(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer rapid oral abstract session and a presentation by Dr. Eric Bent discussing results of the phase II Metacure trial assessing intensified hormonal blockade with stereotactic body radiotherapy in PSMA-PET detected oligometastatic prostate cancer. Metastasis directed therapy with stereotactic body radiotherapy is a standard of care in patients with oligometastatic hormone-sensitive prostate cancer (HSPC) and can delay the use of ADT. Combining stereotactic body radiotherapy with a defined period of systemic therapy may lead to durable control of oligometastatic disease and is often used in this setting, however, the optimal intensity and duration of hormonal blockade with stereotactic body radiotherapy remains unclear.
Metacure is a multi-center, multi-arm randomized phase 2 trial that tests novel systemic therapies in the context of a multimodality approach, including stereotactic body radiotherapy to oligometastatic sites. The B2 and B2 expansion cohorts of Metacure tested stereotactic body radiotherapy +/- salvage radiotherapy to prostate bed/nodes with time-limited ADT + androgen receptor pathway inhibitor hormonal blockade in patients with PSMA-PET detected metachronous oligometastatic HSPC. Eligible patients had biochemical recurrence or persistence (PSA >0.2 ng/mL) after prostatectomy with metastases treatable within max 3 radiotherapy plans. Cohort B2 randomized patients to metastasis-directed stereotactic body radiotherapy with either 10 months of ADT + apalutamide + abiraterone acetate + prednisone or ADT + apalutamide. In the B2 expansion cohort patients received 6 months of ADT + apalutamide with stereotactic body radiotherapy:
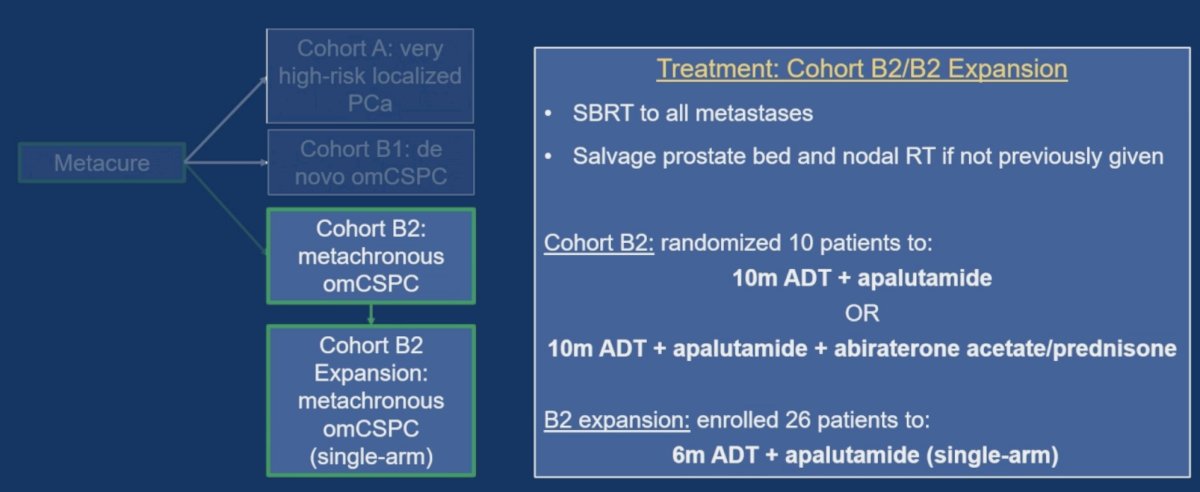
The primary endpoint was proportion of patients with undetectable PSA (PSA <0.1 ng/mL) at 12 months from treatment start and with recovered testosterone. Secondary objectives included PSA<0.1 ng/mL at 24 months, time to PSA progression (PSA 0.2 ng/mL), time to testosterone recovery, radiographic progression free survival, and progression free survival (PSA, radiographic, or clinical progression or death). The study schema for cohort B2 and cohort B2 expansion is as follows:

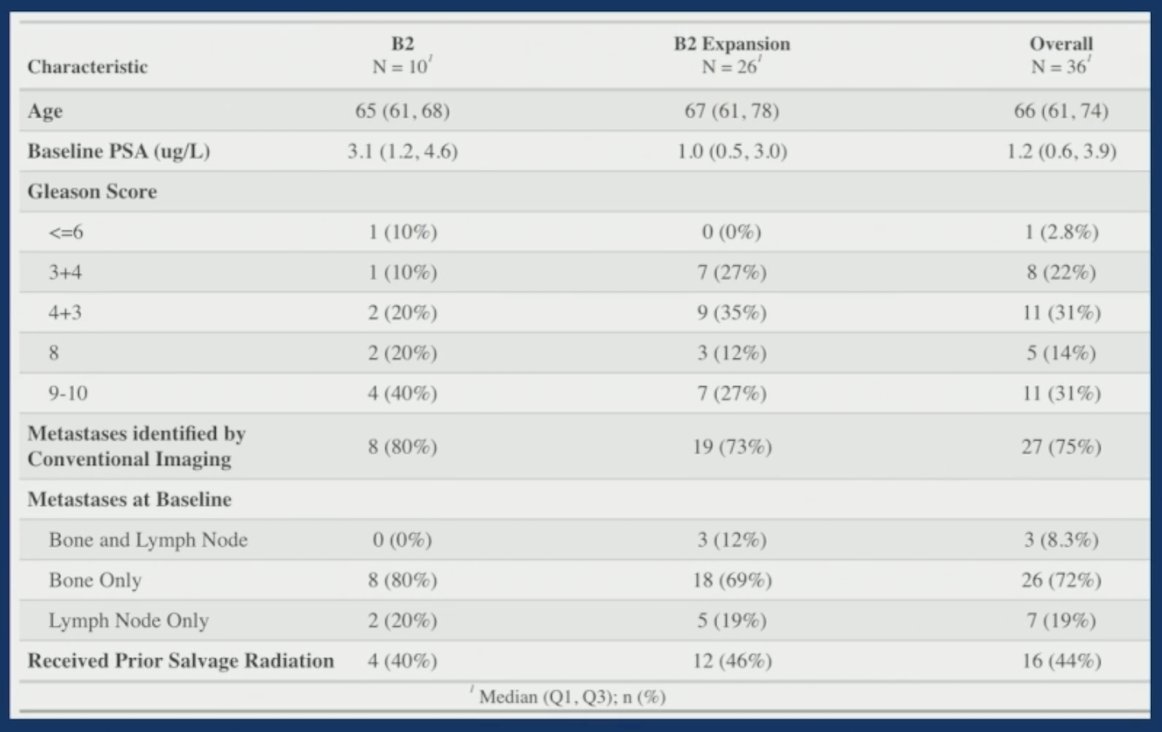
There were 36 patients treated in the combined B2 (10 patients) and B2 expansion (26 patients) cohorts. Overall, 45% of patients had Gleason 8-10 prostate cancer at diagnosis, the median PSA was 1.2 ng/mL, 75% had metastasis on conventional imaging, with 31/36 having metastasis on PSMA PET and 5/36 on fluciclovine. Most patients (72%) had bone only metastases, and 75% had a single metastasis irradiated:
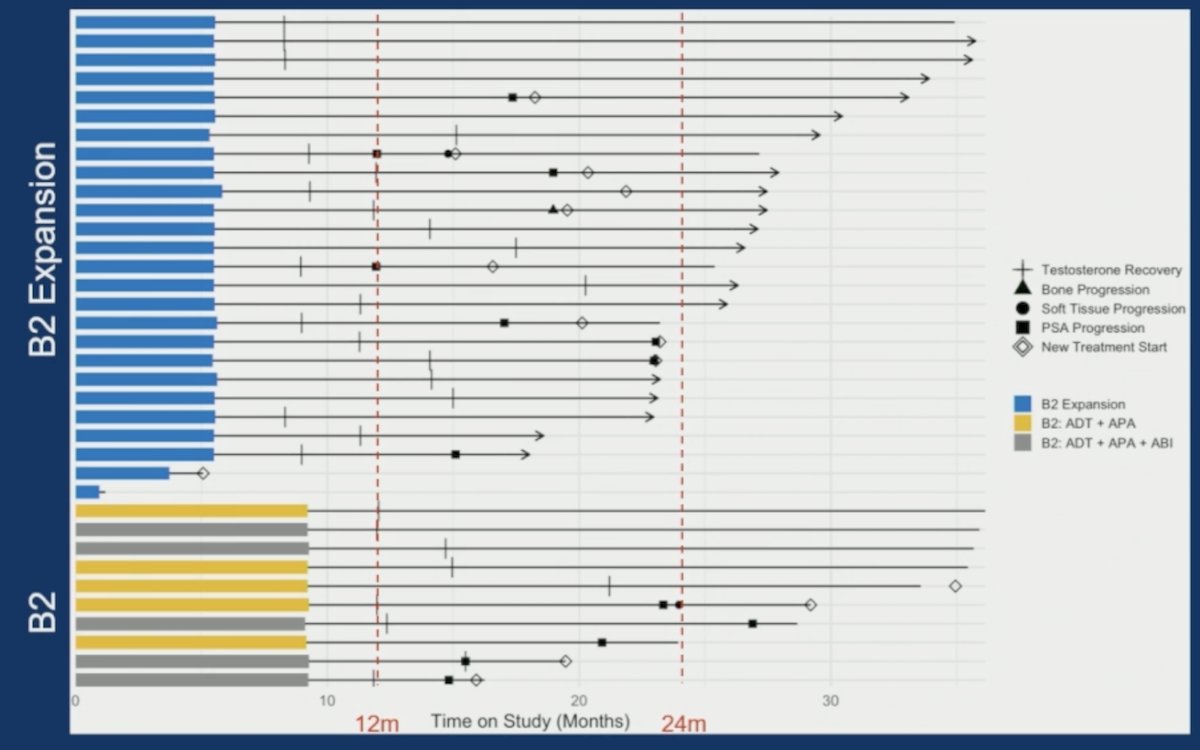
The median follow-up was 35 months for cohort B2 and 19 months for the B2 expansion. The primary endpoint of undetectable PSA with a recovered testosterone (> 150 ng/mL) was met in 11/26 (42%) of the B2 expansion patients and 5/10 (50%) of the combined B2 cohort:

This met the pre-defined statistical criteria for a positive study with > 4 patients in B2 expansion. The 24 month PSA progression free survival and 24 months radiographic progression free survival rates by cohort are as follows:

There were 16/36 patients with recovered testosterone with no progression event on study. The median time to testosterone recovery was 3 months in the B2 cohort and 5.5 months in the B2 expansion cohort:
Limitations of this trial include: (i) this was a pilot study with limited enrollment, (ii) single-arm nature of the B2 expansion limits comparison with other proposed oligometastatic castration sensitive prostate cancer regimens, and (iii) follow-up remains limited.
Dr. Bent concluded his presentation discussing results of the phase II Metacure trial assessing intensified hormonal blockade with stereotactic body radiotherapy in PSMA-PET detected oligometastatic prostate cancer with the following take home points:
- Stereotactic body radiotherapy to <= 3 sites with a short course of intensified hormonal therapy leads to rapid testosterone recovery and durable disease control
- 6 months of ADT + apalutamide with stereotactic body radiotherapy body radiotherapy is promising for metachronous oligometastatic castration sensitive prostate cancer
Presented by: Eric H. Bent, MD, Memorial Sloan-Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.