(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. David Wise discussing a phase 1 study of gotistobart (BNT316/ONC-392) in combination with lutetium Lu 177 vipivotide tetraxetan in patients with metastatic castration-resistant prostate cancer (mCRPC). When used in combination with physician’s choice of care, Lu 177 showed significant progression free survival and overall survival improvements in mCRPC. Additional combinations with novel agents are being explored to extend the therapeutic benefit. Preclinical models have demonstrated that radiotherapy selectively expands and functionally activates regulatory T cells in the tumor microenvironment. Given the role of gotistobart (a unique pH-sensitive anti-CTLA-4 antibody that preserves CTLA-4 recycling and avoids lysosomal degradation) in selective depletion of regulatory T cells in the tumor microenvironment, this study will initially test the safety and toxicity of gotistobart plus Lu 177 in mCRPC.
PRESERVE-006 (NCT05682443) is an open-label, randomized, active control, multi-center, phase 1/2 study of gotistobart in combination with Lu 177 in patients with mCRPC who have progressed after androgen receptor pathway inhibition. Patients were randomized (2:1) to receive gotistobart at 3 mg/kg, every 4 weeks, 6 mg/kg every 6 weeks, or 10 mg/kg every 6 weeks for up to 13 doses + Lu 177 7.4 GBq (200 mCi) every 6 weeks for up to 6 doses, or to the control arm to receive Lu 177 7.4 GBq (200 mCi), every 6 weeks for up to 6 doses:
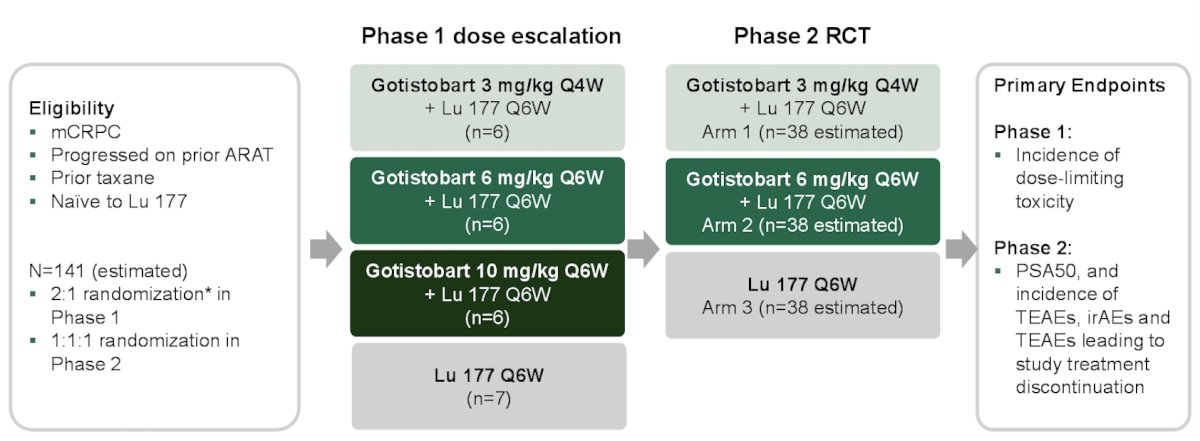
At the ASCO 2025 annual meeting, Dr. Wise and colleagues reported results from the dose escalation phase 1 that aims to assess safety and select two dose regimens for the phase 2 dose optimization study.
As of May 6, 2025, 25 patients received at least 1 drug (one patient had a baseline PSA < 1 ng/mL, which was a protocol violation, and was excluded from the safety analysis). The median age was 70.5 (range 52–86) years, and 62.5%, 25.0% and 4.2% were White, Black, and Asian, respectively:

The median follow-up was 14.7, 6.1 and 9.3 months for the 3 mg/kg every 4 weeks (n = 6), 6 mg/kg every 6 weeks (n = 5) and 10 mg/kg every 6 weeks (n = 6) combination regimens, respectively, and 10.4 months for Arm B Lu 177 (n = 7).
There were no deaths, dose-limiting toxicity, or grade 4–5 treatment-related adverse events observed at any gotistobart dose. Treatment-related adverse events related to gotistobart or Lu 177 were grade 1–2 at 3 mg/kg every 4 weeks and 6 mg/kg every 6 weeks, whereas there was one patient (16.7%) in the 3 mg/kg regimen who had grade 2 colitis leading to treatment discontinuation. At 10 mg/kg every 6 weeks, two patients (33%) had grade 3 colitis (both of whom discontinued treatment), and one patient (16.7%) had grade 3 fatigue. Infusion-related reactions (grade 1–2) were seen in 6 mg/kg (40.0%) and 10 mg/kg (66.7%) regimens:

In the efficacy-evaluable population, confirmed PSA50 (a key secondary endpoint for phase 2) was observed in 4 of 6 patients, and 3 of 6 patients in 3 and 10 mg/kg regimens, respectively, versus 2 of 6 patients in the Lu 177 control group. The following figures highlight the PSA best percent change from baseline and the PSA response over time:

Finally, the following figures demonstrate the PSA change over time and the target lesions' best percent change from baseline (RECIST 1.1):

Dr. Wise concluded his presentation discussing a phase 1 study of gotistobart (BNT316/ONC-392) in combination with lutetium Lu 177 vipivotide tetraxetan in patients with mCRPC with the following take home points:
- Overall findings support combination regimens with gotistobart doses less than 10 mg/kg
- The combination of gotistobart + Lu 177 was well tolerated and associated with durable PSA50 responses at doses of 3 mg/kg every 4 weeks, and 6 mg/kg every 6 weeks compared with Lu 177 alone, supporting these doses for the ongoing phase 2 study
- The phase 2 study is expected to complete enrollment by the end of 2025
Presented by: David R. Wise, MD, PhD, Perlmutter Cancer Center, NYU Langone Health, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Phase I Trial Combines ONC-392 with Lutetium-177 for Prostate Cancer - David Wise