(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Nicolas Sayegh discussing the additive clinical utility of tissue biomarkers of microsatellite instability status and tumor mutational burden to predict immune checkpoint inhibitor effectiveness for real-world patients with metastatic castration-resistant prostate cancer (mCRPC). FoundationOneCDx supports two FDA-approved biomarkers to guide treatment decisions for immune checkpoint inhibitor for patients with mCRPC: microsatellite instability status and tumor mutational burden. Microsatellite instability-high and tumor mutational burden-high (10+ mut/MB) have strongly overlapping prevalence. As such, Dr. Sayegh and colleagues sought to better characterize immune checkpoint inhibitor outcome associations of tumor mutational burden-high/non- microsatellite instability-high population and relative effectiveness of taxanes and immune checkpoint inhibitor among patients who received these agents in sequence.
Following a prespecified analysis plan, this study used the nationwide (US-based) de-identified Flatiron Health-Foundation Medicine mCRPC clinico-genomic database, with data originating from ~280 US cancer clinics (~800 sites of care). Inclusion criteria included patients with mCRPC treated with single-agent anti-PD(L)1 therapy in the Flatiron Health network between January 1, 2011, and March 30, 2024. This study used the microsatellite instability and tumor mutational burden algorithms from the tissue based FoundationOneCDx. Time to next treatment and overall survival were assessed with Kaplan-Meier plots and in multivariable Cox models adjusted for ECOG performance score, socioeconomic status, prior treatment history, and baseline PSA. Among patients who received taxanes in a prior line of therapy, the effectiveness (time to next treatment 1 versus time to next treatment 2) of taxane and immune checkpoint inhibitor was compared.
Among 2,995 prostate cancer tissue specimens in the database, 95 (3.1%) were microsatellite instability-high and 142 (4.7%) were tumor mutational burden-high. There were 94 (3.1%) microsatellite instability-high and tumor mutational burden-high, 1 was microsatellite instability-high and tumor mutational burden-low, and 48 (1.6%) were tumor mutational burden-high and not microsatellite instability-high:
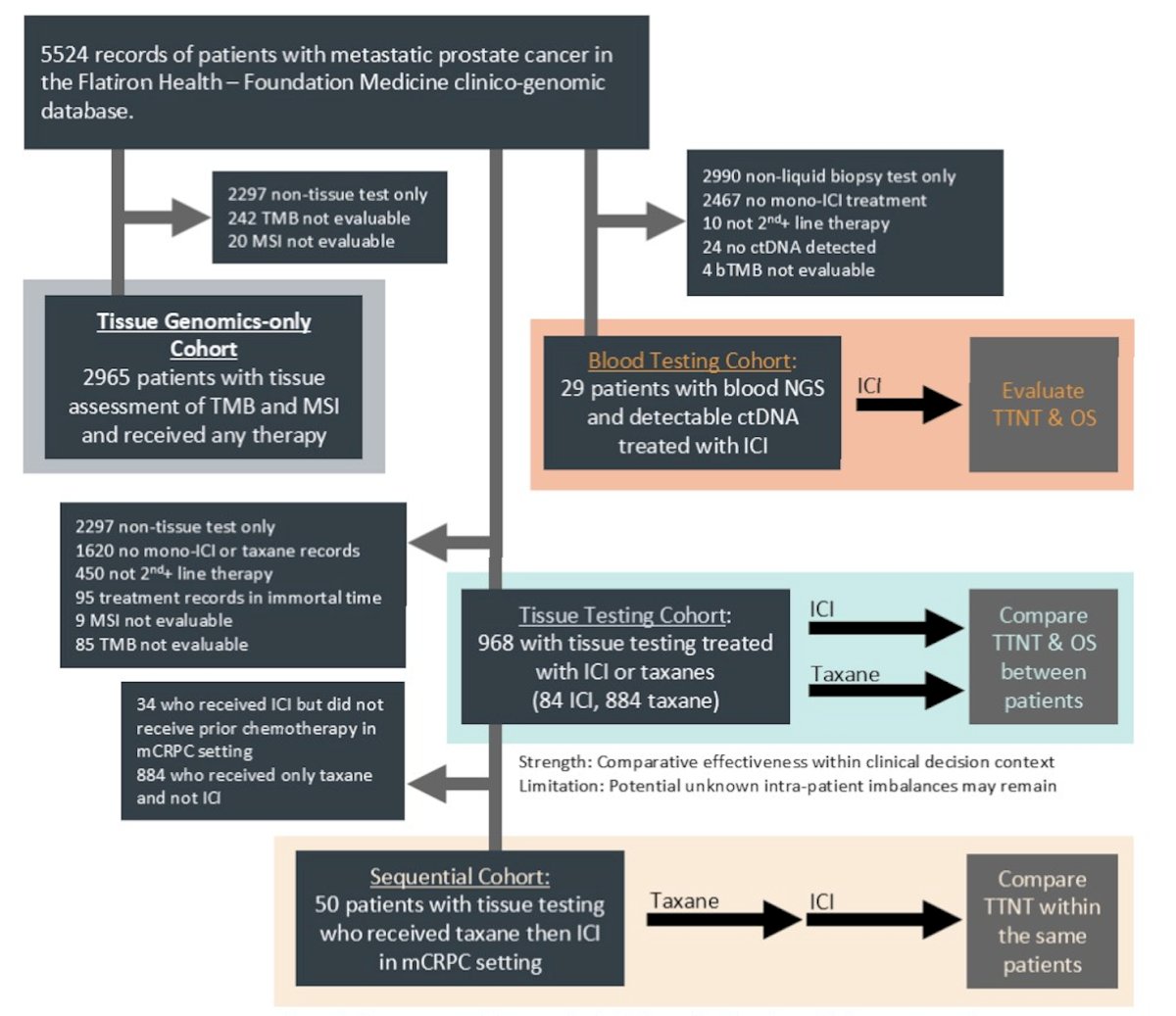
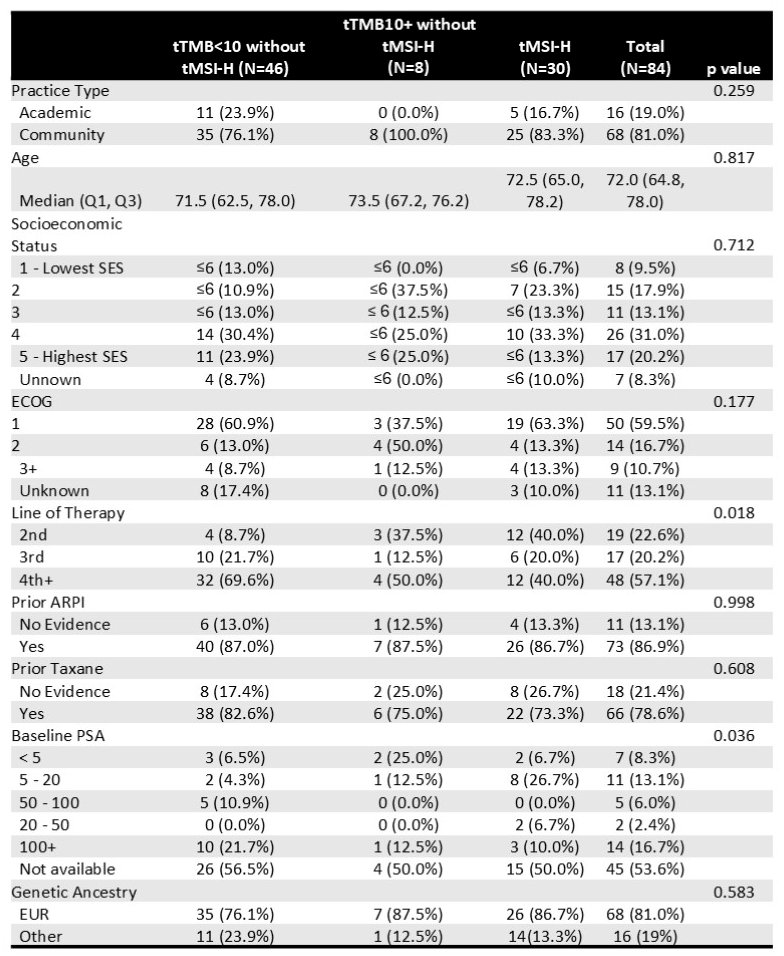
Among these, 84 patients with mCRPC were treated with immune checkpoint inhibitor and met inclusion criteria, including microsatellite instability-high and tumor mutational burden-high (n = 30), non-microsatellite instability-high and tumor mutational burden-high (n = 8), and non-microsatellite instability-high and tumor mutational burden-low (n = 46):
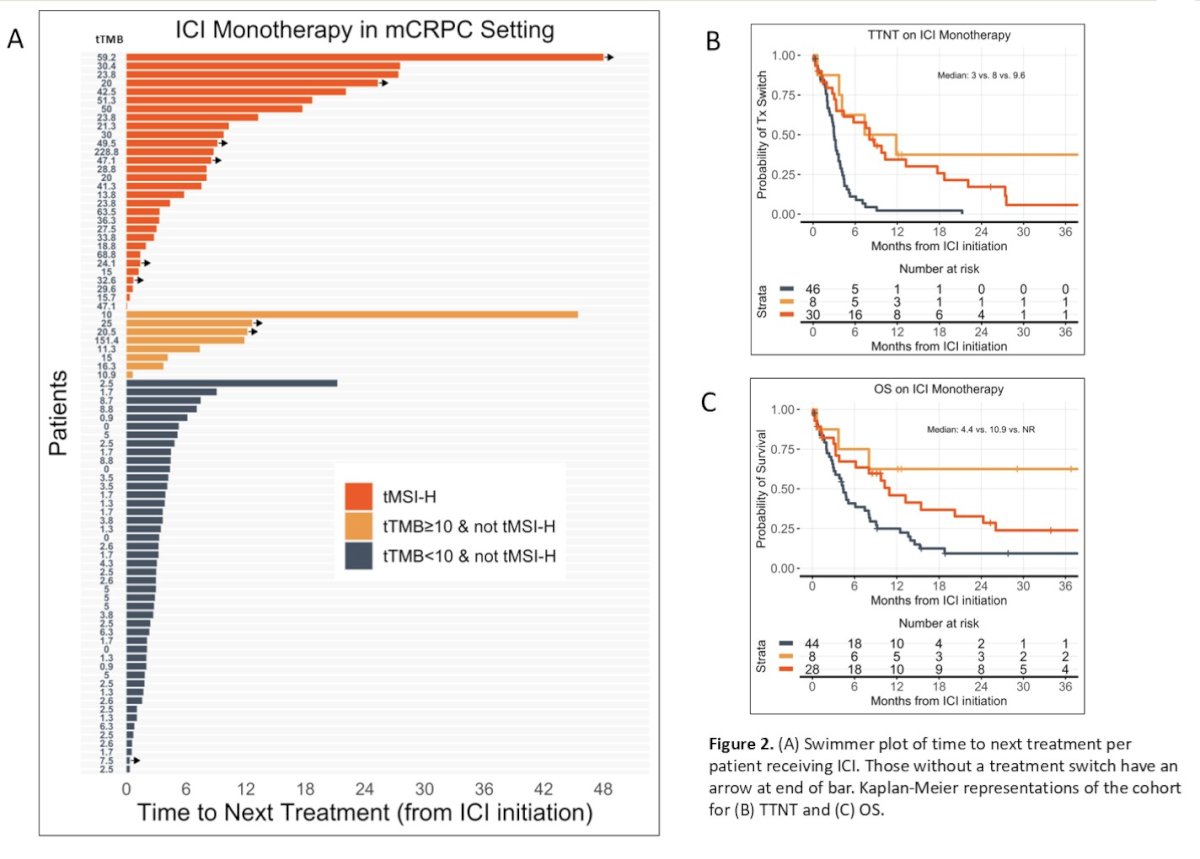
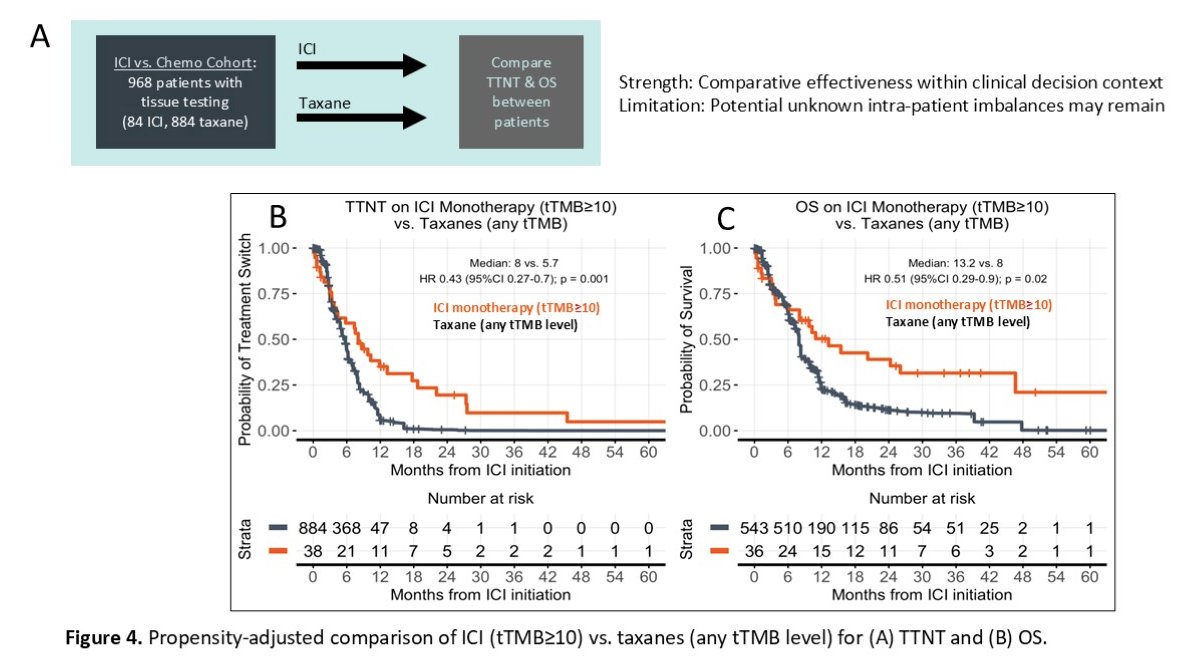
The respective median time to next treatment on immune checkpoint inhibitor were 8.0, 9.6, versus 3 months. The respective median overall survival from initiation of immune checkpoint inhibitor was 10.9 versus not reached versus 4.4 months. In multivariable models evaluating immune checkpoint inhibitor only, compared to non-microsatellite instability-high and tumor mutational burden-low, the microsatellite instability-high and tumor mutational burden-high group had more favorable time to next treatment (HR 0.20, 95% CI: 0.10 – 0.41, p < 0.001) and overall survival (HR 0.33, 95% CI 0.16 – 0.70, p = 0.004), and the non-microsatellite instability-high and tumor mutational burden-high group also had more favorable time to next treatment (HR 0.13, 95% CI 0.04 – 0.45, p = 0.002) and overall survival (HR 0.20, 95% CI 0.05 – 0.75, p = 0.017):
There were 50 of the 84 (60%) patients treated with immune checkpoint inhibitor that had prior mCRPC taxane treatment. Better time to next treatment 2 on subsequent immune checkpoint inhibitor versus prior taxane was observed for microsatellite instability-high (HR 0.49, 95% CI 0.23 – 1.01, p = 0.051) and tumor mutational burden-high (HR 0.54 95% CI 0.30 – 0.98, p = 0.044), but the opposite was true for non-microsatellite instability-high and tumor mutational burden-low subgroups, with significant treatment interactions for each (p = 0.0018, p = 0.00052):
Dr. Sayegh concluded his presentation discussing the additive clinical utility of tissue biomarkers of microsatellite instability status and tumor mutational burden to predict immune checkpoint inhibitor effectiveness for real-world patients with mCRPC with the following take home points:
- This study further validates the clinical relevance of tumor microsatellite instability and tumor mutational burden as predictive biomarkers of immune checkpoint inhibitor monotherapy in mCRPC and add validity to blood microsatellite instability testing when tissue is unavailable
- Although patients with tumor microsatellite instability-high and tumor mutational burden-high prostate cancer make up a small proportion of the general prostate cancer population (~4.5%), when present, these molecular features can predict significant immune checkpoint inhibitor benefit, and immune checkpoint inhibitors should be considered as a later line of therapy given the tumor-agnostic approvals of pembrolizumab in this setting
Presented by: Nicolas Sayegh, MD, Huntsman Cancer Institute, University of Utah Health Care, Salt Lake City, UT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Dissecting Tumor Mutational Burden and Microsatellite Instability in mCRPC: Differential Responses to Immune Checkpoint Inhibitors - Nicolas Sayegh