(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a kidney and bladder cancers oral abstract session. Dr. Toni Choueiri presented results from the expansion cohort of the phase I ARC-20 study of combination casdatifan plus cabozantinib in patients with previously treated clear cell renal cell carcinoma (RCC).
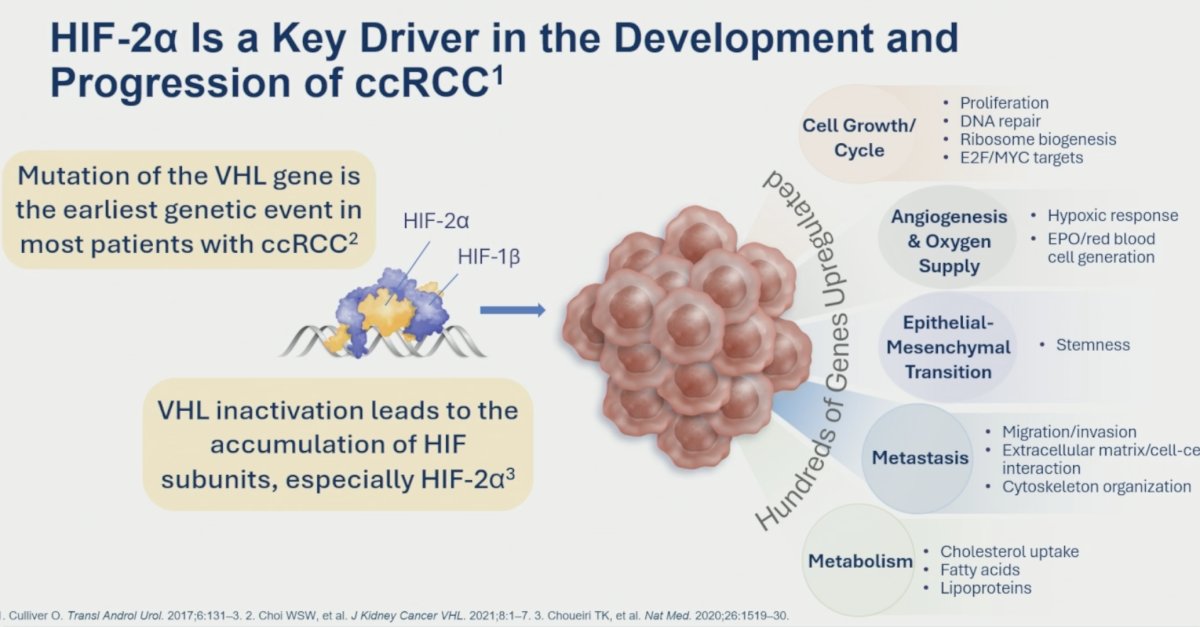
The HIF-VHL pathway is critical to RCC pathogenesis. Under normal oxygen conditions, VHL causes ubiquitination of HIF and targets it for proteosomal degradation. However, when VHL is lost, HIF accumulates in the cell – the alpha and beta units dimerize, translocate into the nucleus, and bind to the hypoxia response elements causing activation of downstream target genes. This leads to increased angiogenesis, cell survival, tumor growth, and all other hallmarks of RCC development.
Casdatifan is a novel HIF-2α inhibitor with unique pharmacodynamic/pharmacokinetic properties:1-4
- Pharmacokinetics:
- Dose-proportional exposure over a tested range (3–150 mg)
- Mean half-life of ~14 hours
- Pharmacodynamics:
- Dose- and concentration-dependent reductions in erythropoietin (EPO) after single and multiple doses, consistent with HIF-2α inhibition
- Similar levels of EPO suppression with casdatifan 20 mg once daily in patients with clear cell RCC as belzutifan 120 mg once daily
Casdatifan 100 mg once daily has been identified as the optimal dose, including in combination with cabozantinib. At this dose, casdatifan has shown a rapid response with meaningful clinical activity and disease control and is well-tolerated with no dose-limiting toxicities.
ARC-20 is a phase I dose-escalation and dose-expansion study of casdatifan. In the dose-escalation portion, Casdatifan monotherapy doses from 20 mg once daily to 200 mg once daily are being evaluated. There are 8 dose expansion cohorts, each with 25–30 patients. In today’s presentation, Dr. Choueiri reported the initial safety and preliminary efficacy data from the casdatifan 100 mg once daily + cabozantinib 60 mg once daily combination cohort of patients who have previously been treated with an anti-PD-1/L-1 agent.

The baseline patient characteristics are summarized below (n=42). The median patient age was 63 years. 79% of patients had IMDC intermediate- or poor-risk disease. The majority (83%) had received one prior line of therapy. 40% had previously received IO + TKI therapy, whereas 60% had received prior IO therapy (either IO-IO or adjuvant pembrolizumab).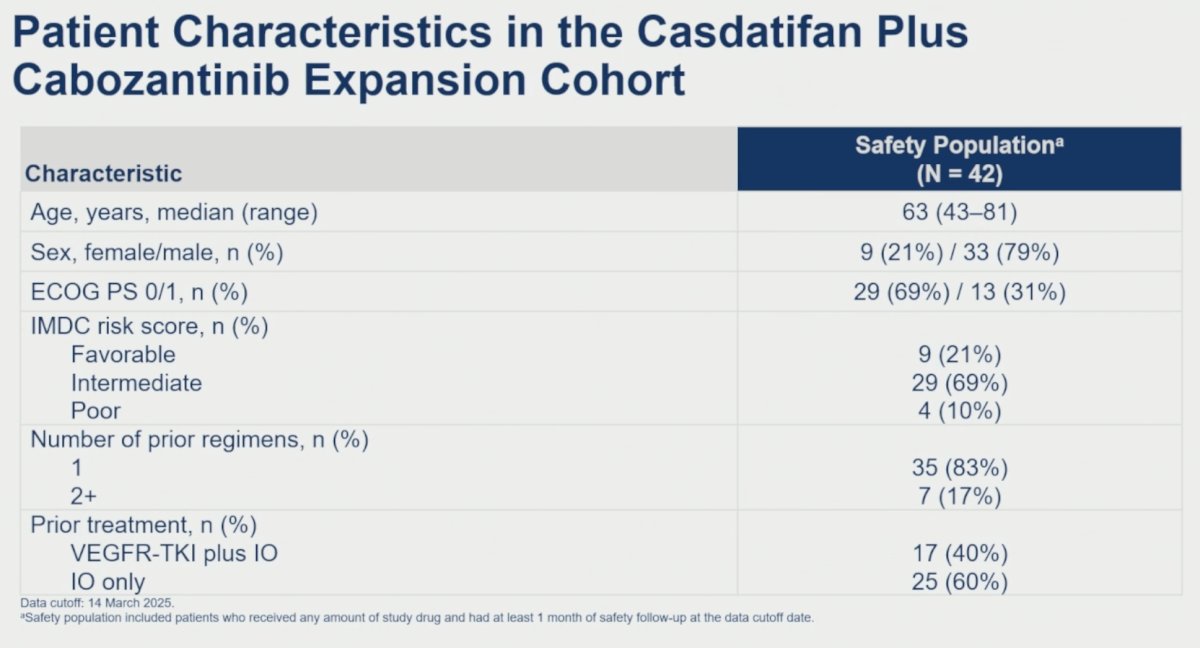
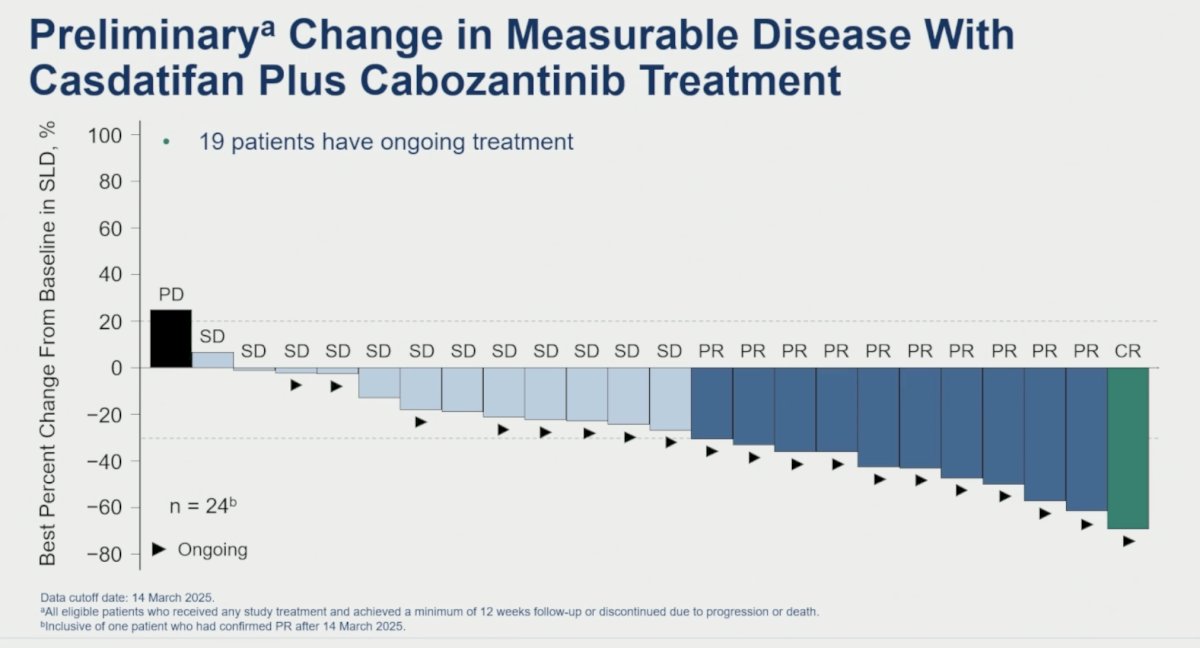
The preliminary efficacy data for the 24 evaluable patients (2 scans required) are summarized below. At a median follow-up of 5.3 months, the confirmed objective response rate (ORR) was 46% (complete: 4%; partial: 42%). Additionally, 50% of patients had stable disease.
As seen below, only one patient had evidence of progressive disease and another patient had an ~5% increase in lesion diameter, with all other 22 evaluable patients experiencing a decrease in the lesion diameter.
The Swimmer’s plot below highlights the time on treatment and timing/duration of responses:
Almost all patients (98%) experienced treatment-related adverse events (TRAEs). The most common TRAEs with casdatifan were anemia (69%) and fatigue (48%). Most cases of anemia and fatigue did not require a dose change and resolved.

Grade ≥3 TRAEs were observed in 48% of patients (31% likely due to casdatifan). Grade ≥3 anemia was observed in 24% of patients. No casdatifan-related grade 4 or 5 AEs were observed.
Only two patients discontinued treatment due to a treatment-emergent AE (TEAE; hypoxia and drug hypersensitivity), and no patients discontinued both treatments due to a TEAE).
Dr. Choueiri concluded his presentation of the ARC-20 dose expansion cohort of casdatifan + cabozantinib in PD-1/L-1-pre-treated metastatic clear cell RCC patients as follows:
- Casdatifan 100 mg once daily plus cabozantinib 60 mg once daily shows promising clinical activity in patients with clear cell RCC previously treated with anti-PD-1/PD-L1 therapy
- Casdatifan plus cabozantinib has a manageable toxicity profile in previously treated patients with clear cell RCC
- Most cases of anemia did not require a dose change and were resolved
- The ARC-20 findings support the evaluation of casdatifan for the management of clear cell RCC across different settings
Presented by: Toni K. Choueiri, MD, Jerome and Nancy Kohlberg Professor of Medicine, Dana-Farber Cancer Institute and Harvard Medical School, Boston, MA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Ghasemi M, Walker J, Miller E, et al. First clinical data from ARC-20: a Phase 1 study of casdatifan, a HIF-2α inhibitor, in patients with advanced clear cell renal cell carcinoma. Presented at: 36th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics; 2024 Oct 23–25; Barcelona, Spain.
- Choueiri TK, Ghasemi M, Walker J, et al. First clinical data from ARC-20: a Phase 1 study of casdatifan, a HIF-2α inhibitor, in patients with advanced clear cell renal cell carcinoma. Presented at: 36th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics; 2024 Oct 23–25; Barcelona, Spain.
- Choueiri TK, Ghasemi M, Walker J, et al. Casdatifan monotherapy in patients with previously treated clear cell renal cell carcinoma (ccRCC): safety, efficacy, and subgroup analysis across multiple doses from ARC-20, a Phase 1 open-label study. Presented at: ASCO Genitourinary Cancers Symposium; 2025 Feb 13–15; San Francisco, CA.
- U.S. Food and Drug Administration. Belzutifan NDA review document. (Accessed 2025A).