(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer rapid oral abstract session and a presentation by Dr. Praful Ravi discussing an ICECaP individual patient-data meta-analysis of randomized controlled trials assessing docetaxel with ADT and radiotherapy for high-risk localized prostate cancer. Radiotherapy + long term ADT is a standard of care for treatment of high risk localized prostate cancer. However, there is no established role for the use of docetaxel with ADT and radiotherapy for high-risk localized prostate cancer, with mixed results seen in prior RCTs. Prior work from ICECaP1 has shown that patients with very high-risk disease (ie 2 or 3 risk factors: Gleason ≥8, PSA >20 ng/mL, ≥cT3 and/or cN1) have the poorest outcomes with radiotherapy + ADT for high-risk localized prostate cancer, with 5-year metastasis-free survival of ≤80%. Dr. Ravi and colleagues aimed to perform an IPD meta-analysis of the role of docetaxel with ADT + radiotherapy for high-risk localized prostate cancer and specifically evaluate whether patients with very high-risk disease benefit from the addition of docetaxel.
IPD from RCTs involving patients with high-risk localized prostate cancer treated with radiotherapy + ADT +/- docetaxel collated by ICECaP were analyzed. “High-risk” disease was defined as presence of 1 risk factor, and “very high-risk” disease as 2-3 risk factors and/or cN1 disease. The primary outcomes of interest were metastasis-free survival and overall survival. Hazard ratios for metastasis-free survival and overall survival were estimated using Cox regression, stratified by year of randomization and adjusted for age at randomization and ECOG performance status. 5-year metastasis-free survival and overall survival rates were estimated using the Kaplan-Meier method. Subgroup analyses were performed according to the severity of disease (high- and very high-risk), and p-values for interaction were tested using the likelihood ratio test.
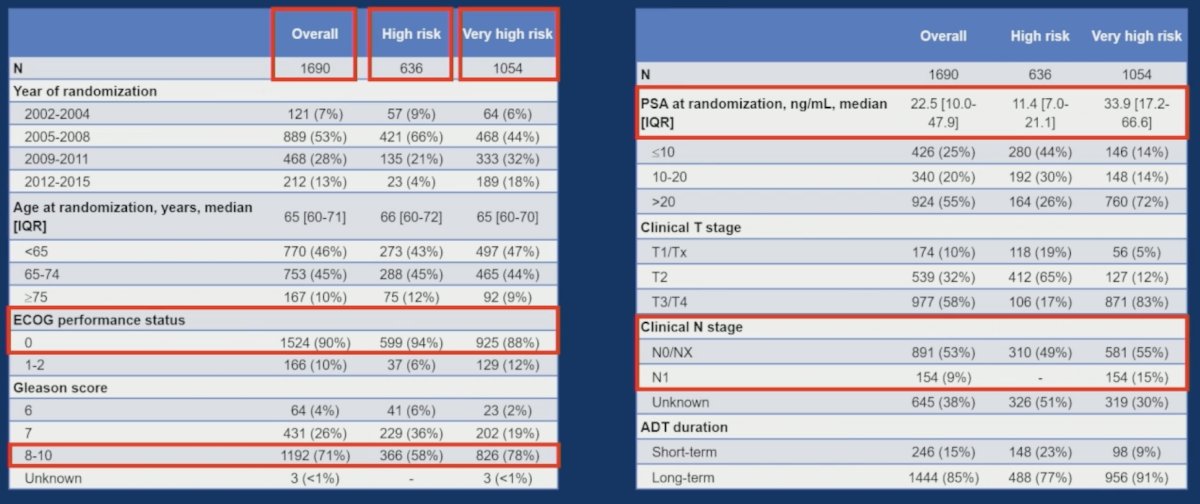
There were 1,690 patients treated on four RCTs (GETUG-12, DFCI 05-043, STAMPEDE, RTOG-0521) between 2002-2015, eligible. The median age was 65 years (IQR 60-71), median PSA was 23 ng/mL (IQR 10-48), 154 (9%) patients had cN1 disease, and 1,444 (85%) received long-term ADT with radiotherapy. The median follow-up was 10 years (range: <1-15):
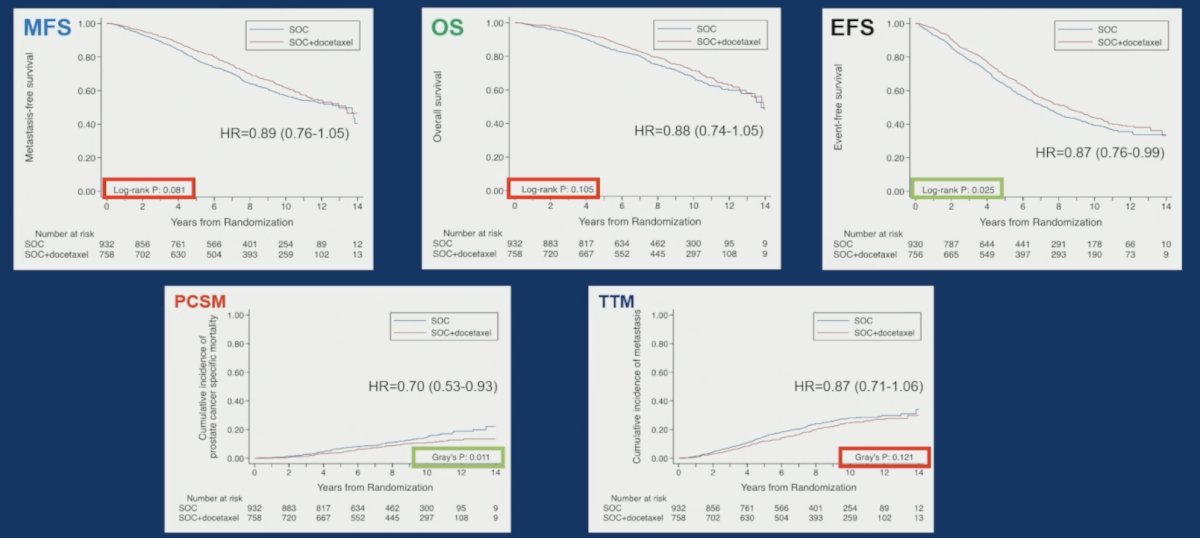
Overall, the addition of docetaxel to radiotherapy + ADT was not associated with a significant benefit in metastasis-free survival (HR 0.89 [0.76-1.05], p = 0.160) or overall survival (HR 0.88 [0.74-1.05], p = 0.167). There was benefit for adding docetaxel to radiotherapy + ADT for event free survival (HR 0.76, 95% 0.76-0.99) and prostate cancer specific mortality (HR 0.70, 95% CI 0.53-0.93:
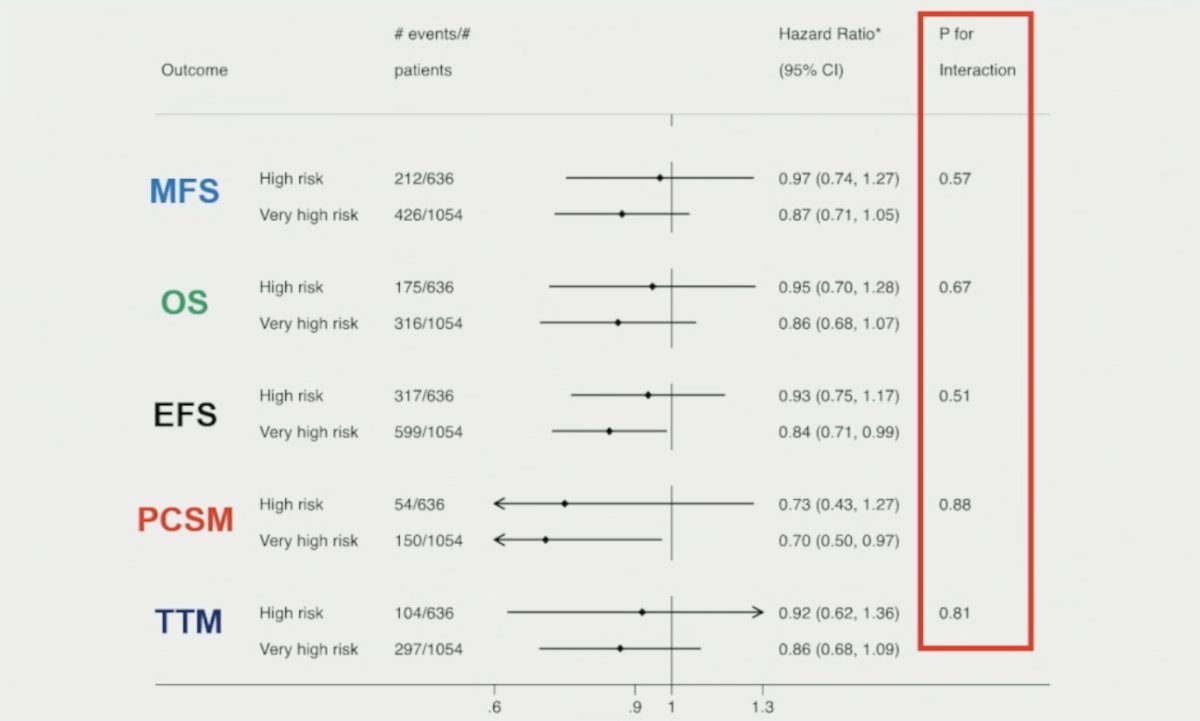
Though there was some evidence for favoring docetaxel in patients with very high-risk disease (n = 1,054: metastasis-free survival HR 0.87 [0.71-1.05]; overall survival HR 0.86 [0.68-1.07]) compared to high-risk disease (n = 636: metastasis-free survival HR 0.97 [0.74-1.27]; overall survival HR 0.95 [0.70-1.28]), there was no evidence of a significant difference in treatment effect by risk group (p-interaction >0.1):
The 5-year metastasis-free survival and overall survival rates in patients with high- and very high-risk disease, stratified by receipt of docetaxel, are shown in the following table:

Several limitations related to this analysis include the following:
- Most men were treated before 2010 and may not have received contemporary radiotherapy
- There was a relatively small number of patients with cN1 disease (<10%)
- SPCG-13 trial data were not included
- The current standard of care for very high risk patients is ADT + abiraterone with radiotherapy
Dr. Ravi concluded his presentation discussing an ICECaP individual patient-data meta-analysis of randomized controlled trials assessing docetaxel with ADT and radiotherapy for high-risk localized prostate cancer with the following take home points:
- In this IPD meta-analysis, the addition of docetaxel to radiotherapy and long term ADT for high risk localized prostate cancer did not significantly improve metastasis free survival or overall survival, though there was a modest but significant benefit in terms of event free survival and prostate cancer specific mortality
- While there was evidence of a potentially greater benefit for docetaxel in patients with ICECaP very high risk disease, there was not a significant interaction by risk group
- Biomarker evaluation within this group may identify those who are candidates for treatment intensification with docetaxel, with radiotherapy + ADT (+/- androgen receptor pathway inhibitors) in high-risk localized prostate cancer
Presented by: Praful Ravi, MB, BChir, MRCP, Dana-Farber Cancer Institute, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References: