(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. April Rose discussing a ctDNA–directed phase II study of carboplatin in patients with previously treated metastatic castration-resistant prostate cancer (mCRPC). PC-BETS registered patients with mCRPC for ctDNA-based genomic screening. A molecular tumor board then assigned patients to sub-studies based on prespecified biomarker criteria: biomarker positive, or by randomization if biomarker negative. IND.234G investigated carboplatin in 2 cohorts: cohort 1 included biomarker positive patients with deleterious DNA damage response (DDR) gene alterations, and cohort 2 included biomarker negative patients.
Key inclusion criteria were:
- mCRPC
- ECOG 0-1
- Evaluable disease
- Biochemical and/or radiological disease progression
- Received prior next-generation androgen receptor pathway inhibitor
- Prior chemotherapy allowed (max 1 regimen for mCRPC)
The primary endpoint was clinical benefit rate (PSA50 response, RECIST complete response/partial response, or stable disease ≥12 weeks). Secondary endpoints included time to PSA progression, and overall survival. Plasma ctDNA and matched leukocyte DNA underwent deep targeted sequencing with a prostate cancer specific panel that included ATM, BRCA1/2, and 22 other DDR genes. Patients with ctDNA <1% were not eligible unless they carried a germline DDR gene alteration. Patients received IV carboplatin (AUC5) on day 1 of 21-day cycles.
From September 2020 to February 2024, 36 patients were enrolled: 19 and 17 in cohort 1 and 2, respectively. All patients were evaluable for safety while 1 patient was not evaluable for clinical benefit rate (biochemical only disease). The median age was 69 years (range: 55-83) and 66 years (range: 54-77), 67%/82% had prior chemotherapy, 22%/6% had prior PARP inhibitor, and 6%/0% had liver metastases in cohorts 1 and 2, respectively:
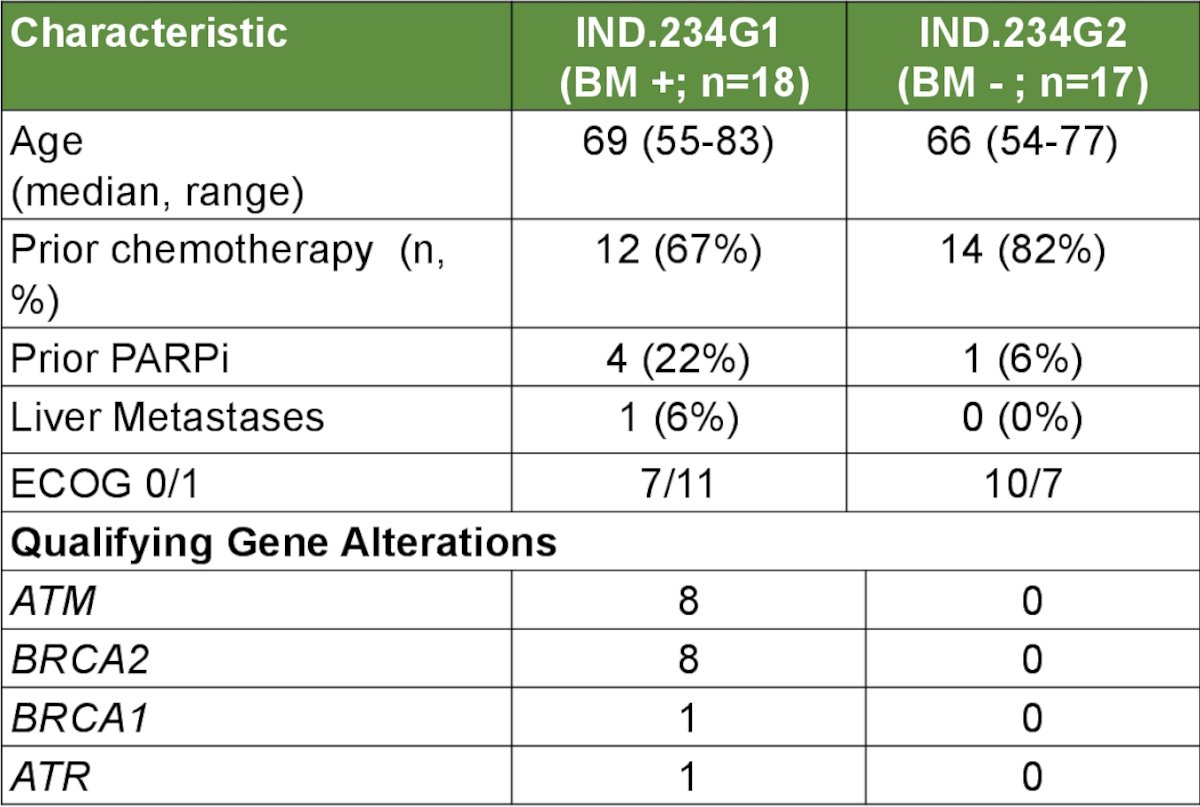
In cohort 1, qualifying gene alterations were: ATM (n = 8), BRCA2 (n = 8), BRCA1 (n = 1), and ATR (n = 1). The median number of cycles was 4 (range: 1-31). The most common adverse events were anemia (97%), thrombocytopenia (89%), lymphopenia (69%), nausea (58%), neutropenia (42%), diarrhea (22%), vomiting (22%), and constipation (33%). Grade ≥3 non-hematologic adverse events occurred in 28% of patients, and 1 patient died from an unrelated myocardial infarction. Overall, 22 patients had dose delays and 15 patients had dose reductions for hematologic adverse events. For cohort 1, clinical benefit rate was observed in 5/8 patients with BRCA2 alterations (4 patients had PSA response), 2/8 patients with ATM alterations (0 PSA responses), and 0/2 patients with ATR/BRCA1 alterations. A clinical benefit rate (with PSA response) was observed in 1 patient enrolled in cohort 2 who did not have DDR gene alterations:

The Kaplan-Meier curves for time to PSA progression and overall survival by cohort are highlighted below:

A summary of the clinical efficacy results is highlighted in the table:

Dr. Rose concluded her presentation discussing a ctDNA–directed phase II study of carboplatin in patients with previously treated mCRPC with the following take home points:
- Carboplatin was associated with meaningful clinical benefit in mCRPC patients with DDR alterations (BRCA2 or ATM mutations) detected in ctDNA, but not in patients without DDR alterations
- Carboplatin warrants further evaluation in mCRPC patients with DDR gene alterations
Presented by: April A. N. Rose, MD, PhD, FRCPC, McGill University, Montreal, Quebec, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.