(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a biomarkers in kidney cancer session. Dr. Axel Bex presented an exploratory analysis of NEOAVAX, a neoadjuvant trial of avelumab + axitinib in patients with localized renal cell carcinoma (RCC), who are at high risk of relapse after nephrectomy.
Dr. Bex noted that adjuvant pembrolizumab is the standard of care for patients with clear cell RCC at high risk of recurrence following a radical or partial nephrectomy.1,2 Neoadjuvant therapy in this setting has been investigated, but results, to date, have been underwhelming, and no agent is approved in this setting.
NEOAVAX (NCT03341845) is an open label, single arm, phase II trial investigating 12 weeks of neoadjuvant avelumab + axitinib prior to nephrectomy in patients with high-risk, non-metastatic clear cell RCC. The primary endpoint, a radiographic partial response by RECIST 1.1 criteria in the primary tumor in ≥25%, was met and previously reported, together with safety and tolerability.3 Herein, Dr. Bex reported updated disease-free (DFS) and overall survival (OS) results and exploratory endpoints associated with diverging clinical behavior.
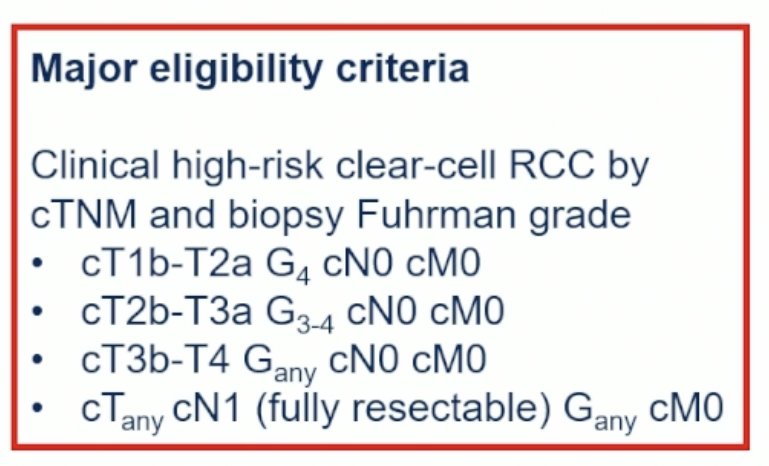
This single arm phase II trial enrolled adult patients with clinically high-risk clear cell RCC, meeting the following criteria:
- cT1b-2a, Grade 4
- cT2b-3a, Grade 3-4
- cT3-4, any grade
- cTanyN1, if resectable
Following enrollment, patients received 12 weeks of neoadjuvant avelumab and axitinib prior to nephrectomy. Forty patients were needed to detect a 25% primary tumor partial response rate with an alpha of 0.05 and a power of 80%, using a Simon 2-sage minimax design.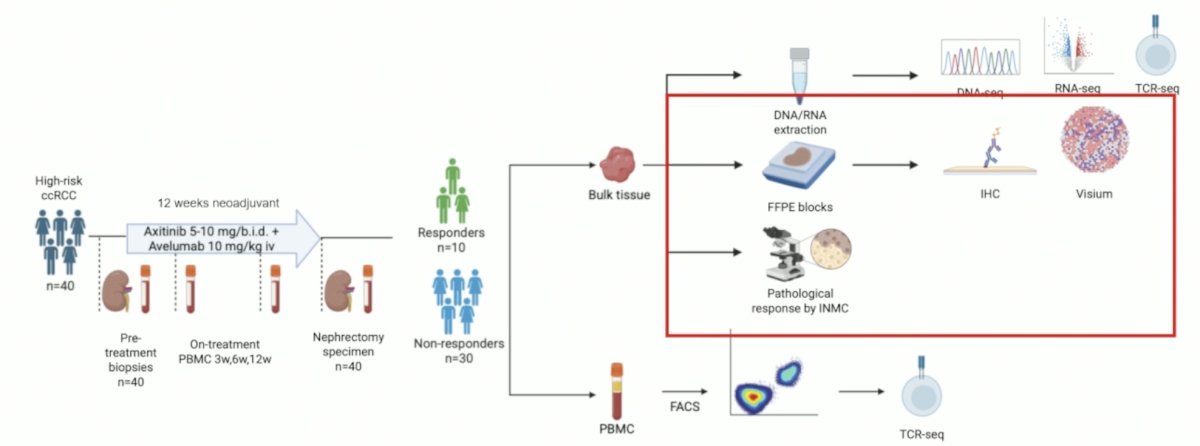
The secondary endpoints of DFS and OS were assessed at the data cut-off date of April 30, 2025, at a median follow-up of 53 months. The exploratory endpoints were:
- Pathologic response by the International Neoadjuvant Melanoma Consortium (INMC) criteria and association with radiologic (RECIST 1.1) response
- The INMC were used as there are no analogous validated criteria for evaluation of pathologic responses in the primary RCC tumor
- Association of RECIST 1.1 and pathologic response with DFS and OS
- Association of DFS with Multiplex IHC signatures in paired tumor samples (pre-treatment biopsy and nephrectomy) from 40 patients
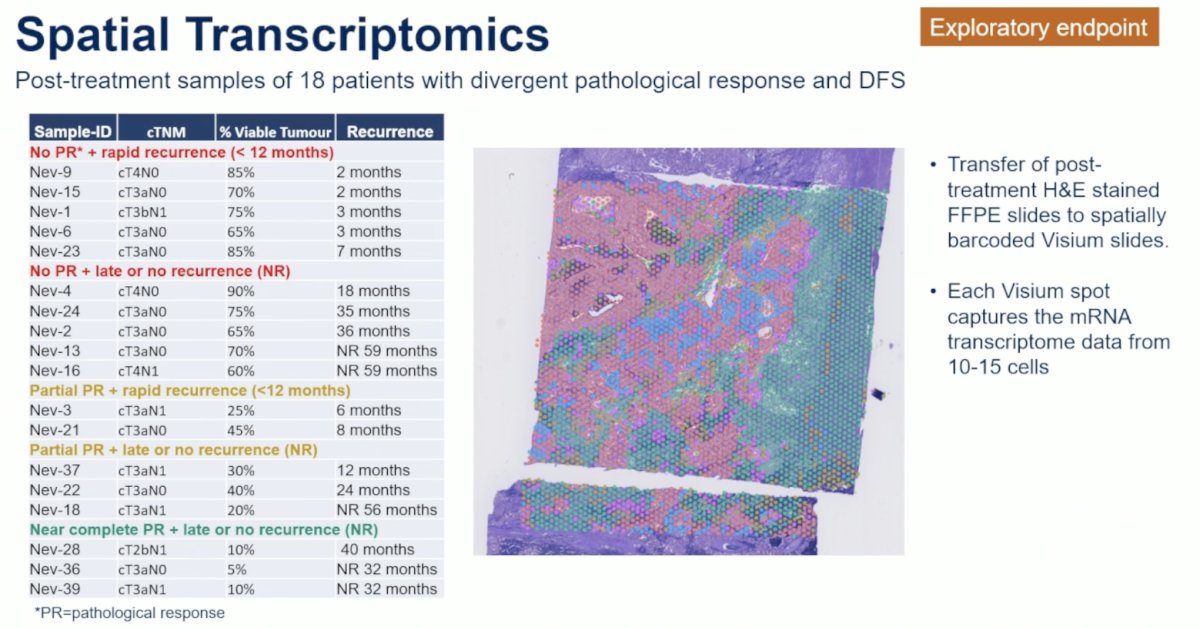
- Visium v2 spatial transcriptomics in post-treatment tumor samples of 18 patients with divergent pathologic response and DFS outcomes
The baseline patient characteristics are summarized below. The median age was 63 years. 70% of patients were male. This trial was appropriately enriched for high-risk patients with 90% of patients having cT3-4 disease, and 43% had cN+ disease. The baseline tumor diameter was 10.3 cm.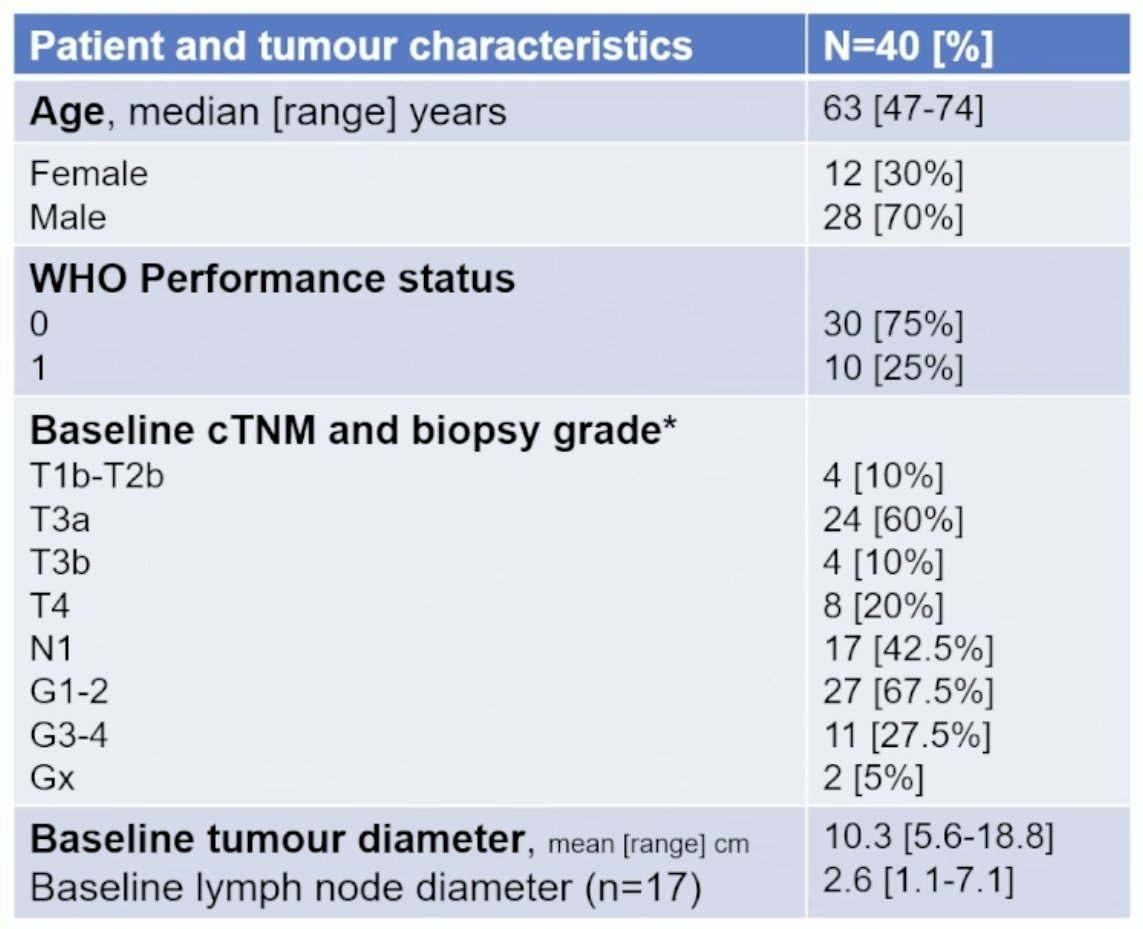
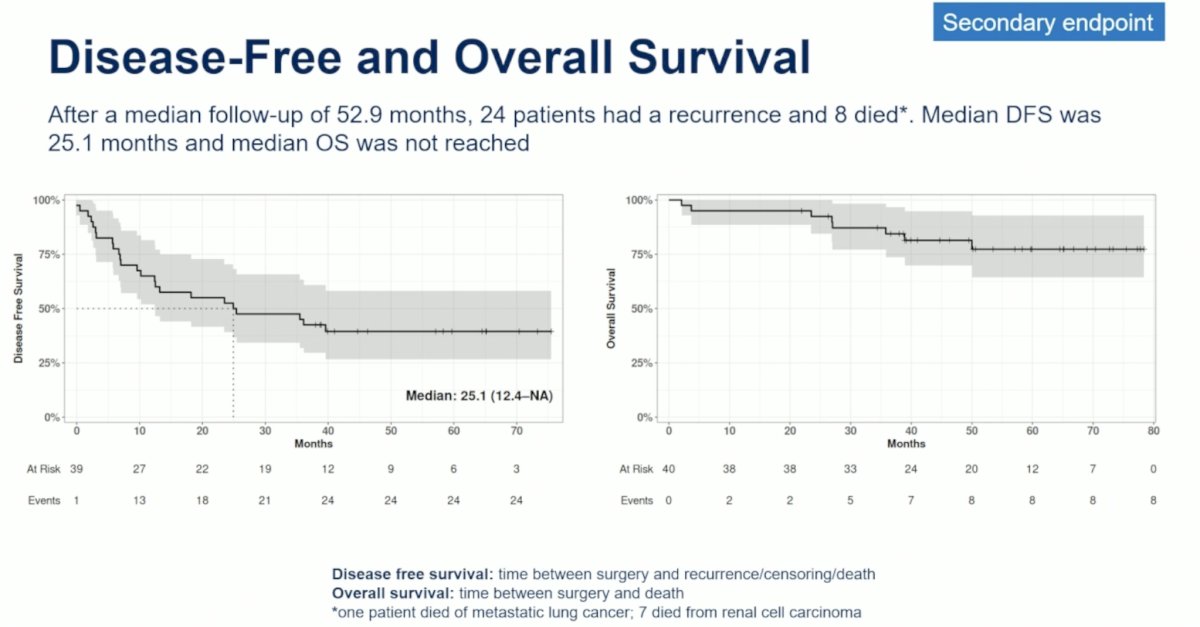
After a median follow-up of 53 months, 24 patients experienced disease recurrence and 8 died. The median DFS was 25.1 months, and the median OS has not been reached.
Patients with a radiologic response (i.e., responders) had superior DFS (median: 35.5 versus 20.9 months; HR: 0.61, p=0.33) and OS, although the p-values for both were >0.05 (0.33 and 0.071, respectively).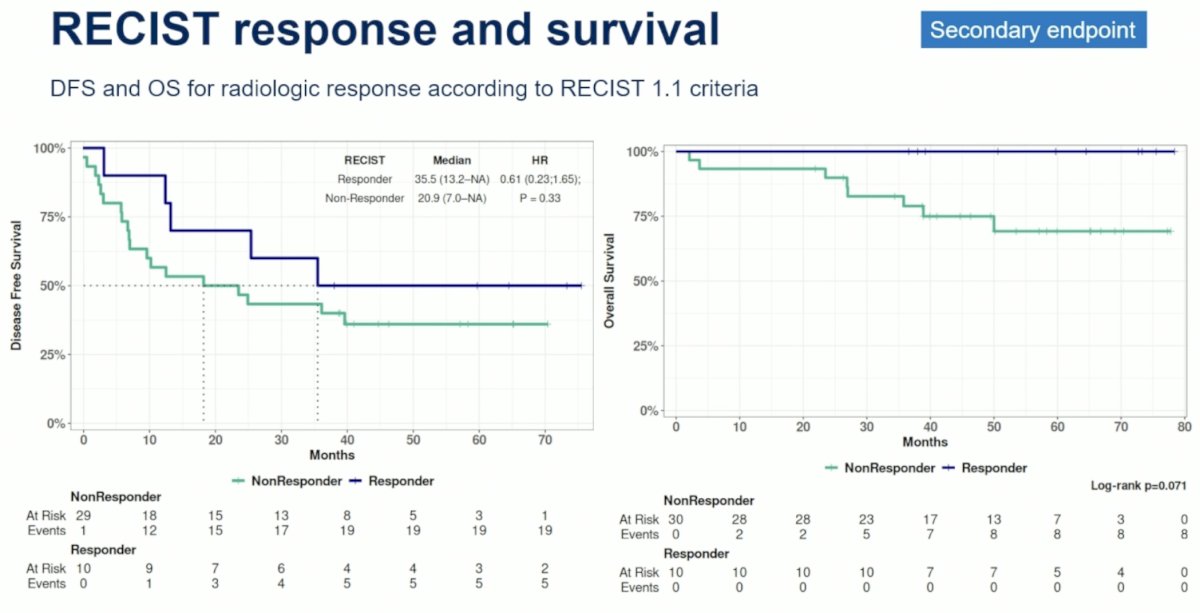
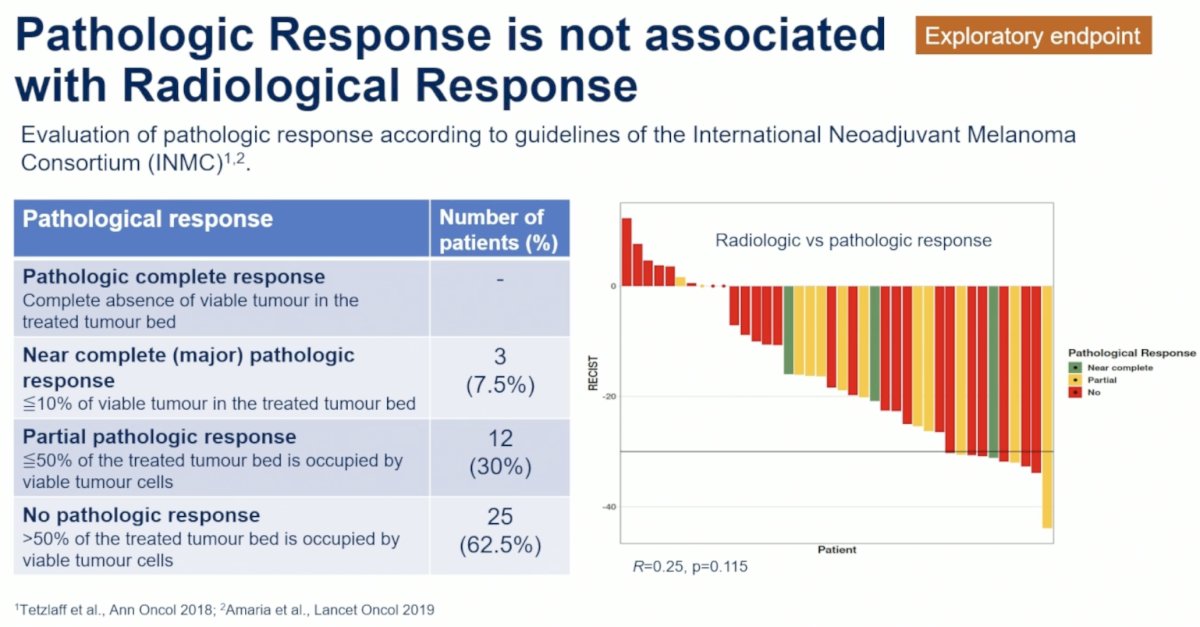
Notably, pathologic response was not associated with radiologic response. No patient had a pathologic complete response, but 3 (7.5%) and 12 (30%) had near complete (i.e., major) or partial pathologic responses, respectively.
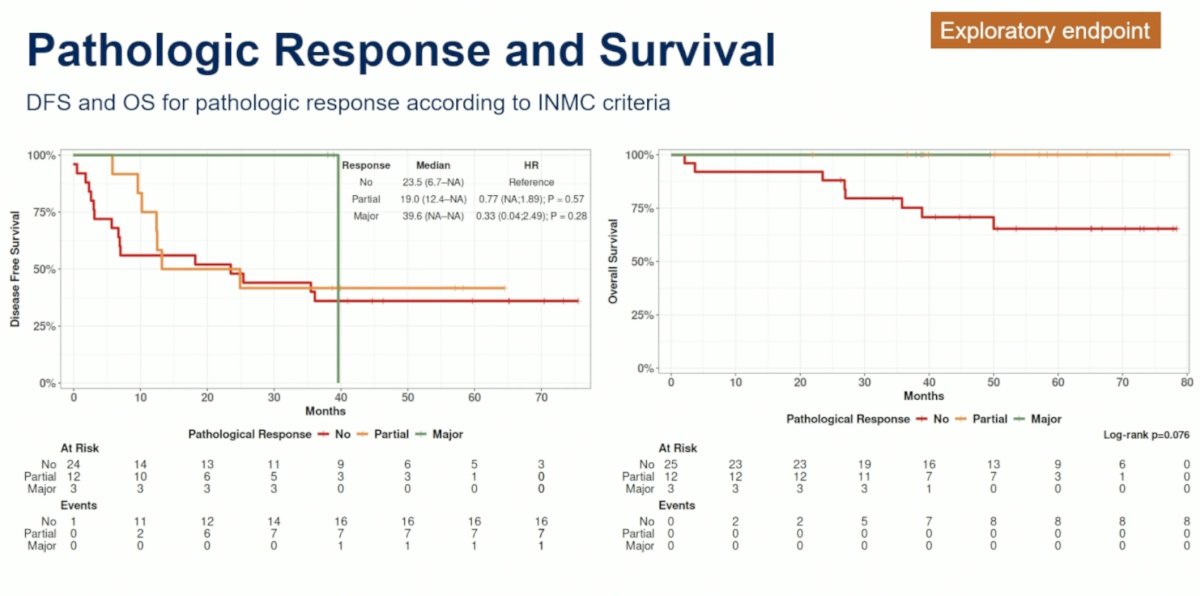
While sample size was limited and no robust statistical inferences could be made, patients with a major pathologic response had numerically superior DFS (median: 39.6 months), compared to patients with no (median: 23.5 months) or partial pathologic responses (median: 19 months). To date, no patient with a major or partial pathologic response has died.
Post-treatment samples of 18 patients with divergent pathologic responses and DFS outcomes were used for spatial transcriptomics.
Nine tumor clusters were identified: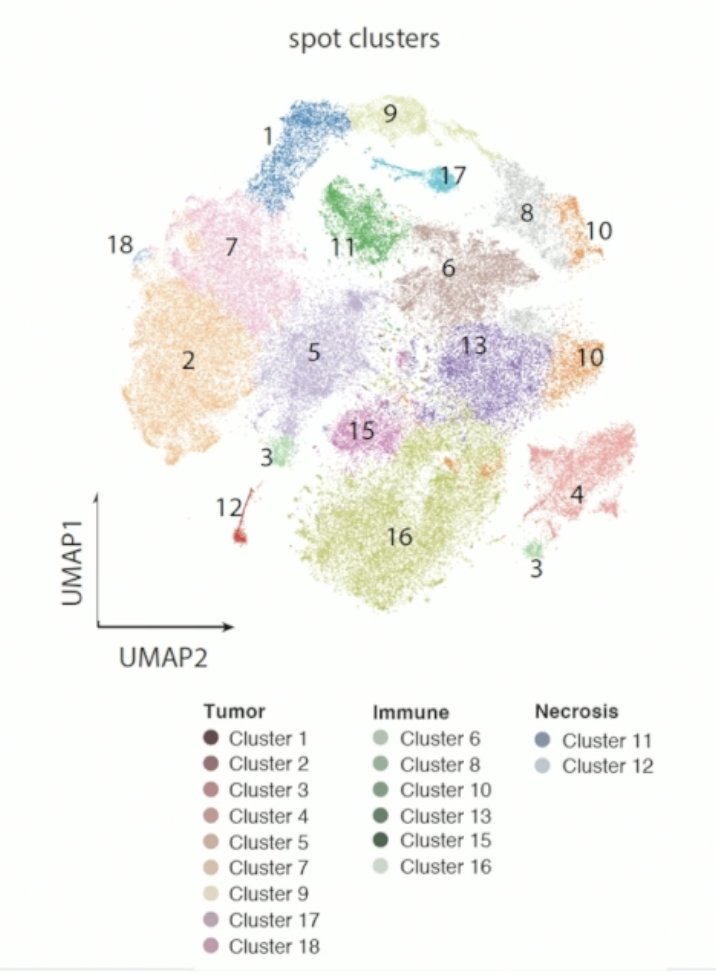
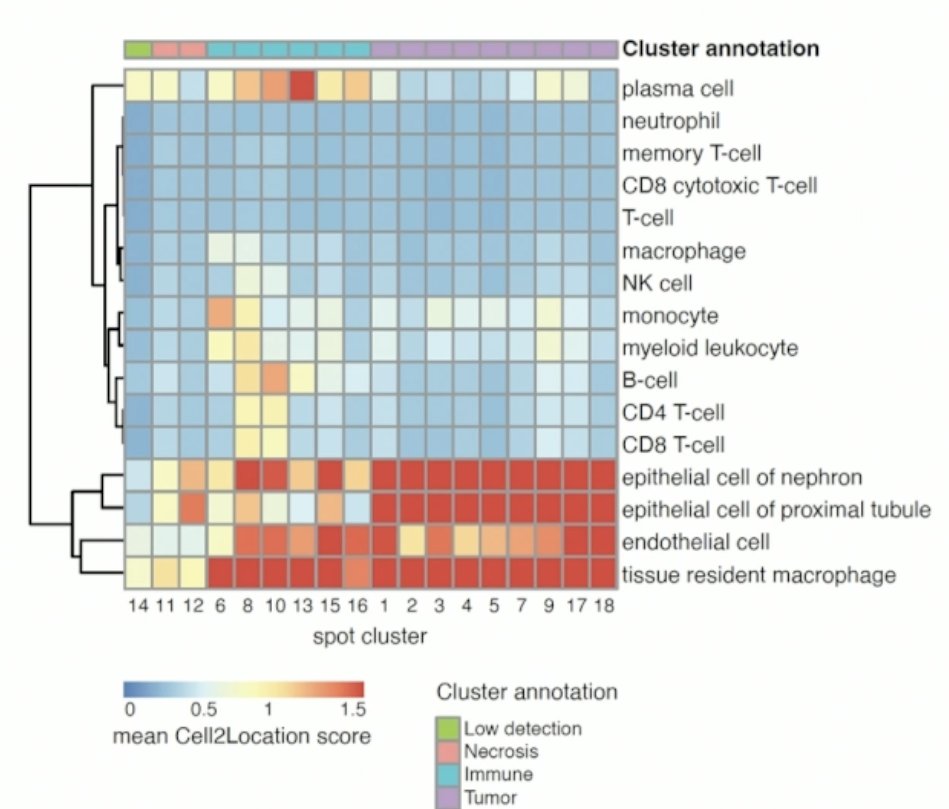
The heatmap below displays the mean Cell2Location score across all spots in each of the Visium spot clusters.
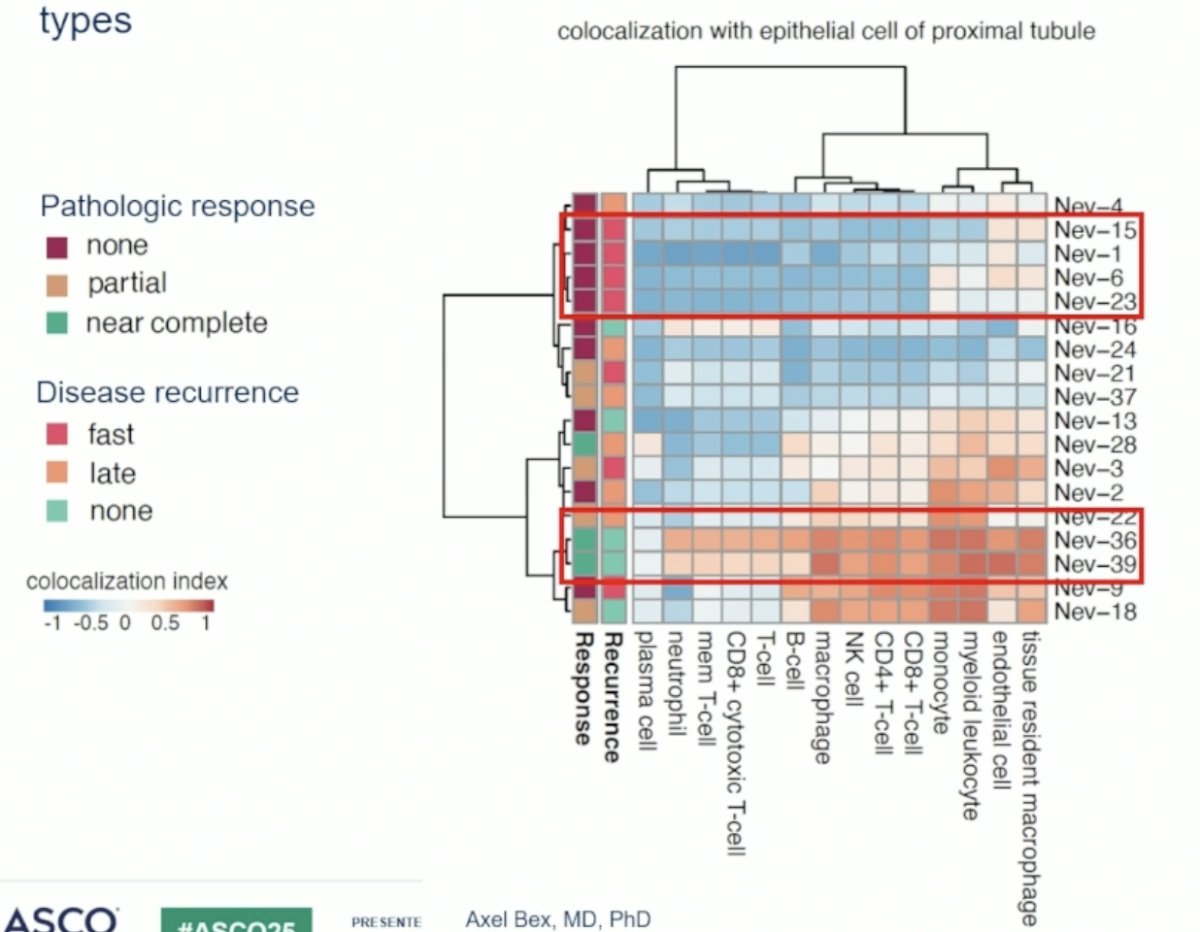
Spatial co-localization analysis of proximal tubule epithelial cells and immune cell types demonstrated:
- In tumors with a major pathologic response, spatial co-localization of tumor cells with tissue-resident macrophages, CD8+ cytotoxic T-cells, memory T-cells, and B-cells was observed
- In tumors with no pathologic response and rapid disease recurrence, co-localization with these immune cells is largely absent
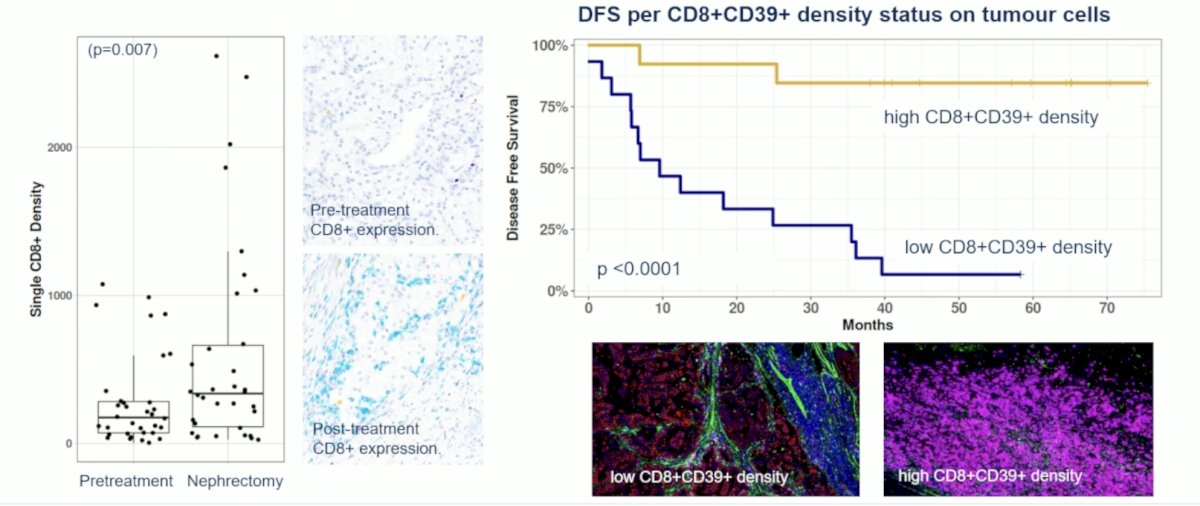
On multiplex immunohistochemistry, an influx of CD8+CD39+ tumor-reactive T-cells among post-treatment tumor cells was shown to be associated with prolonged DFS.
Dr. Bex concluded his presentation of the NEOAVAX trial as follows:
- Twelve weeks of neoadjuvant avelumab and axitinib for non-metastatic clear cell RCC lead to clinical and pathological tumour responses, which provides prognostic information.
- Major pathologic response (MPR; ≤10% viable tumour) does occur in primary tumors, albeit infrequently.
- In patients with MPR, long-term DFS and immune response in the tumour microenvironment are observed. In contrast, pathologic non-responders have a poorer prognosis and show less prominent co-localization of immune and tumour cells.
- Influx of CD8+CD39+ T-cells among post-treatment tumor cells associates with prolonged DFS and may represent a predictive biomarker.
- Radiologic and pathologic response as well as post-treatment tumour infiltrating lymphocyte signatures in the primary tumour could be used to design perioperative adaptive trials and investigate personalized treatment approaches.
Presented by: Axel Bex, MD, PhD, Netherlands Cancer Institute Antoni Van Leeuwenhoek, The Netherlands
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Choueiri TK, Tomczak P, Park SH, et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med. 2021; 385(8):683-694.
- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Chang YH, et al. Overall survival with adjuvant pembrolizumab in renal-cell carcinoma. N Engl J Med. 2024; 390(16):1359–1371.
- Bex A, Grünwald V, Albers P, et al. A phase II trial of neoadjuvant nivolumab and vaccine (NEO-NIVO-VAC) in high-risk localized renal cell carcinoma (NEOVAX). J Clin Oncol. 2022; 40(16_suppl):289.