckPRO trial. A total of 81 patients received at least one treatment cycle and were eligible for evaluation, with the following baseline demographics:
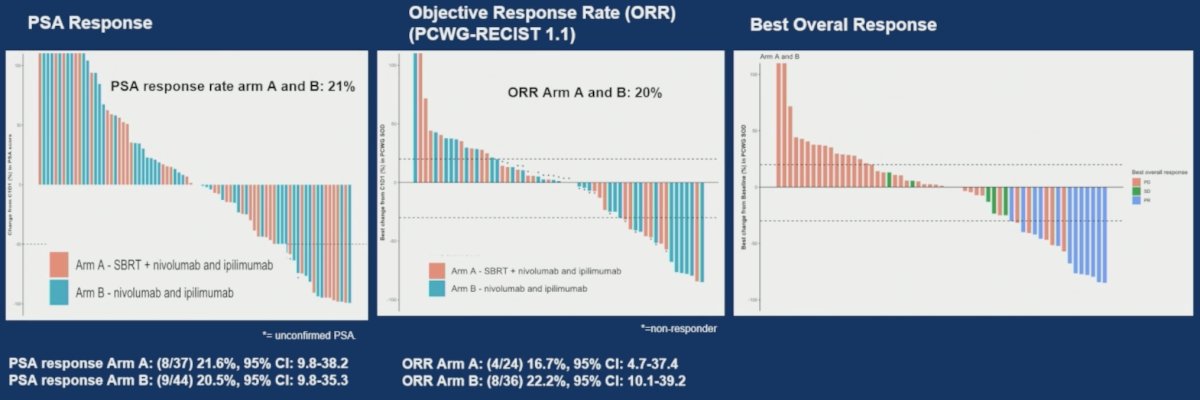
The confirmed PSA response rate was 21.6% in arm A and 20.5% in arm B. The objective response rate was 16.7% (95% CI [4.7-37.4] %) and 22.2% (95% CI 10.1-39.2) in arm A and B, respectively:
The PSA progression free survival in Arm A was 2.6 months versus 2.5 months in Arm B, and radiologic progression free survival was 2.1 months and 1.9 months in arm A and B, respectively. The median overall survival was 10.2 months in arm A and 9.2 in arm B:

Serious adverse events related to immune checkpoint inhibitors occurred in 29.7% of patients in arm A and 31.8% in arm B.
Dr. Eefsen concluded this presentation of the CheckPRO trial with the following take home points:
- Responses were demonstrated in patients with mCRPC treated with combination immune checkpoint inhibitor, however progression free survival was short and treatment-related toxicity was significant
- While the addition of stereotactic body radiation therapy was safe, it did not improve treatment outcomes in this study
- Further analyses are ongoing to identify patients with mCRPC who are most likely to respond to immune checkpoint inhibitors
Presented by: Rikke L. Eefsen, MD, PhD, Department of Oncology, Experimental Cancer Therapy Unit, Herlev, Denmark
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.