(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a kidney and bladder cancers oral abstract session. Dr. Vivek Narayan presented the 5-year follow-up analyses from the phase III LITESPARK-004 trial of belzutifan, a Hypoxia-Inducible Factor-2α (HIF-2α) inhibitor, in von Hippel-Lindau (VHL) disease–associated neoplasms.
The HIF-2α inhibitor belzutifan is approved for the treatment of VHL disease–associated renal cell carcinoma (RCC), central nervous system (CNS) hemangioblastoma, and pancreatic neuroendocrine tumors (pNETs) that do not require immediate surgery.1

At the last analysis of the LITESPARK-004 study (minimum study follow-up of 4 years) of belzutifan for VHL disease–associated neoplasms, the following results were observed:
- Objective response rate (ORR):
- RCC: 67%
- CNS hemangioblastoma: 48%
- pNETs: 91%
- The median duration of response (DoR) was not reached for all 3 tumor types
Herein, Dr. Narayan presented updated results from the 5-year follow-up of LITESPARK-004. The study design of this phase II trial is summarized below. Eligible patients were those with a VHL diagnosis based on a germline alteration, ≥1 measurable renal cell carcinoma (RCC) tumor, no prior systemic anticancer therapy, no metastatic disease, and an Eastern Cooperative Oncology Group performance status (ECOG PS) score of 0 or 1. Sixty-one participants were enrolled, and they received oral belzutifan 120 mg once daily. Tumor assessments were performed at screening, every 12 weeks for ≥3 years, and then every 24 weeks thereafter. The primary study endpoint was ORR in VHL disease-associated RCC per RECIST v1.1 by an independent review committee (IRC).

Efficacy and safety were analyzed in all participants who received ≥1 dose of study treatment.
Adverse events were monitored throughout the study and were graded by NCI CTCAE, version 4.03. The median time from first dose to data cutoff was 61.8 months.
As of the data cutoff date, 61 participants were treated and 35 were continuing treatment. The median study follow-up was 61.8 months. The primary reason for treatment discontinuation was participant decision.
At baseline, all participants had RCC; 50 (82%) had at ≥1 evaluable CNS hemangioblastoma tumor and 20 (33%) had ≥1 pNET. 59 (97%) participants underwent ≥1 VHL disease–related surgical procedure before starting belzutifan.

The ORR was 70.5%. A complete response (CR) was observed in 7 (11%) patients and a partial response (PR) in 36 (59%). From the previous data cutoff date of April 3, 2023, to the current data cutoff date of April 1, 2024, the ORR increased from 67% to 70.5% (2 additional partial responses). 93% of participants experienced any reduction from baseline in the total sum of RCC target lesion diameter.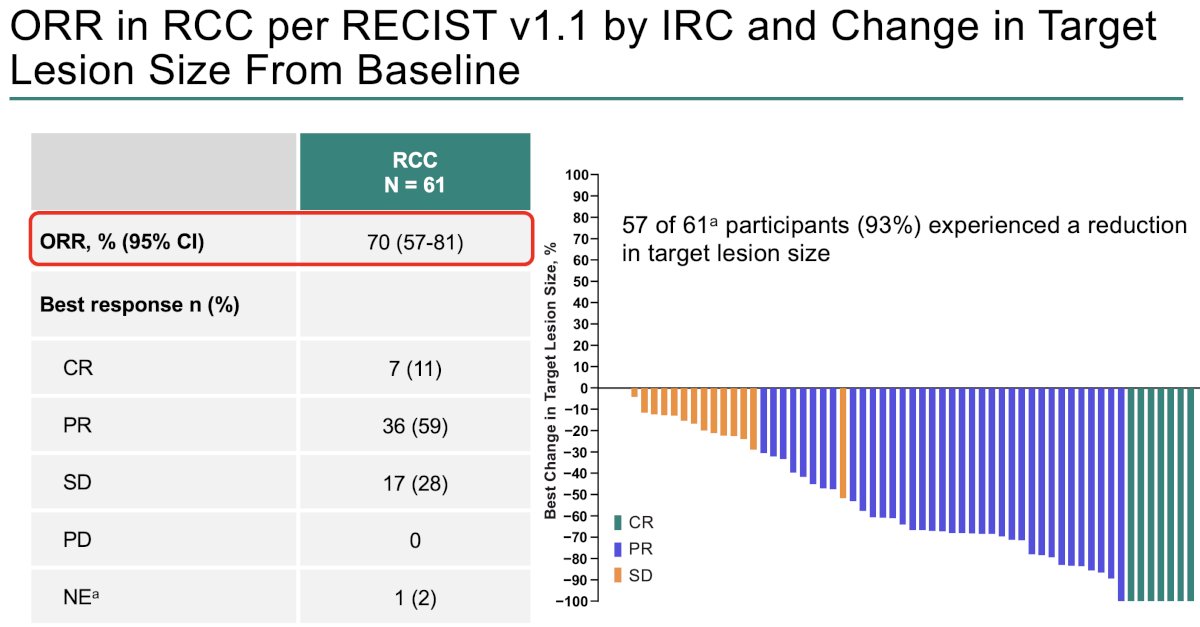
ORRs were observed across number/size of RCC lesions. The highest CRs were observed in patients with solitary tumors <2 cm in size (5 complete; 32%).
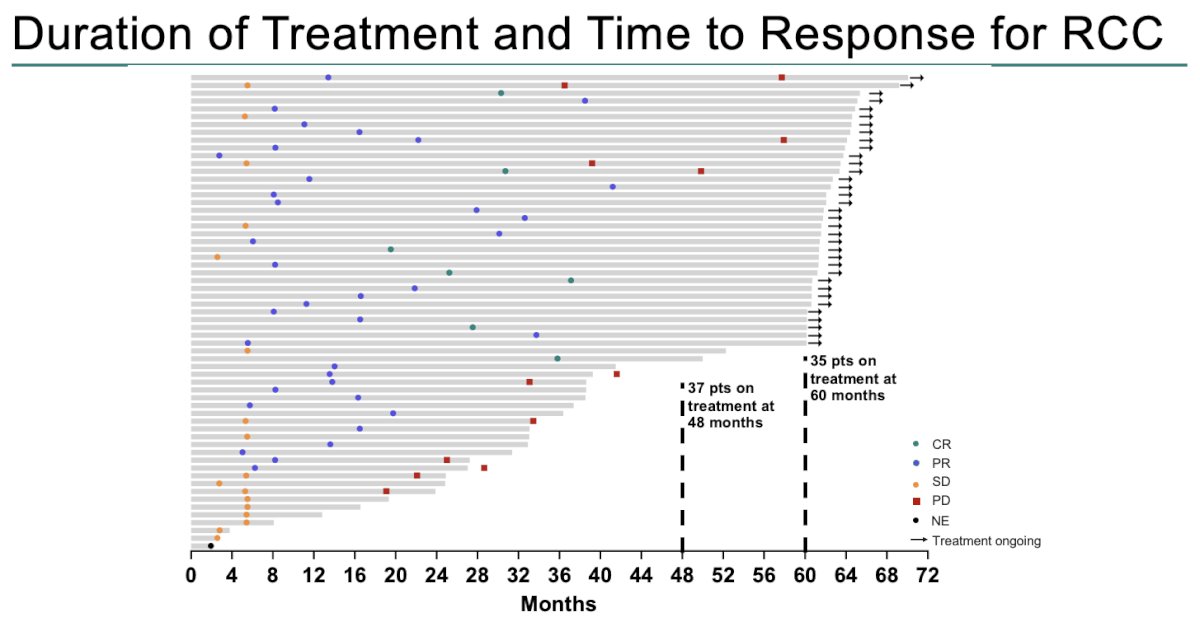
The median duration of therapy was 60.2 months. Thirty-five participants remained on treatment at 60 months. Five patients with progressive disease remained on treatment, as of the data cut-off date. The median time to response was 8.5 months (range: 2.7–41.2).
76.2% of participants with RCC remained in response at the 4-year landmark.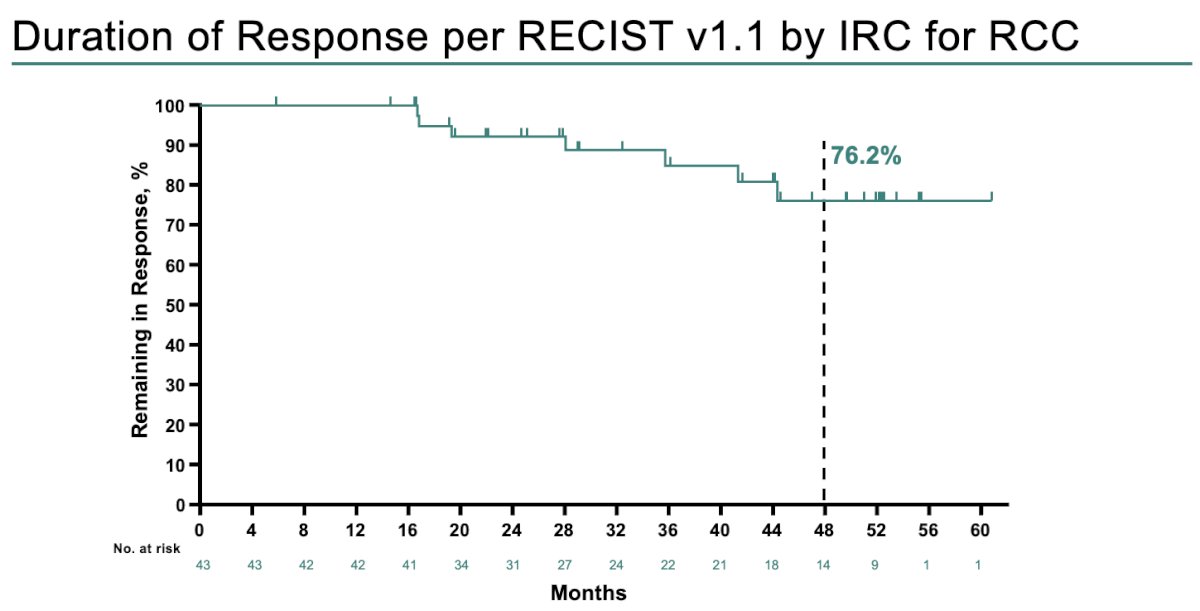
The ORR in CNS hemangioblastomas increased from 48% to 50%, with four participants experiencing a CR and 18 experiencing PRs. 96.7% of participants with measurable CNS hemangioblastoma tumor size experienced any reduction from baseline in the total sum of target lesion diameter. Of 30 participants with RCC and measurable CNS hemangioblastoma tumor size, 27 (90%) had shrinkage in both tumor types, 2 (6.7%) had only CNS tumor shrinkage, and 1 (3.3%) had only RCC tumor shrinkage.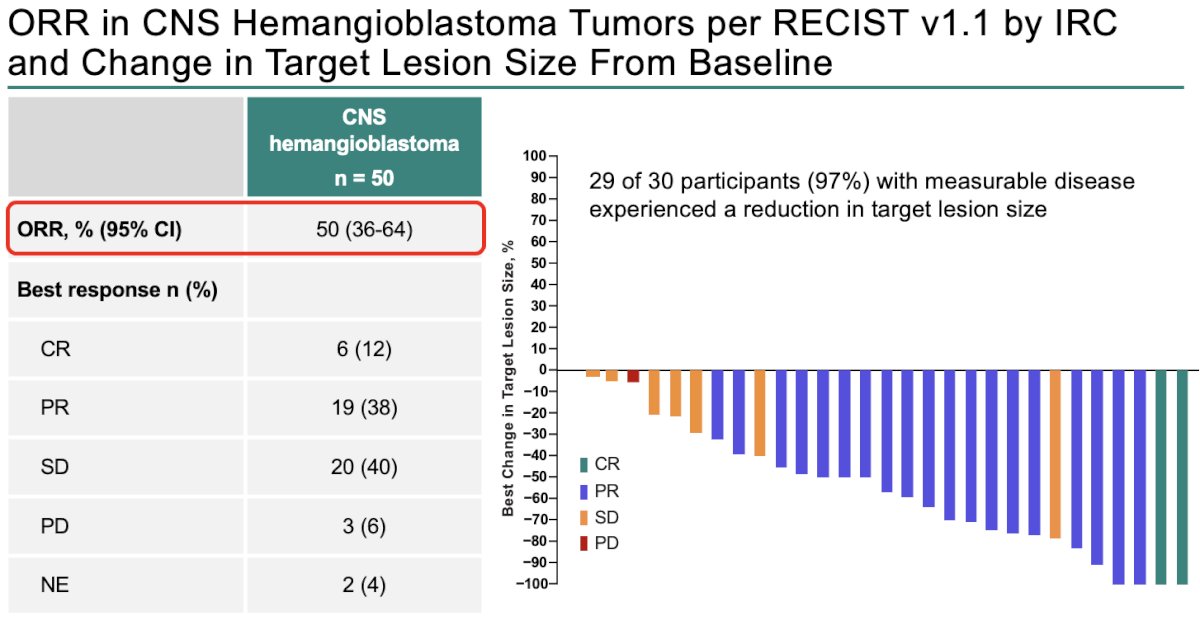
At 48 months follow-up, 81.5% of patients had maintained their response for CNS hemangioblastomas.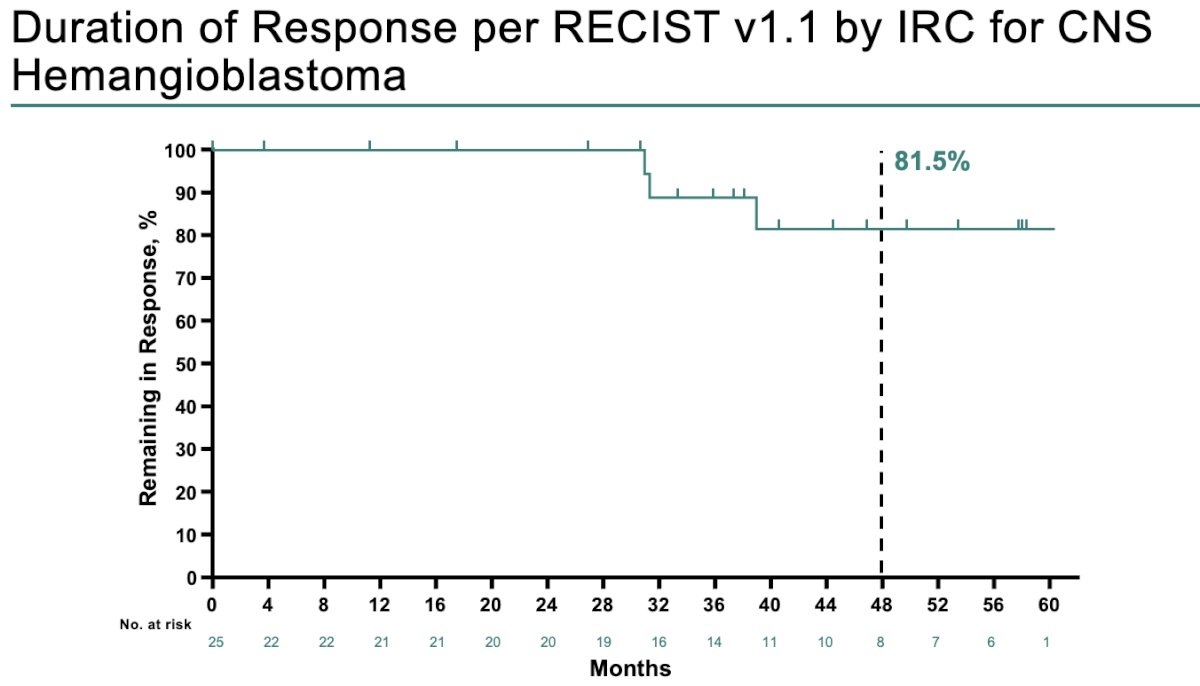
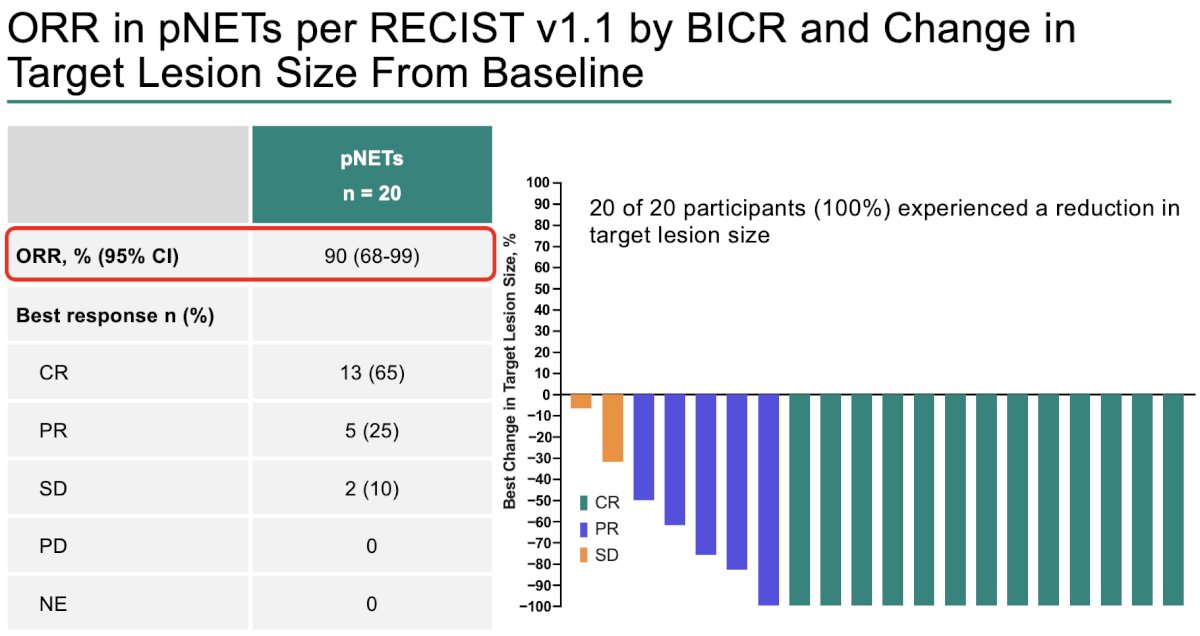
The ORR in pNETs was 90%. 100% of participants with pNETs experienced any reduction from baseline in the total sum of target lesion diameter.
At 48 months follow-up, 94.1% of patients had maintained their response for pNETs.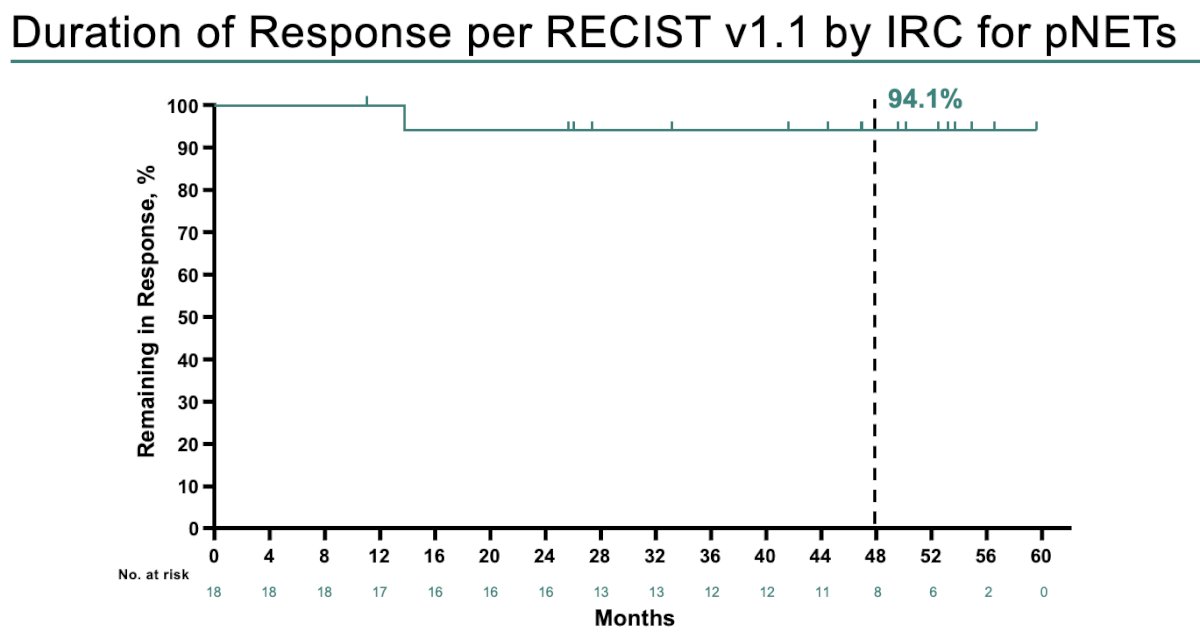
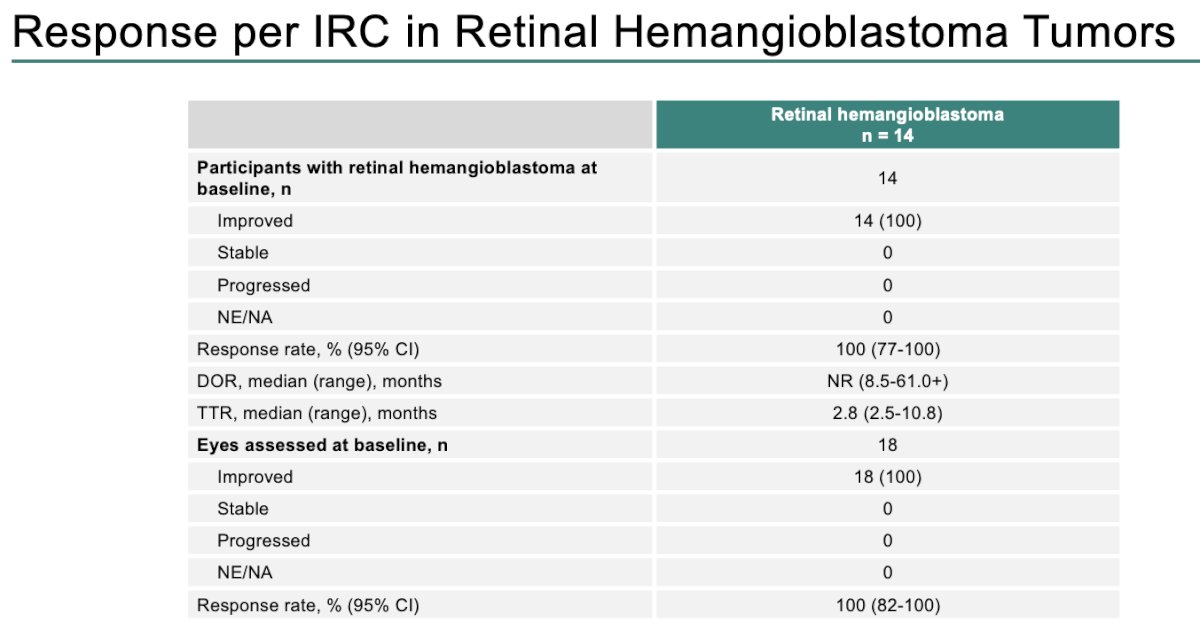
There were 14 participants with retinal hemangioblastoma tumors. All 18 lesions in the 14 participants demonstrated improvement during follow-up (response rate: 100%).
Within 5 years before starting belzutifan, 46 participants (75%) underwent 97 VHL-related procedures. After starting belzutifan:
- 19 participants (31%) underwent 24 surgical procedures
- 17 RCC
- 3 CNS hemangioblastoma
- 1 pancreatic lesion
- 3 retinal hemangioblastoma
- 1 participant received radiation therapy for CNS hemangioblastoma

All participants experienced ≥1 treatment-related adverse event (TRAE). There was no grade 4–5 TRAEs observed. No additional participants have discontinued treatment or died since the latest data cutoff date of April 1, 2024.
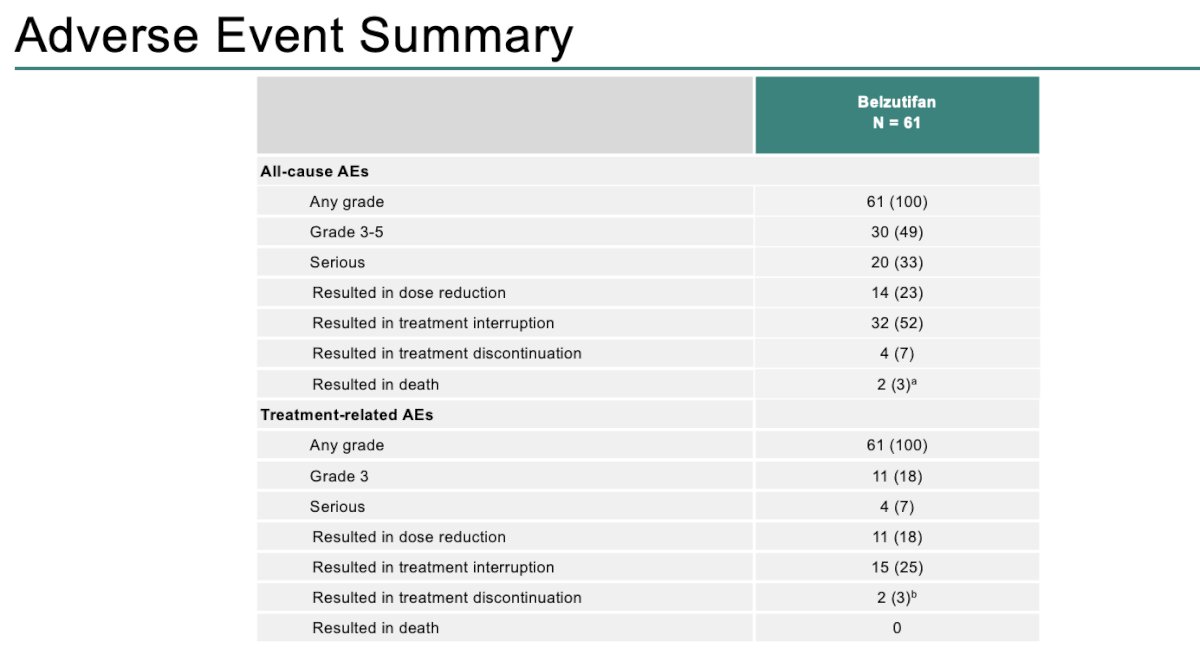
Grade 3 adverse events occurred in 41% of participants, and grade 4 or 5 events occurred in 8% of participants. Adverse events with an incidence ≥20% are summarized in the graph below:
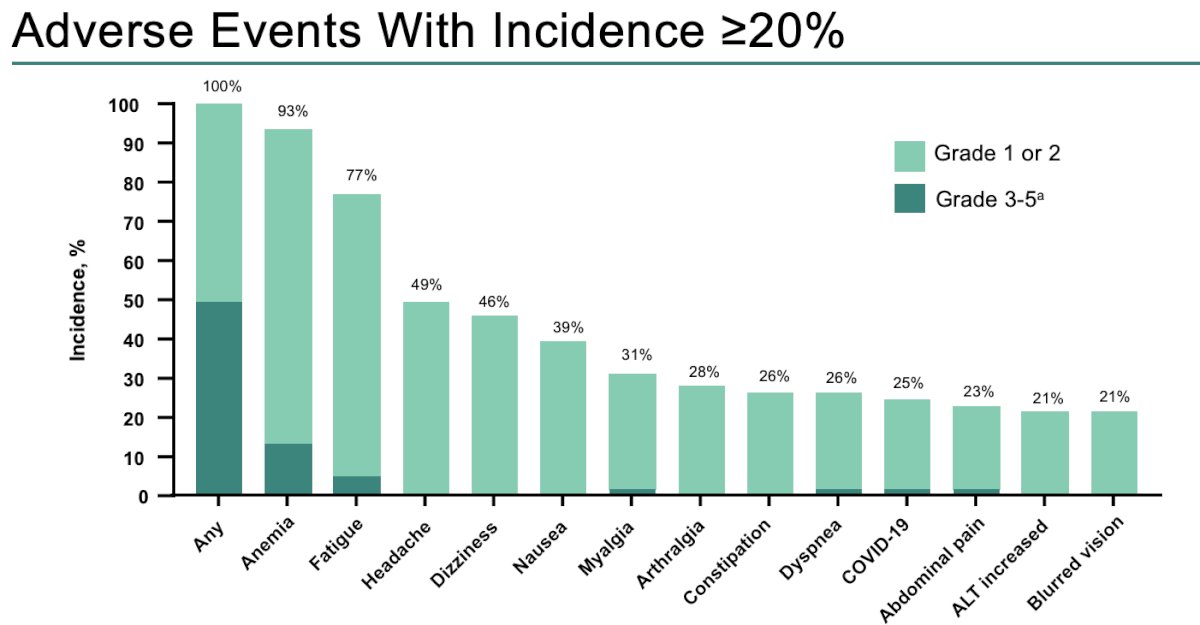
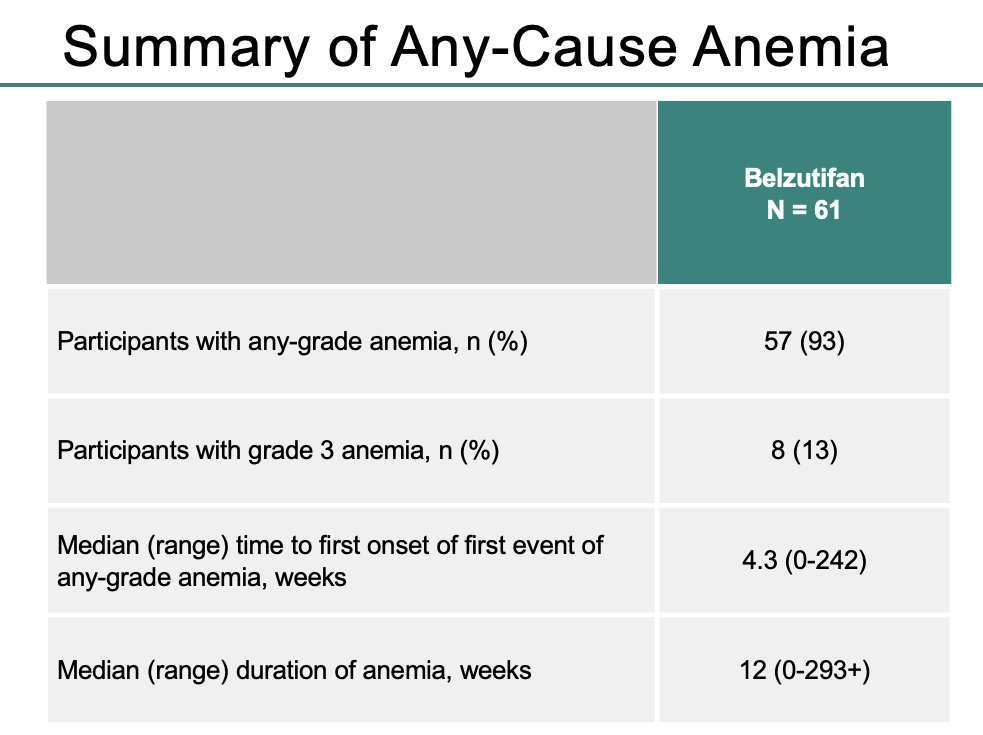
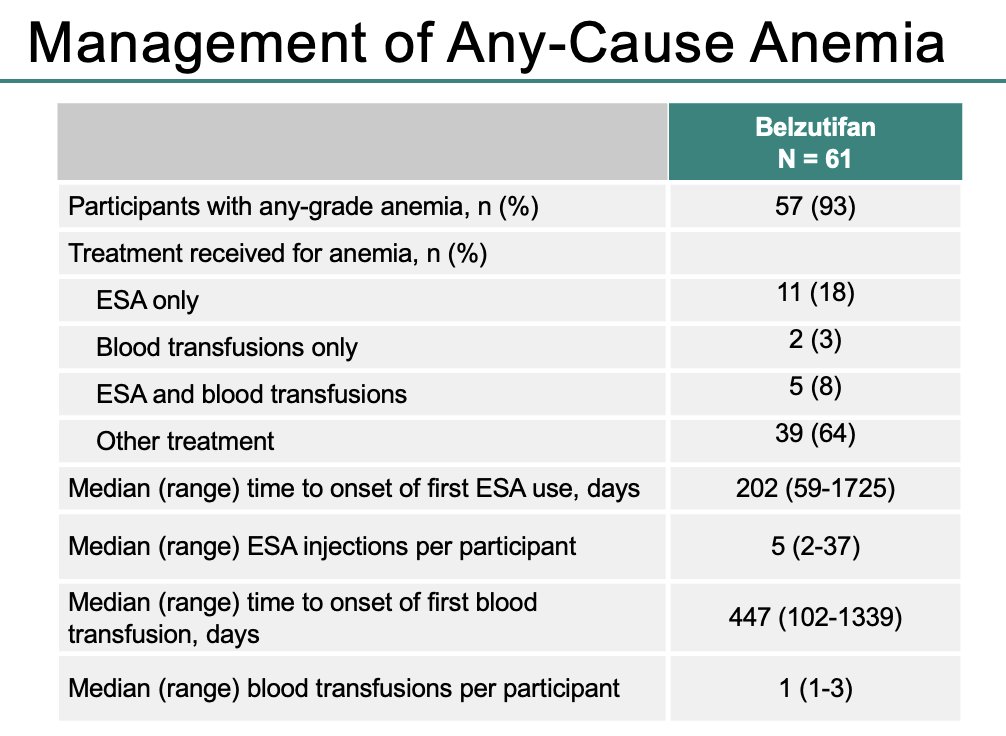
Anemia was the most common adverse event and occurred in 57 participants (93%). Eight patients (13%) experienced grade 3 anemia. The median time to 1st onset of any-grade anemia was ~1 month.
Five patients (8%) required both erythropoietin stimulating agents (ESAs) and blood transfusions, two (3%) required blood transfusions only, and 11 (18%) required ESA only.
Dr. Narayan concluded his presentation of the updated results from the LITESPARK-004 trial as follows:
- With a median study follow-up of 61.8 months, belzutifan continues to show clinically meaningful efficacy and durable responses in participants with VHL disease–associated RCC and other associated neoplasms
- ORR was 70% in RCC, 50% in CNS hemangioblastoma, and 90% in pNETs
- All 14 participants with retinal hemangioblastoma showed improvement
- The response was durable, and most participants who had an objective response remained in response at 48 months
- These results suggest that belzutifan may delay or reduce the need to undergo surgical procedures
- No new safety signals were observed with additional follow-up
- 35 participants (57%) remained on treatment as of the data cutoff date
- Belzutifan is the only approved systemic treatment option for patients with VHL disease–associated RCC, pNETs, or CNS hemangioblastoma that does not necessitate immediate surgery
Presented by: Vivek Narayan, MD, MS, Assistant Professor of Medicine (Hematology-Oncology), Hospital of the University of Pennsylvania, Philadelphia, PA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Belzutifan Demonstrates Durable Activity in VHL Disease Tumors - Vivek Narayan
- Jonasch E, Donskov F, Iliopoulos O, et al. Belzutifan for renal cell carcinoma in von Hippel–Lindau disease. N Engl J Med. 2021;385:2036–46.