(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a kidney and bladder cancers poster session. Dr. Zhu Shimiao presented PELUR, a prospective phase II trial of neoadjuvant lenvatinib plus pembrolizumab for resectable clear-cell renal cell carcinoma (ccRCC).
Lenvatinib in combination with pembrolizumab prolongs overall survival (OS) and progression-free survival (PFS) in advanced ccRCC, with significantly improved objective response rate (ORR) and survival times, compared with other agents in this setting. However, questions remain regarding the adverse event/safety profile of this combination. The efficacy and safety of neoadjuvant low-dose lenvatinib plus pembrolizumab prior to nephrectomy in ccRCC patients at high-risk of recurrence or progression has not been assessed.
This was an open label phase II clinical trial of patients with resectable, high-risk ccRCC who received neoadjuvant low-dose lenvatinib (8 mg orally once daily) plus pembrolizumab (200 mg intravenously every 3 weeks) for 3 cycles. Following surgery, patients at intermediate-high or high risk of recurrence (KEYNOTE-564 criteria1 – i.e., pT2, G4; pT3-4, pN1, and/or pM1) were recommended for pembrolizumab 200 mg every 3 weeks for up to 17 cycles.
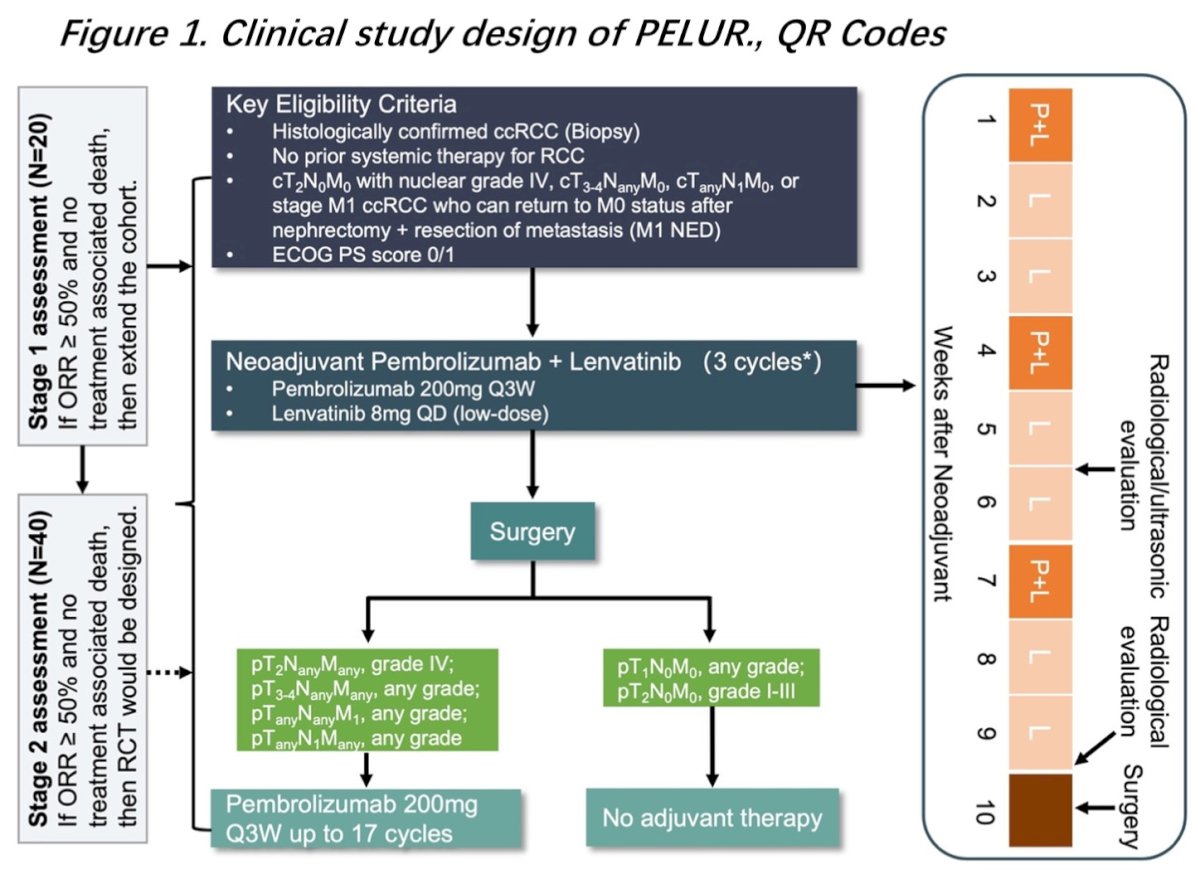
Participants were enrolled from July 2022 to December 2023. The primary endpoints were tumor response and safety. The secondary endpoints were PFS and patient-reported quality-of-life outcomes.
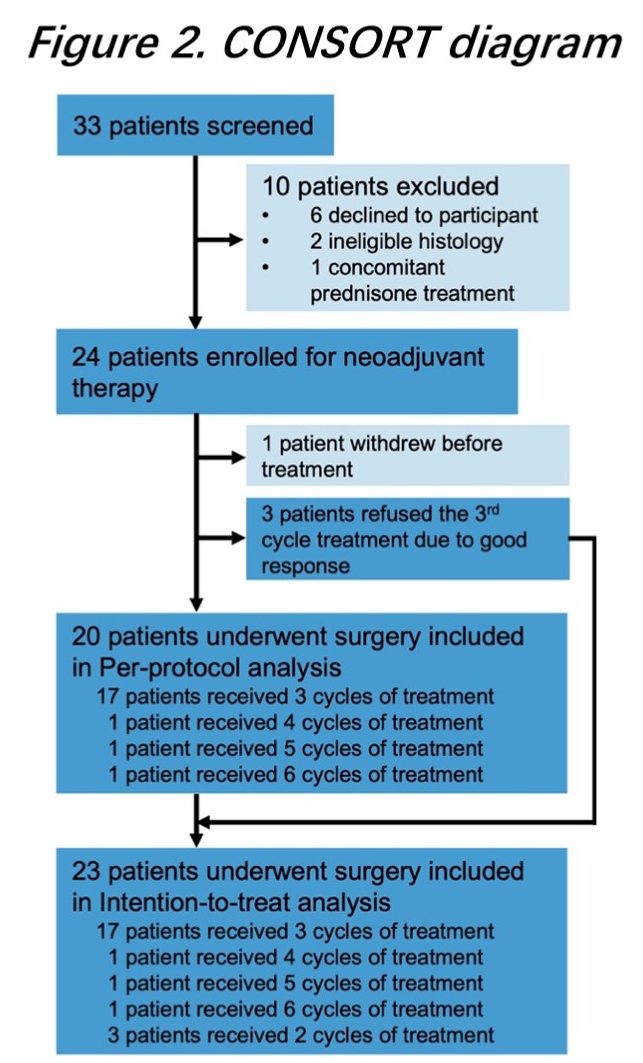
A total of 33 patients were enrolled – 23 received neoadjuvant therapy followed by radical nephrectomy and were included in the intention-to-treat (ITT) analysis.
All patients received neoadjuvant therapy at the dose pre-specified in the protocol, with no dose reductions or discontinuations required. Two patients had their surgery delayed due to reasons not related to adverse events. There was only one grade 3 adverse event (hypertension) during neoadjuvant therapy. The most common treatment-emerged adverse events of any grade during neoadjuvant treatment were:
- Hypertension
- Fatigue
- Rash
- Pruritis
During adjuvant therapy, three grade 3 adverse events were reported, including one case of rash, ALT/AST elevation, and acute kidney injury. The most common AEs of any grade during adjuvant pembrolizumab were rash, fatigue and pruritus (n=6, 26.1%).
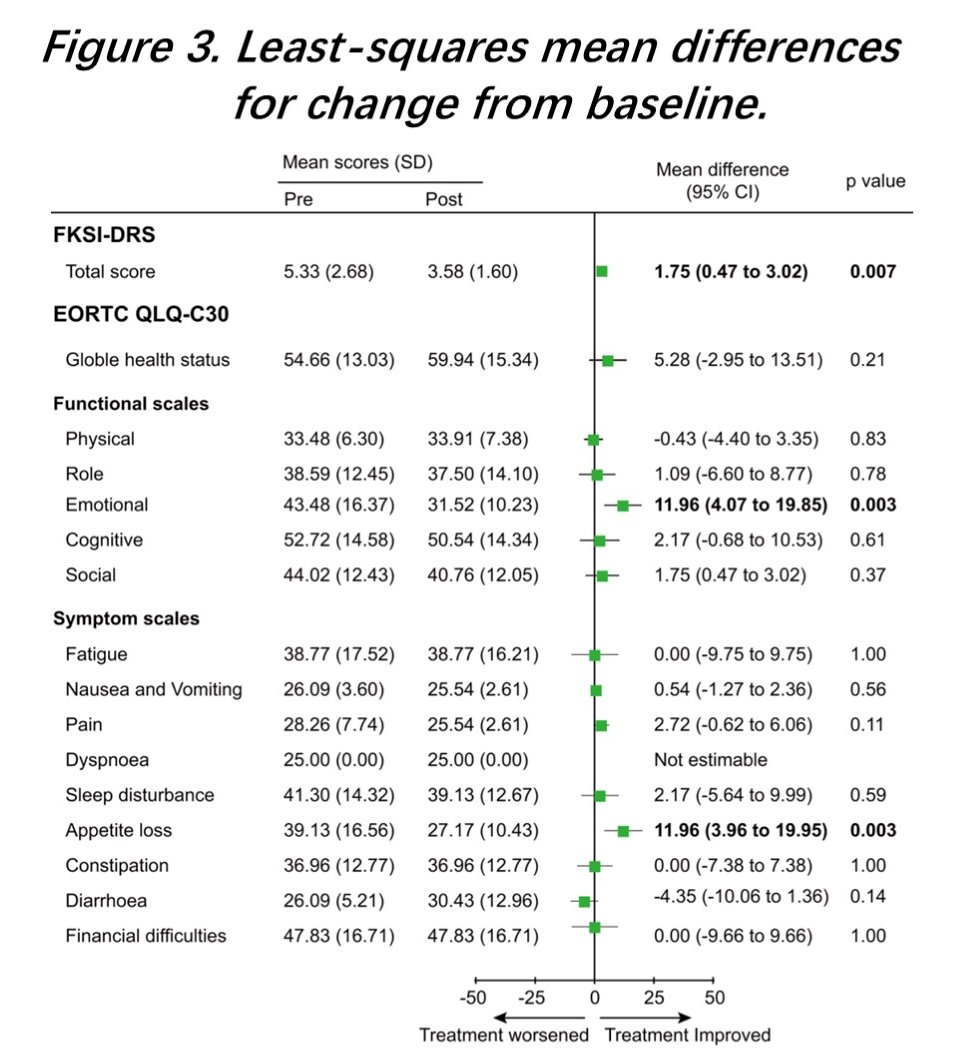
On the EORTC Cancer Quality of Life Questionnaire (EORTC QLQ-C30) questionnaires, there was evidence of significant improvements in all emotion functional domains and appetite. The total score of the Functional Assessment of Cancer Therapy Kidney Symptom Index Disease-Related Symptoms (FKSI-DRS) was also significantly improved.
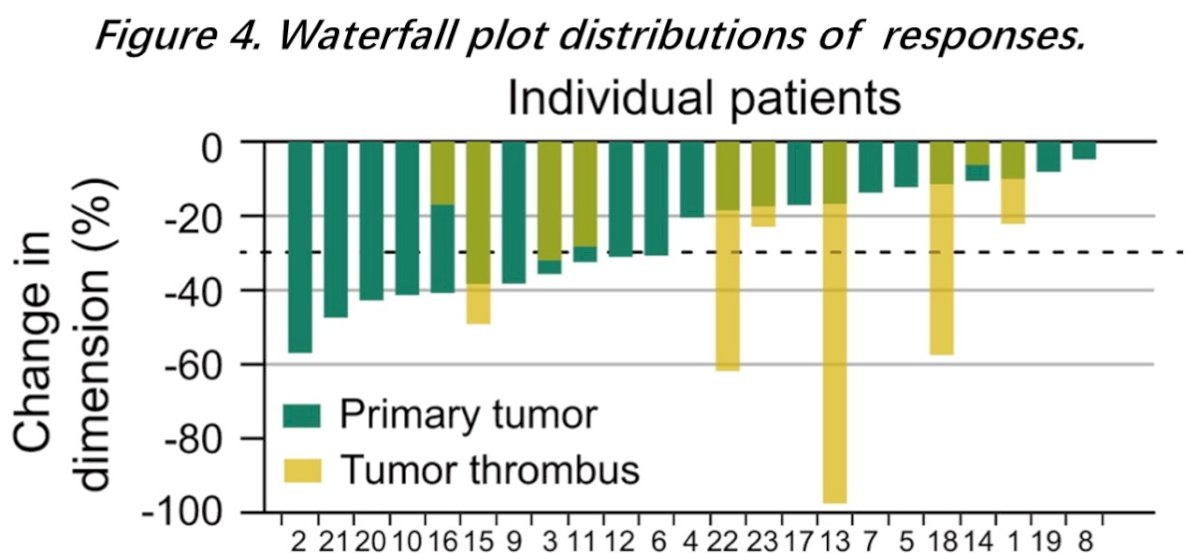
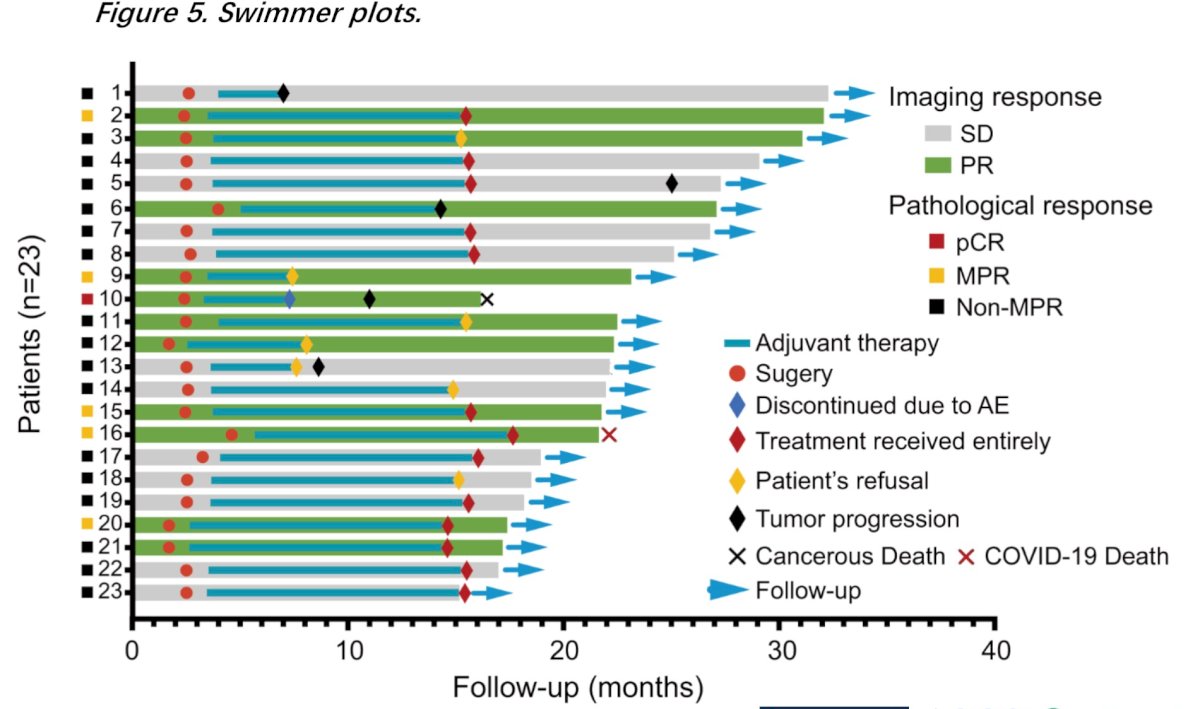
Tumor and thrombus regression occurred in all patients following neoadjuvant therapy, with 11/23 (48%) of patients experiencing a partial response.
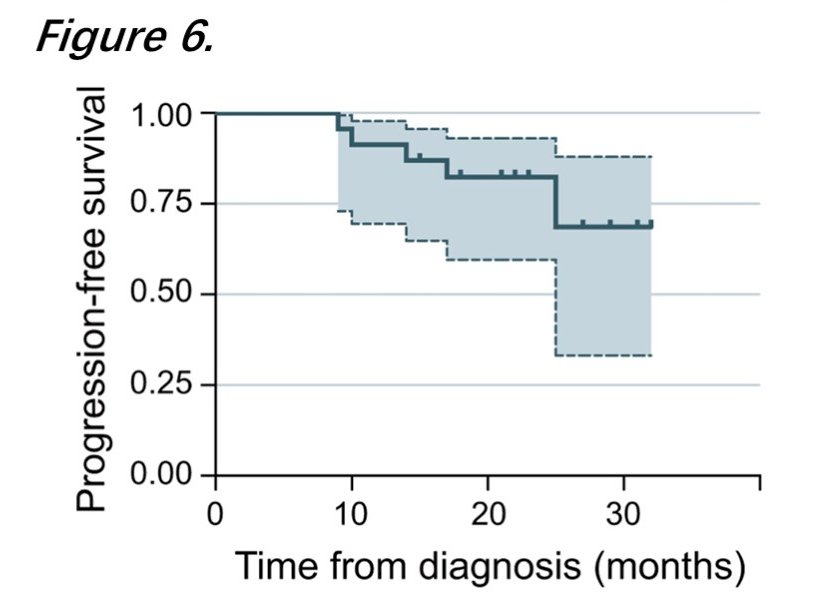
At a median follow-up of 22 months (IQR: 15–35 months), five patients experienced disease progression and two died (ccRCC-related: 1; COVID-related: 1).
Dr. Shimiao concluded that this data preliminarily demonstrated the safety and efficacy of neoadjuvant low-dose lenvatinib plus pembrolizumab followed by a radical nephrectomy in ccRCC patients at high-risk of recurrence or progression.
Presented by: Zhu Shimiao, MD, PhD, Tianjin Institute of Urology, the Second Hospital of Tianjin Medical University, Tianjin, China
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References: