(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a kidney and bladder cancers oral abstract session. Dr. Samer Srour presented updated results of the phase I TRAVERSE study of ALLO-316 in advanced clear cell renal cell carcinoma (ccRCC).
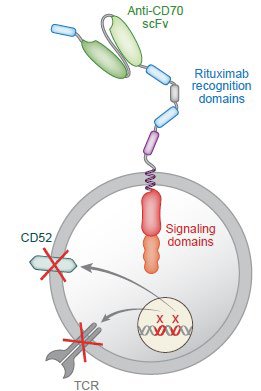
CAR T therapy has revolutionized the treatment of hematologic malignancies, but progress in solid tumors has been slow.1 ALLO-316 is an off-the-shelf, HLA-unmatched allogeneic CD70 CAR T product designed to target both CD70+ tumors and alloreactive host T cells. Phase Ia data from the TRAVERSE study of ALLO-316 in patients with ccRCC showed manageable safety with promising antitumor activity.2 The results from 20 heavily pre-treated, refractory patients in the phase Ib part of the study, treated with standard lymphodepletion and 80M CD70 CAR T cells were reported by Dr. Srour in this presentation.
The study design of the TRAVERSE phase 1b portion (NCT04696731) is summarized below. This trial included patients meeting the following eligibility criteria:
- Adult patients with advanced or metastatic clear cell RCC
- Disease progression after PD-1 axis and VEGF targeted therapies
- CD70 positive by immunohistochemistry on archival or fresh tumor tissue
- Excellent performance status with adequate end-organ function
In the phase 1b portion, patients underwent standard lymphodepletion from Days -5 to -3, followed by ALLO-316 80x106 CAR+ cells on Day 0. Patients were monitored until 60 months for response and safety assessments. The phase 1b endpoints are as follows:
- Primary: Treatment-emergent adverse events (TEAEs)
- Secondary:
- Objective response rate (ORR)
- Complete response rate (CRR)
- Duration of response (DoR)
- Time to response (TTR)
- Progression-free survival (PFS)
- Overall survival (OS)
- CAR T expansion kinetics

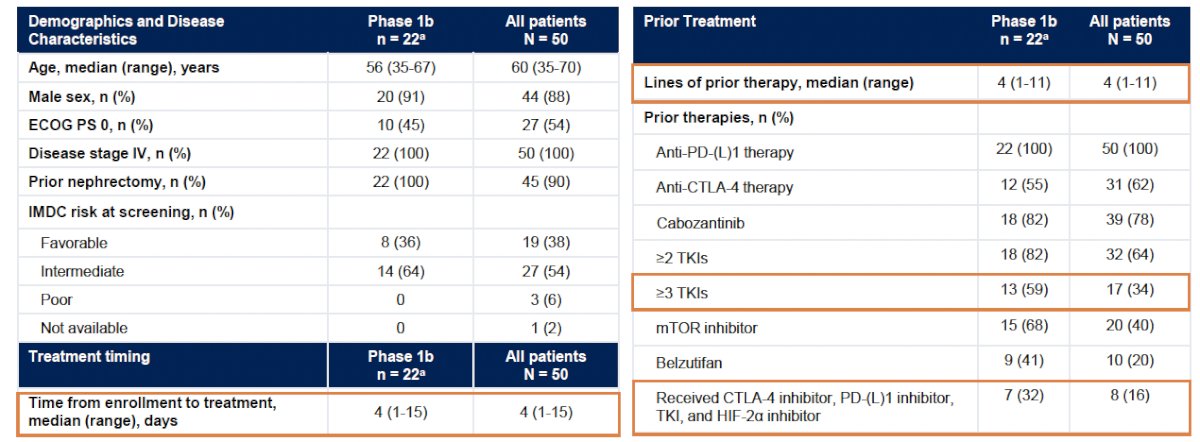
Phase 1b patients (n=22) received a median of 4 prior lines of therapy: 59% had received 3+ prior TKIs, 41% had received belzutifan, and 32% were quadruple class refractory to inhibition of the CTLA-4, PD-(L)1, TKI, and HIF-2α pathways:
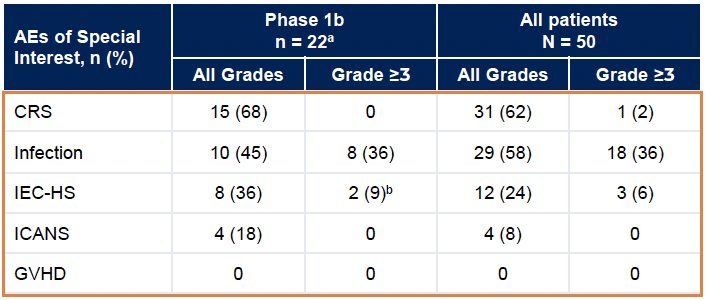
The adverse event profile was consistent with that of lymphodepletion and active CAR T therapy. Any-grade TEAEs occurred in 100% of phase 1b patients, including:
- The majority of Grade ≥3 TEAEs were hematologic in nature
- No treatment-related Grade 5 AEs were observed

In the 20 patients from the phase 1b portion with evaluable efficacy data, an ORR was observed in 25% (5/20). All ORRs were observed in patients with a CD70+ tumor proportion score (TPS) ≥50%.
Tumor responses occurred early and were sustained following a single infusion of ALLO-316. Among CD70+ TPS ≥50% patients, 44% (7/16) had >30% reduction in the diameters of baseline target lesions.
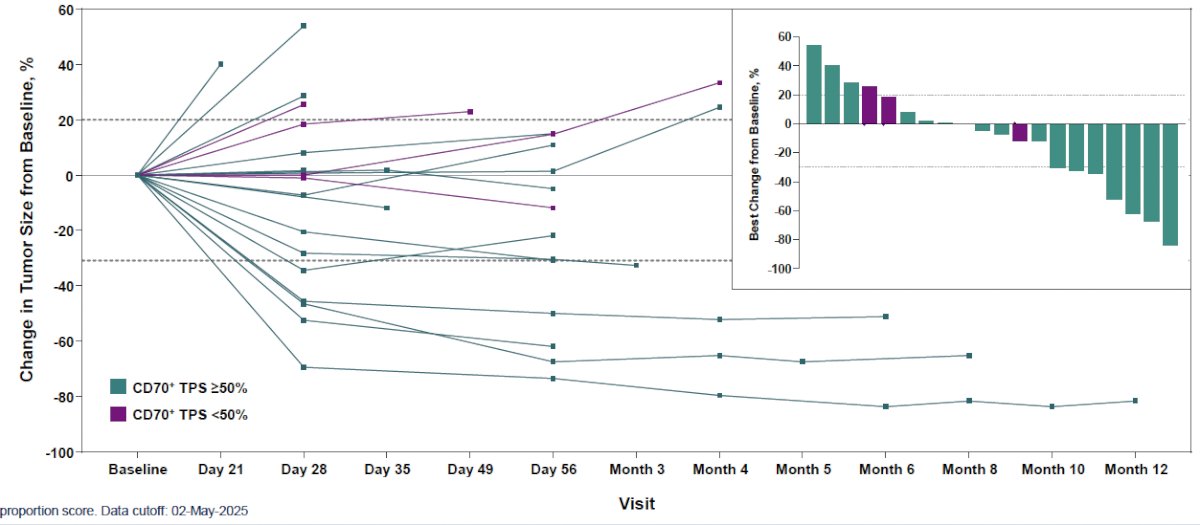
Out of the 5 confirmed responders, 4 have an ongoing response; 1 has reached the 1-year mark post–ALLO-316.

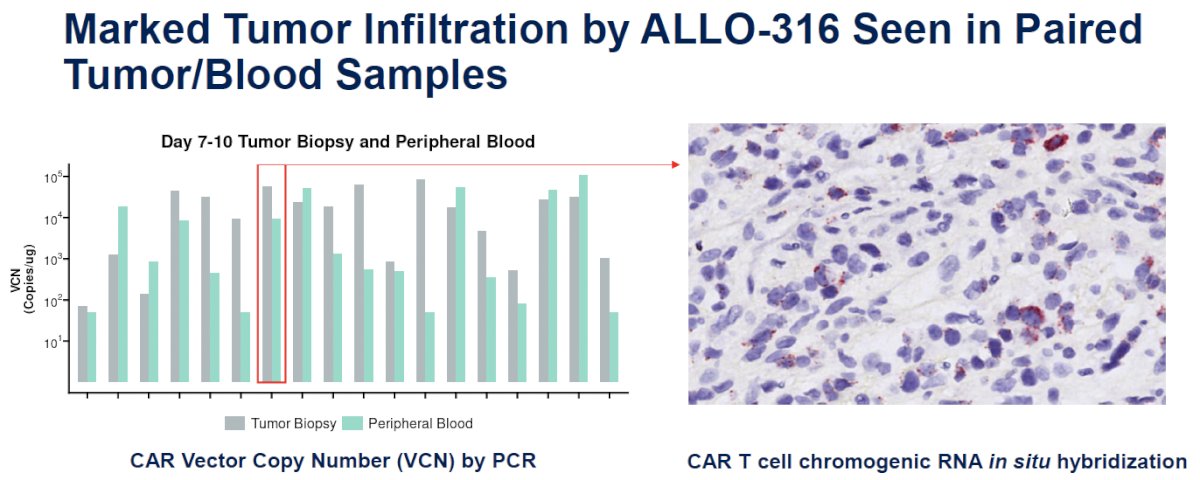
Homing and infiltration of ALLO-316 CAR T cells into the tumor was demonstrated by two independent methods: VCN (PCR) and chromogenic RNA in situ hybridization assay using a probe against CAR transcripts. The high VCN levels observed in the tumor samples demonstrated the extensive infiltration of ALLO-316.
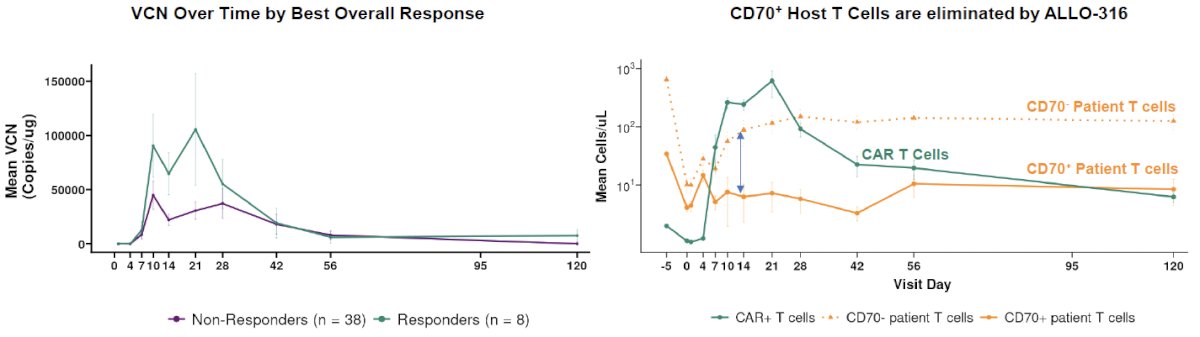
The responders had robust expansion and persistence of CAR T cells. CD70- patient T cells quickly rebounded while CD70+ patient T cells remained low until ALLO-316 CAR T contraction (Dagger® Effect).
Dr. Srour concluded as follows:
- Patients with advanced or metastatic clear cell RCC have limited options following development of disease resistant to checkpoint blockers, TKIs and HIF-2α inhibitors
- A single dose of ALLO-316 demonstrated a 31% confirmed ORR in patients with heavily-pretreated advanced or metastatic ccRCC. 4 of 5 responses are ongoing, including one extending beyond a year after treatment, representing a potential breakthrough for CAR T therapy in solid tumors
- Safety profile was manageable and consistent with standard Flu/Cy lymphodepletion and an active CAR T therapy. Improvements in the diagnosis of IEC-HS enabled early intervention and effective management
- ALLO-316 delays allorejection by depleting patient CD70+ cells, driving robust and sustained CAR T-cell expansion. This Dagger® effect may be incorporated into other allogeneic CAR T products to enable CAR T expansion and improve responses with reduced intensity of lymphodepletion.
- These results underscore the transformative potential of allogeneic CAR T in solid tumors and validate further development of ALLO-316 in RCC and other CD70+ malignancies
Presented by: Samer Ali Srour, MBChB, MS, Assistant Professor, Transplant Physician, Department of Stem Cell Transplantation and Cellular Therapy, The University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Albelda SM, June CH, Wherry EJ, et al. Immune resistance in cancer: strategies for clinical translation. Nat Rev Clin Oncol. 2024; 21:47–66.
- Srour SA, Smith L, Johnson K, et al. Emerging immunotherapy combinations in solid tumors: insights from preclinical models. J Immunother Cancer. 2024; 12(Suppl 2):A1–A1683.