(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to a State of the Science session on novel diagnostics and therapeutics in renal cell and urothelial carcinomas. Dr. Rana McKay discussed HIF-2α targeting as a new frontier in renal cell cancer (RCC) therapy.
Von Hippel-Lindau (VHL) gene mutations drive pathogenesis in RCC. The VHL tumor suppressor gene was identified in 1993, and mutations of the VHL gene were later found to be very common in clear cell RCC (~78%).1

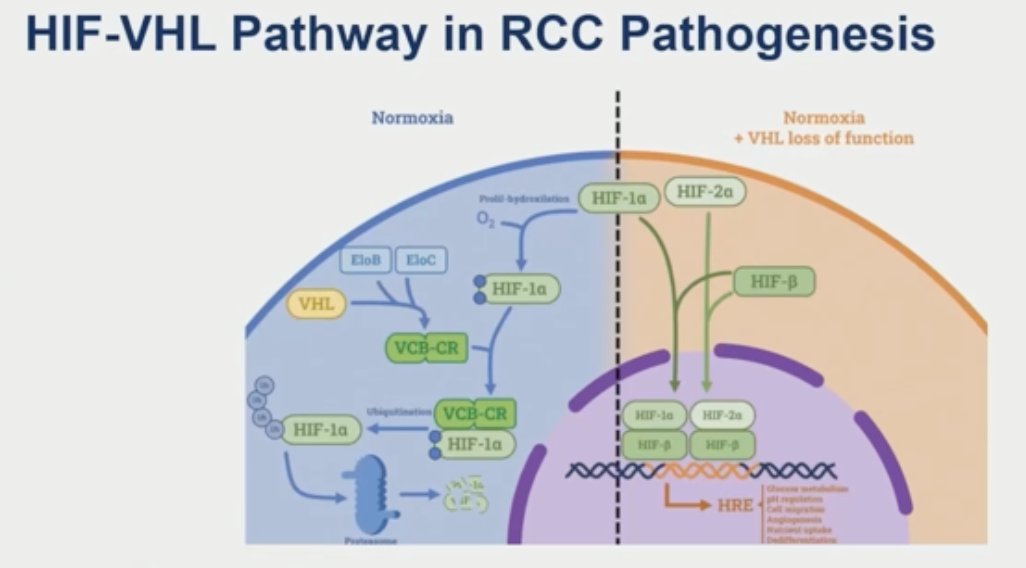
The HIF-VHL pathway is critical to RCC pathogenesis. Under normal oxygen conditions, VHL causes ubiquitination of HIF and targets it for proteosomal degradation. However, when VHL is lost, HIF accumulates in the cell – the alpha and beta units dimerize, translocate into the nucleus, and bind to the hypoxia response elements, causing activation of downstream target genes. This leads to increased angiogenesis, cell survival, tumor growth, and all other hallmarks of RCC development.
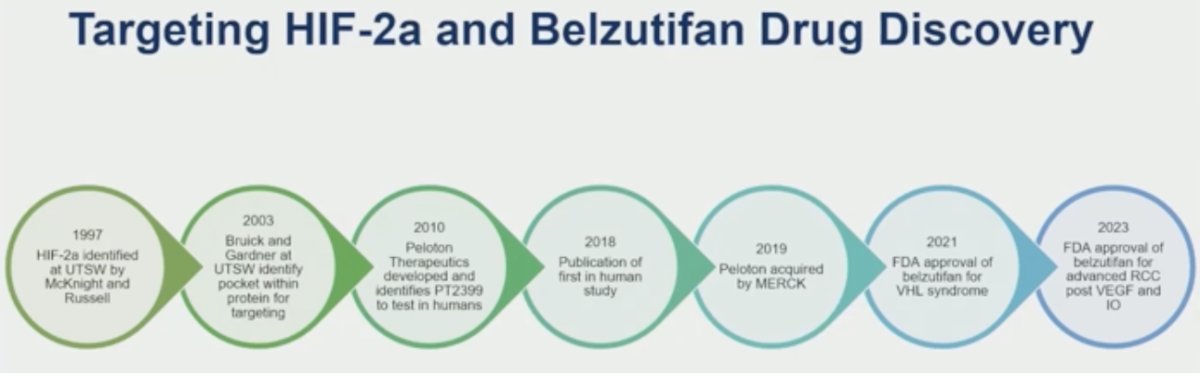
The 26-year timeline of targeting HIF-2α and belzutifan drug discovery is illustrated below:
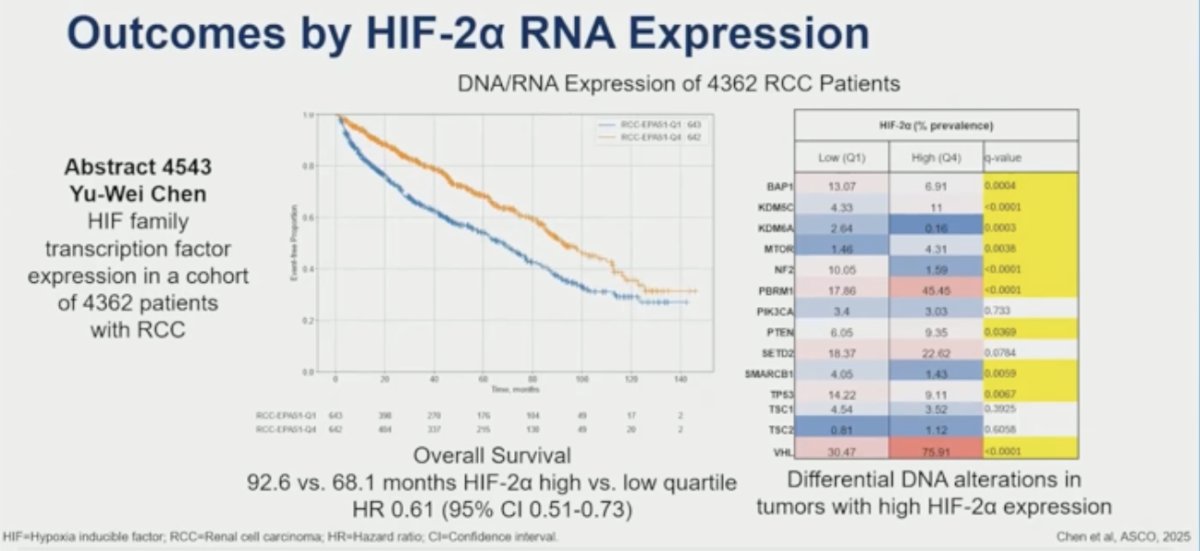
HIF-2α RNA expression is prognostic in RCC. In data from the University of Toronto presented during ASCO 2025, Chen et al. evaluated HIF family transcription factor expression in a cohort of 4,632 patients with RCC. Patients in the highest HIF-2α expression quartile had superior overall survival (OS) compared to those in the lowest expression quartile: 92.6 versus 68.1 months (HR: 0.61; 95% CI: 0.51–0.73). Additionally, tumors with high HIF-2α expression had unique DNA mutational profiles.
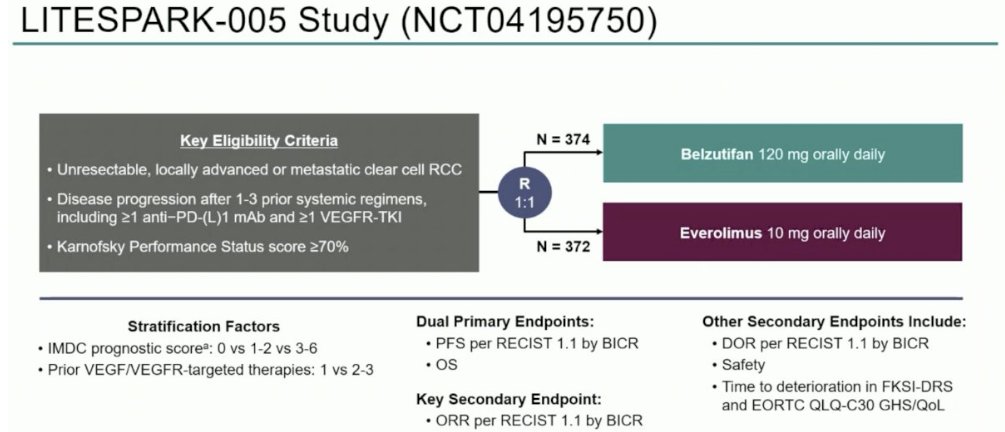
LITESPARK-005 (NCT04195750) is an open label, randomized phase III study of patients with unresectable, locally advanced, or metastatic ccRCC with evidence of disease progression after 1-3 lines of prior systemic therapy, including ≥1 anti-PD-(L)1 agent and ≥1 VEGFR-TKI. Patients in this study underwent 1:1 randomization to:
- Belzutifan 120 mg orally once daily (n=374)
- Everolimus 10 mg orally once daily (n=372)
66% and 12% of patients had IMDC intermediate- and poor-risk disease. The median number of prior therapies was 2, and 13% had received only 1 prior line of therapy. This trial met its primary endpoint with a progression-free survival (PFS) of 5.6 months in both arms (HR: 0.75, p<0.001). The median OS in the belzutifan arm was 21.4 months versus 18.1 months with everolimus (HR: 0.92, p=0.18). The ORR was 22.7% versus 3.5% for everolimus.2 The results of this study led to the approval of belzutifan for patients with advanced RCC following PD-1/L-1 and VEGFR-TKI therapy.3
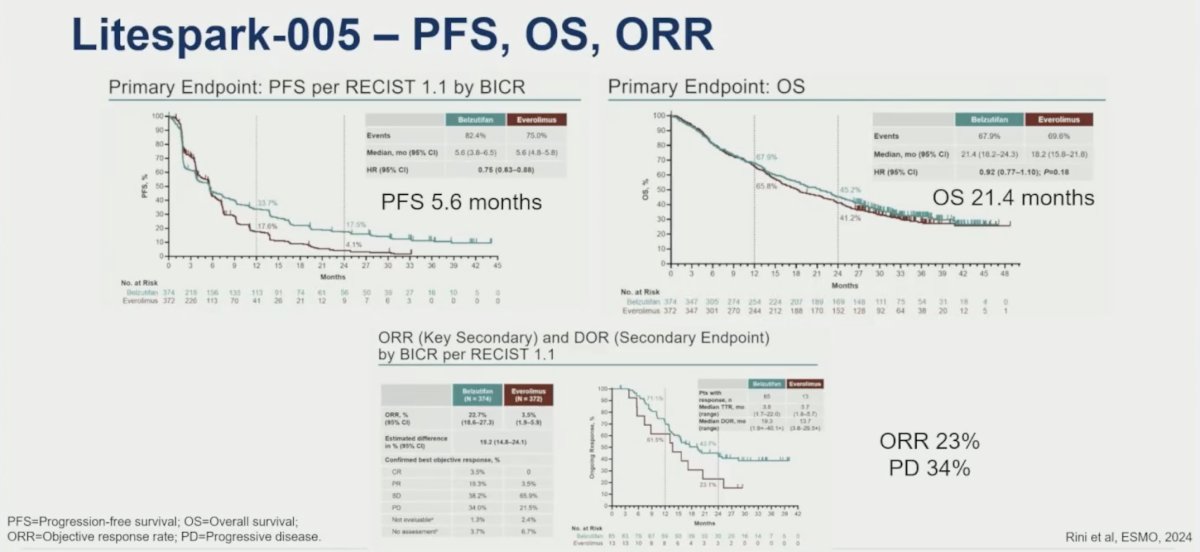
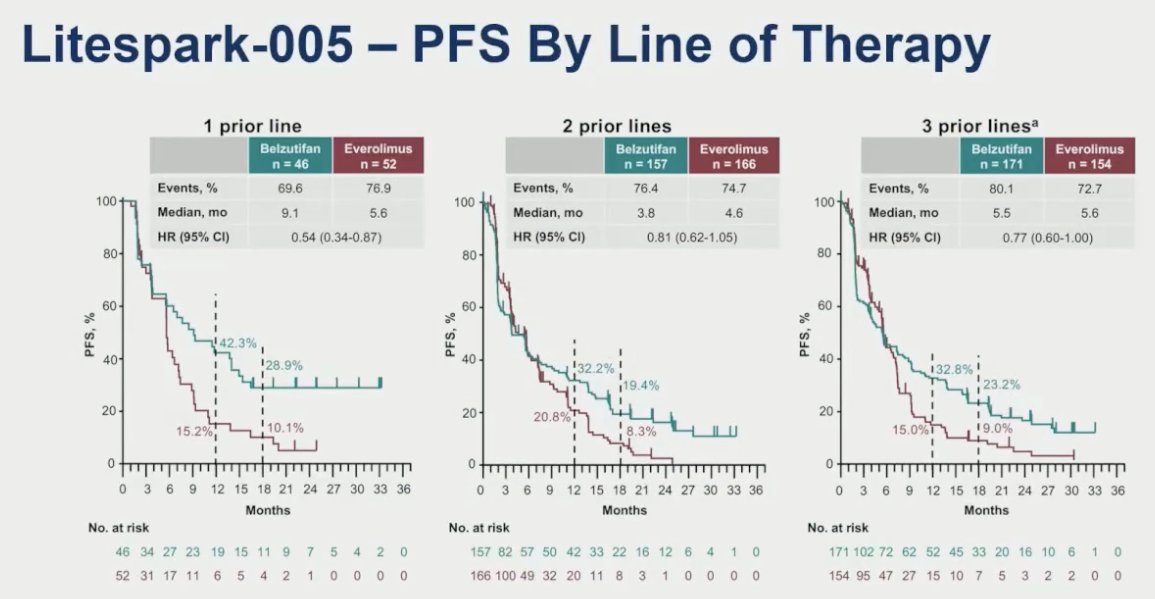
Post hoc analyses by lines of prior therapy demonstrated that the relative benefit of belzutifan was most pronounced for patients who had received 1 prior line of therapy (PFS, median: 9.1 vs 5.6 months; HR: 0.54, 95% CI: 0.34–0.87).
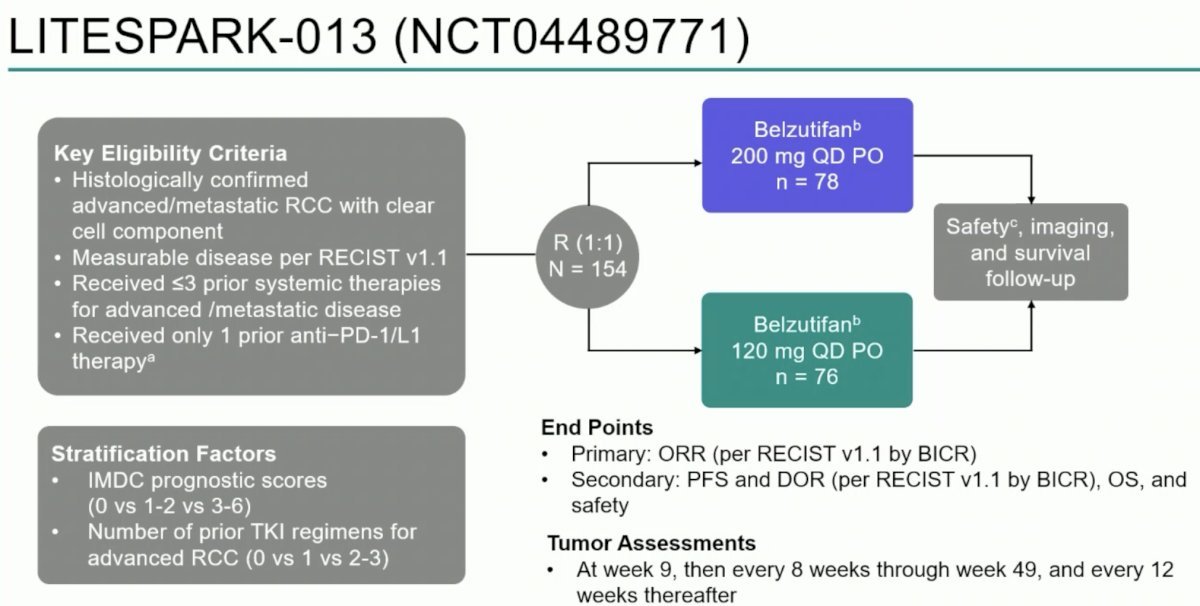
The phase II LITESPARK-013 study compared belzutifan 200 mg and 120 mg doses in patients with advanced clear cell RCC that progressed on anti-PD-1/L1 therapy in order to evaluate the safety and efficacy of these 2 doses in a larger, randomized trial. LITESPARK-013 (NCT04489771) included patients with histologically confirmed advanced/metastatic clear cell RCC who received ≤3 prior systemic therapy regimens for advanced/metastatic disease. Importantly, patients had received only 1 prior anti-PD-1/L-1 therapy. Patients underwent 1:1 randomization to:
- Belzutifan 200 mg orally once daily (n=78)
- Belzutifan 120 mg orally once daily (n=76)
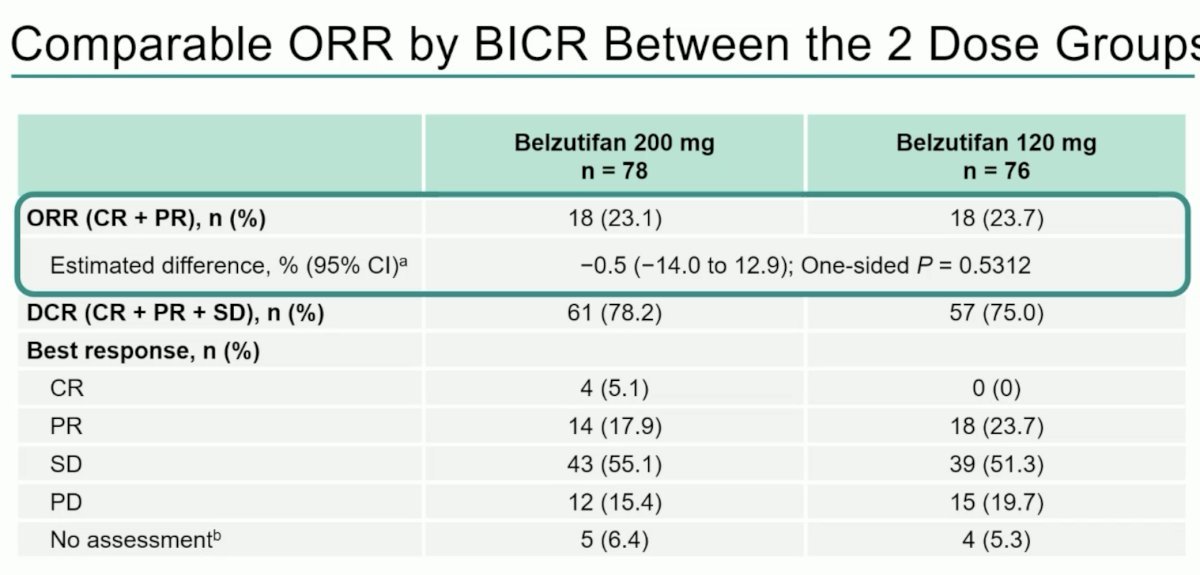
69% and 14% of patients had IMDC intermediate- and poor-risk disease, respectively. 47% of patients had received 1 prior line of therapy. Overall, there were no significant differences in efficacy outcomes between the two dosage groups. The ORR was similar in both arms at 23.1 – 23.7%. Of note, 4 patients (5.1%) in the belzutifan 200 mg dose group had a complete response, compared to none in the 120 mg group.4 Nonetheless, these results led to the adoption of belzutifan 120 mg as the standard treatment dose.
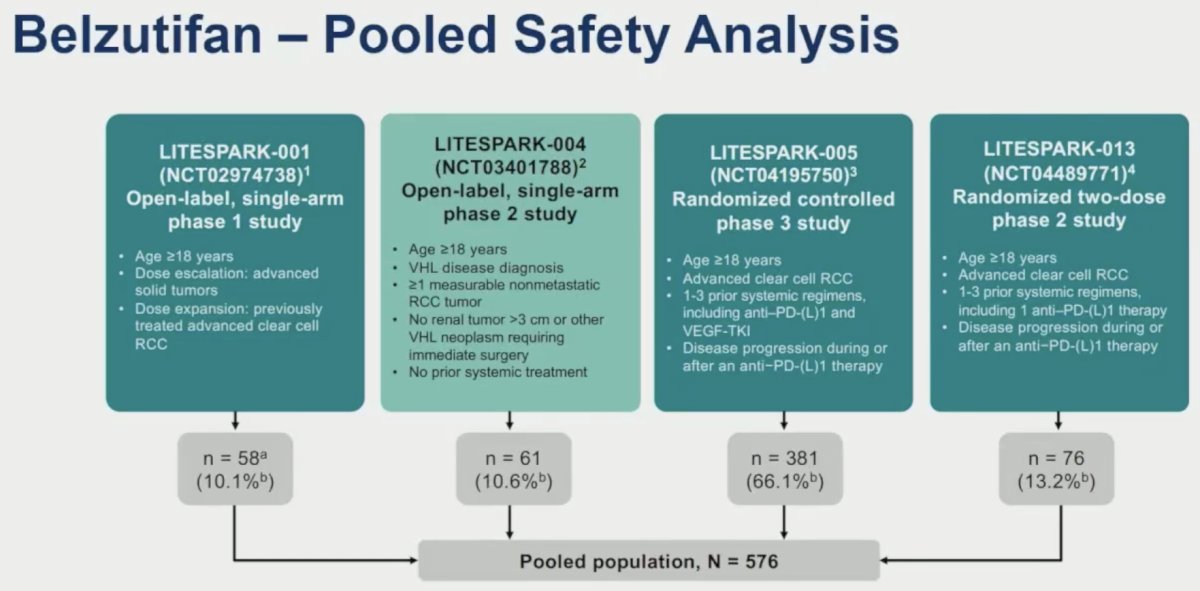
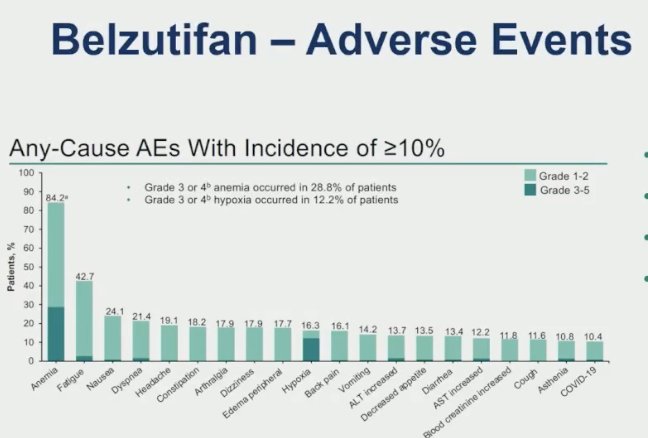
A pooled safety analysis of LITESPARK-001, LITESPARK-004, LITESPARK-005, and LITESPARK-013 demonstrated the following pooled adverse event profile for belzutifan:
- Any-cause grade 3-5 adverse events (AEs): 62%
- Treatment-related grade 3-5 AEs: 38%
- Treatment discontinuation: 6%
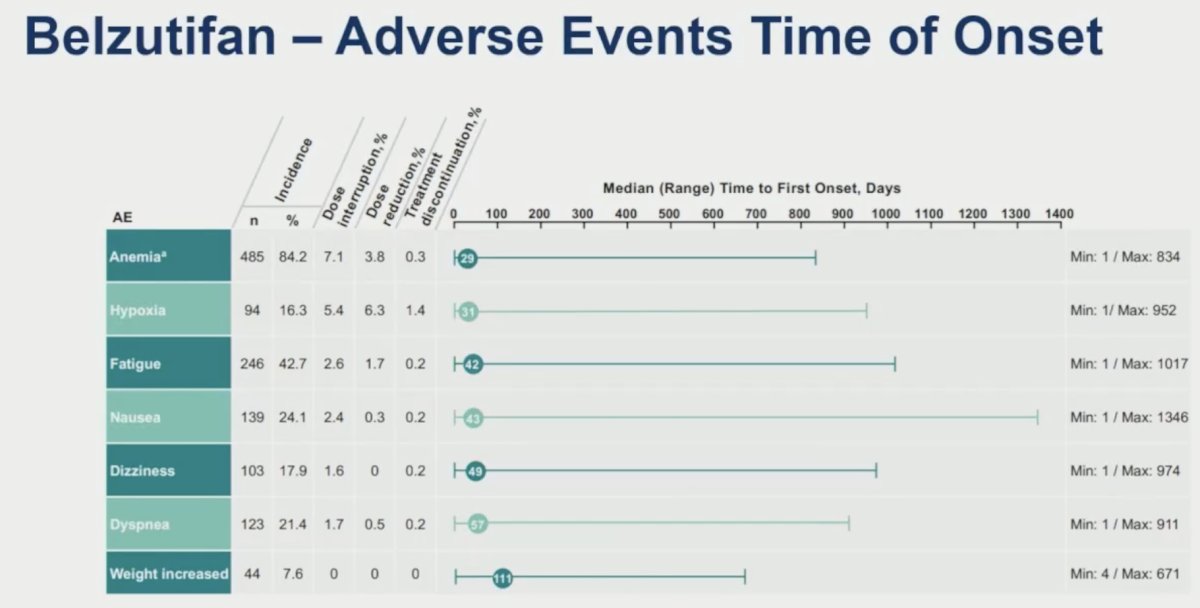
- Anemia management
- Erythropoietin-stimulating agent (ESA): 23%
- Blood transfusion: 18%
- ESA + blood transfusion: 13%
The median time to onset of most AEs was 1-2 months (anemia: 29 days; hypoxia: 31 days).
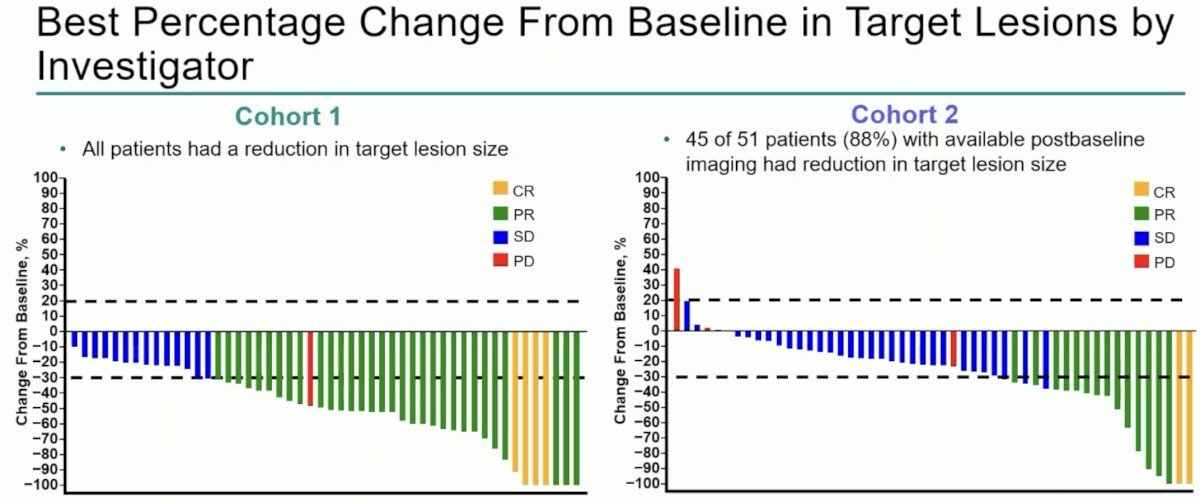
Next, Dr. McKay discussed LITESPARK-003, which evaluated the combination of belzutifan + cabozantinib. This phase II trial assigned patients with locally advanced or metastatic clear cell RCC (treatment-naïve or previously treated) to belzutifan 120 mg orally once daily plus cabozantinib 60 mg orally once daily. Cohort 1 included treatment-naïve patients, whereas Cohort 2 included pre-treated patients.
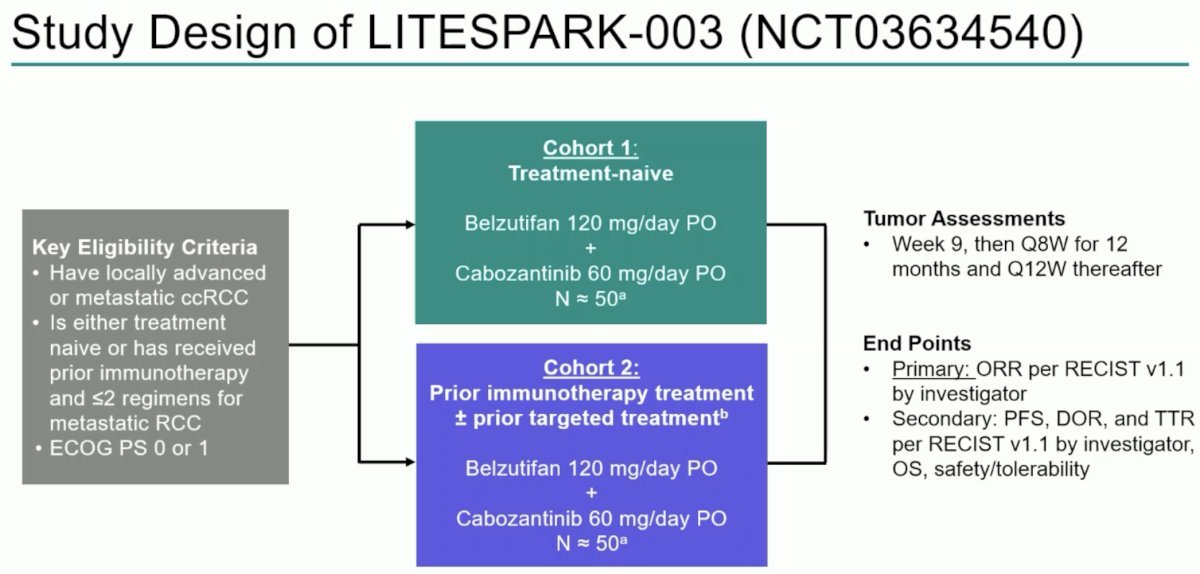
For the primary outcome of investigator-assessed ORR, 70% of patients in Cohort 1 had an ORR (complete or partial response). In Cohort 2, the ORR was 31%.
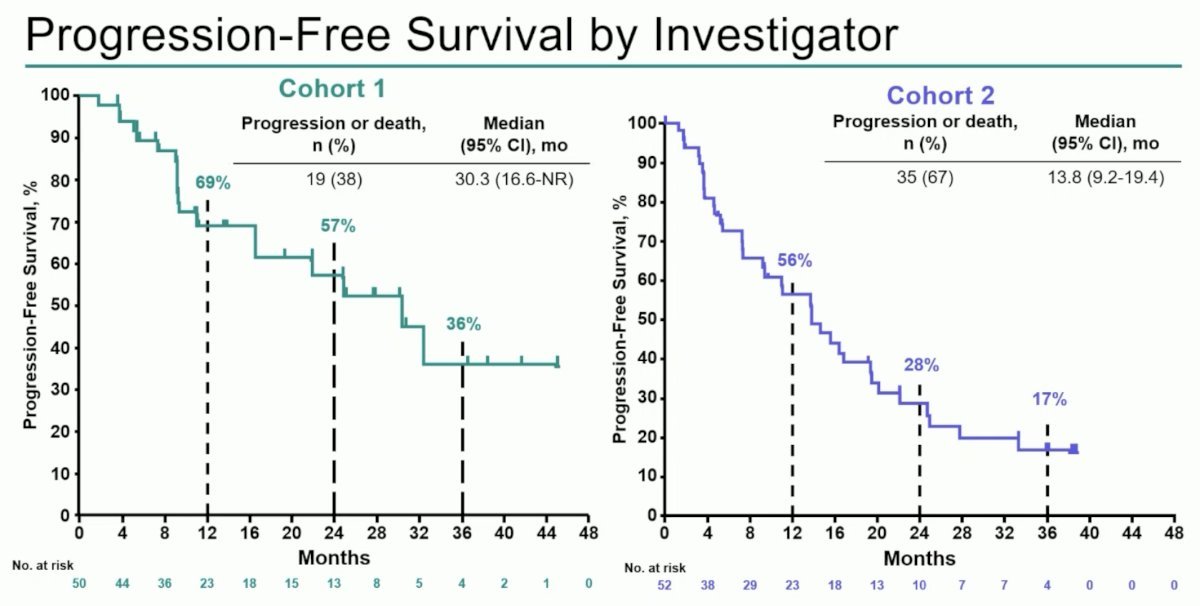
Investigator-assessed PFS is summarized for each cohort in the Kaplan Meier curves below. The median PFS was 30.3 months in Cohort 1 and 13.8 months in Cohort 2.5
The LITESPARK-011 trial is randomizing patients with advanced or metastatic clear cell RCC who experienced disease progression after 1st or 2nd line anti-PD-1/L-1 therapy and who had received ≤2 prior systemic therapies to:
- Belzutifan 120 mg orally once daily + lenvatinib 20 mg orally once daily
- Cabozantinib 60 mg orally once daily
This trial has completed accrual and results are expected soon.

LITESPARK-012 is evaluating belzutifan combinations in the 1st line setting, whereby treatment-naïve patients with advanced or metastatic clear cell RCC are being randomized 1:1:1 to:
- Arm A: Belzutifan 120 mg daily + pembrolizumab 400 mg IV every 6 weeks + lenvatinib 20 mg daily
- Arm B: Quavonlimab 25 mg/pembrolizumab 400 mg IV every 6 weeks + lenvatinib 20 mg daily
- Arm C: Pembrolizumab 400 mg IV every 6 weeks + lenvatinib 20 mg daily
The co-primary endpoints are PFS and OS.
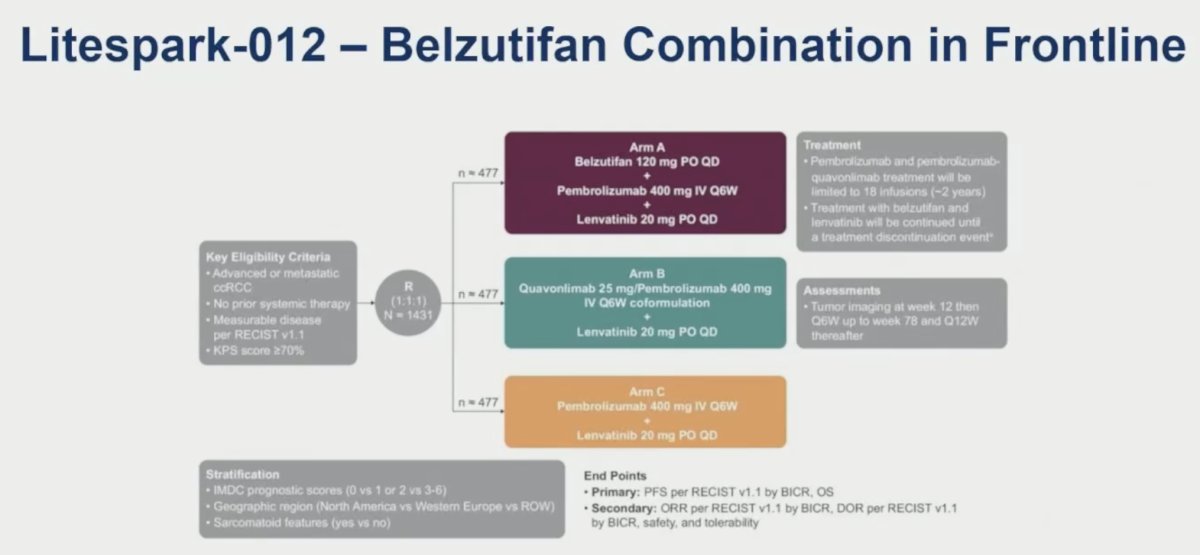
This study has also completed accrual, and results are expected soon.
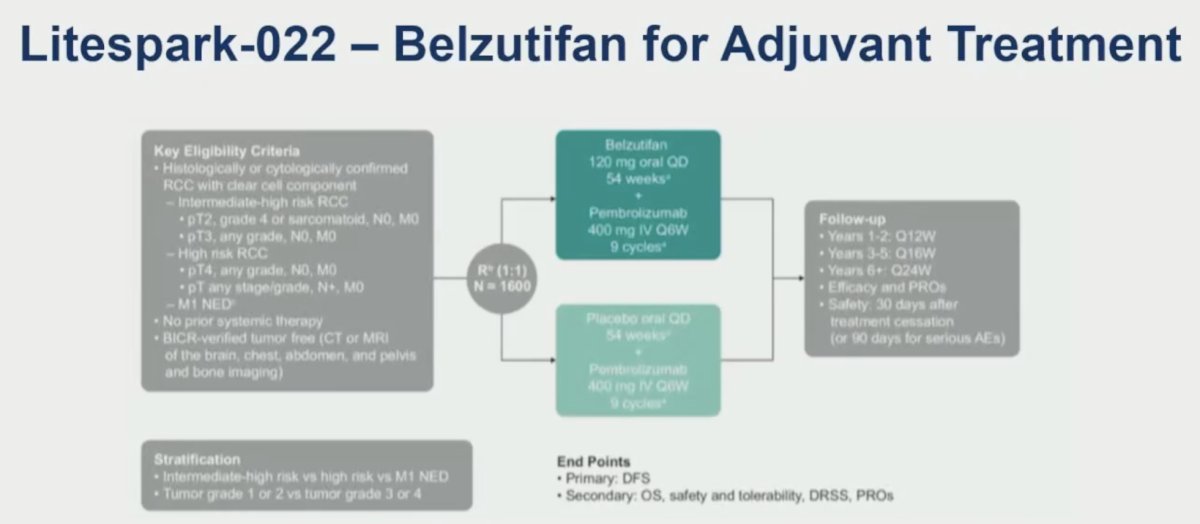
Moving to the adjuvant setting, the phase III LITESPARK-022 trial compares adjuvant pembrolizumab plus belzutifan with adjuvant pembrolizumab alone in intermediate-high and high-risk clear cell RCC patients following nephrectomy. The primary endpoint is disease-free survival (DFS), with OS a key secondary endpoint. Results are expected in 2027.
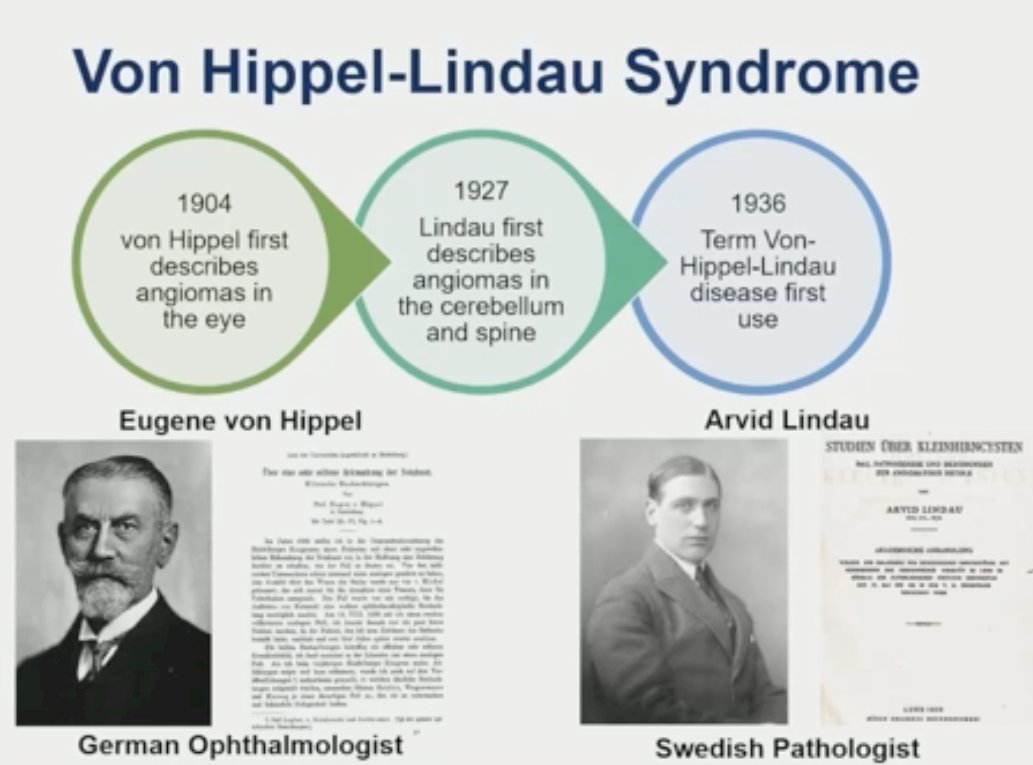
Now shifting to discuss the VHL syndrome in further detail, Dr. McKay noted that in 1904, Dr. Eugene von Hippel, a German ophthalmologist, 1st described angiomas in the eye. In 1927, Arvid Lindau, a Swedish pathologist, 1st described angiomas in the cerebellum and spine. In 1936, the term Von Hippel-Lindau disease was 1st used.
VHL is an autosomal dominant syndrome, with 80% of patients having an affected parent, while 20% arise de novo. Nearly all patients will express the syndrome by age 65. The incidence of this syndrome is 1 in 36,000, and roughly two-thirds will develop an RCC.
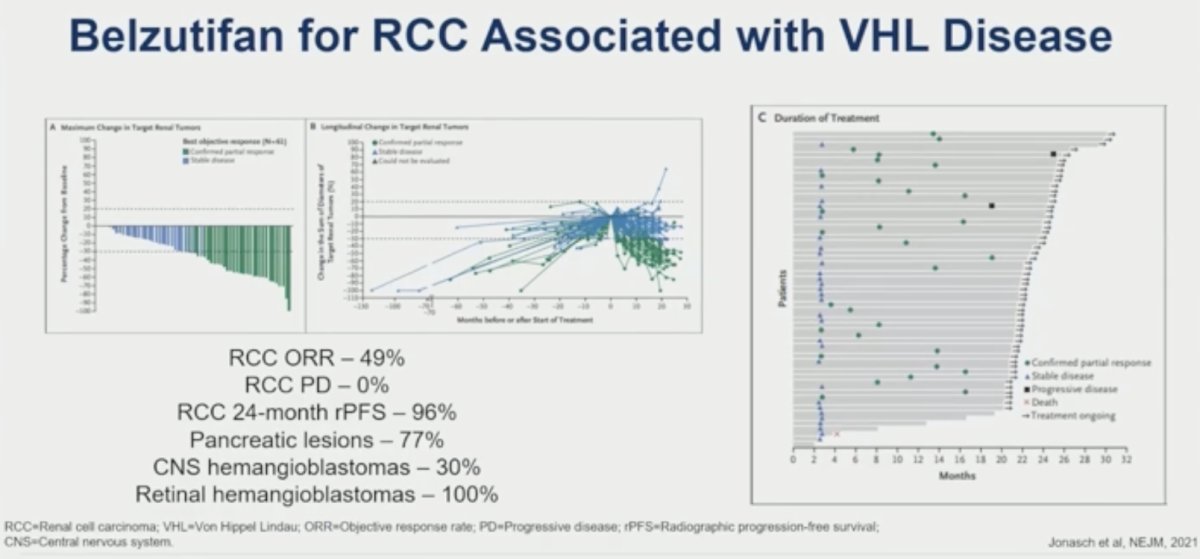
The LITESPARK-004 (MK-6482-004) phase II trial evaluated the efficacy and safety of belzutifan 120 mg orally once daily in patients with RCC associated with VHL disease. After a median follow-up of 21.8 months, the ORR (primary endpoint) was 49%. None of the patients experienced progressive disease. The RCC 24-months rPFS was 96%.
Responses were also observed in patients with pancreatic lesions (77%) and central nervous system hemangioblastomas (30%). Among the 16 evaluable eyes in 12 patients with retinal hemangioblastomas at baseline, all (100%) were graded as showing improvement.6
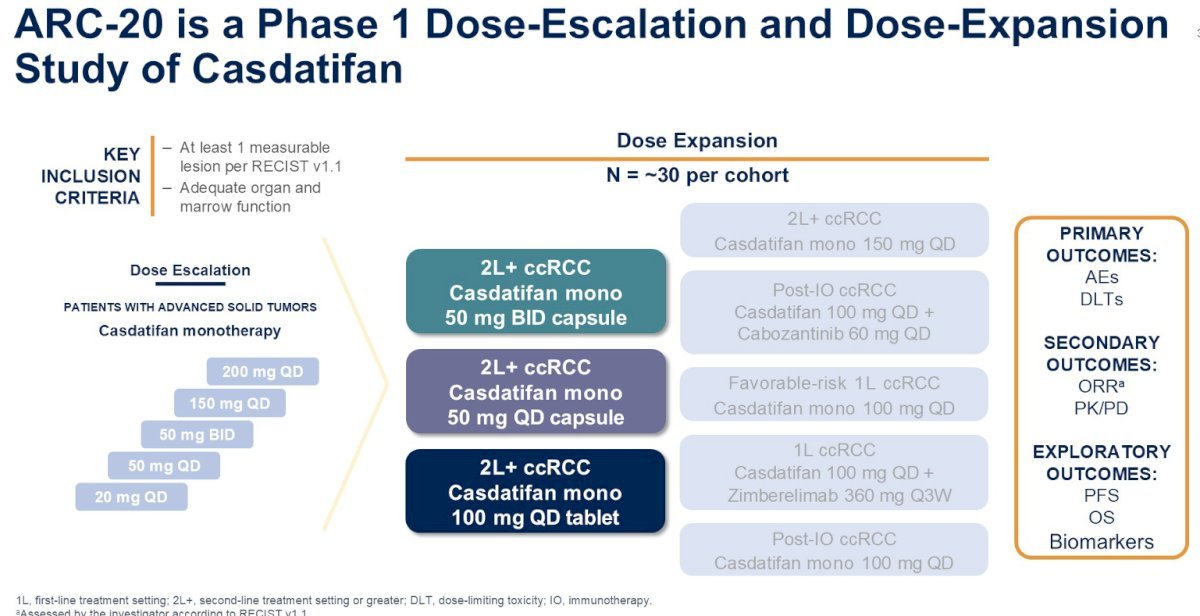
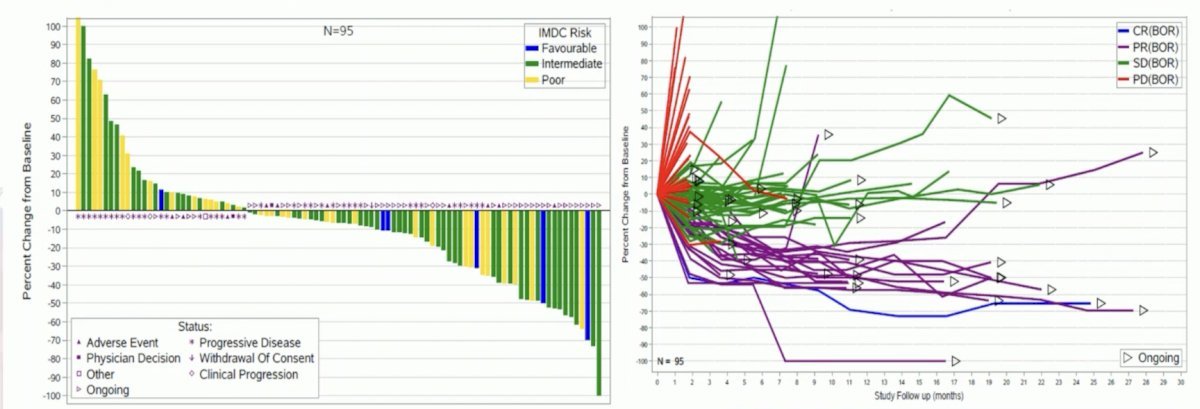
Beyond belzutifan, there are other HIF-2α inhibitors in development. Casdatifan is being evaluated in ARC-20 (NCT05536141), a phase I, open-label dose-escalation and dose-expansion study evaluating casdatifan monotherapy in patients (age ≥18) with clear cell RCC who are HIF-2α inhibitor naïve and previously treated with anti-PD-(L)1 and VEGFR-TKI therapies. In the phase I dose escalation portion, patients with advanced solid tumors containing an RCC component received various doses of casdatifan monotherapy at doses of 20 mg to 200 mg once daily. In the dose expansion cohort, casdatifan combination therapies will be tested.
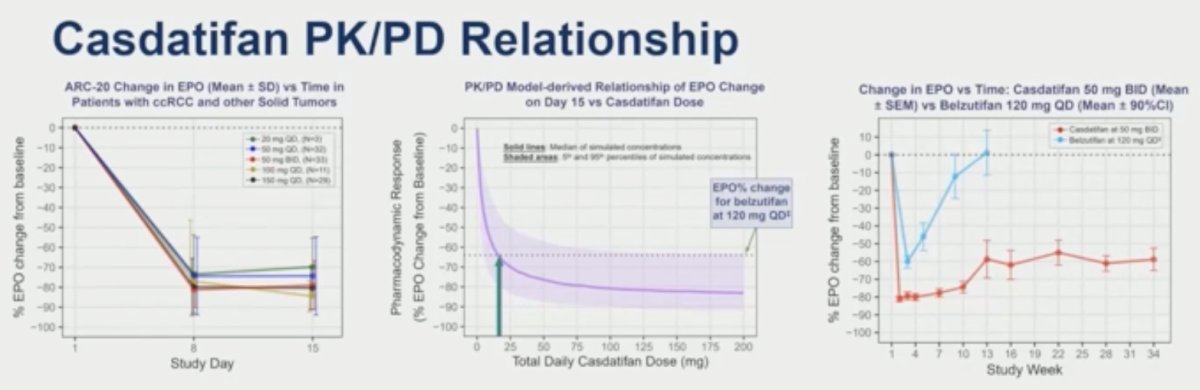
Casdatifan may hold key pharmacokinetic and pharmacodynamic advantages compared to other HIF-2α inhibitors:
- Casdatifan 20 mg daily provided a similar level of EPO suppression as belzutifan 120 mg daily
- Casdatifan dose of 100 mg had 5-fold higher exposure than 20 mg
- Casdatifan at 100 mg daily dose resulted in deeper and more sustained reduction in EPO
- Overall, the casdatifan dose of 100 mg was selected for further development
At a median follow-up of 5–15 months, the confirmed ORR was highest in the 100 mg once daily group (33%) versus 25% and 29% in the 50 mg twice daily and once daily groups, respectively. The 100 mg orally once daily dose was chosen as the recommended phase III dose.
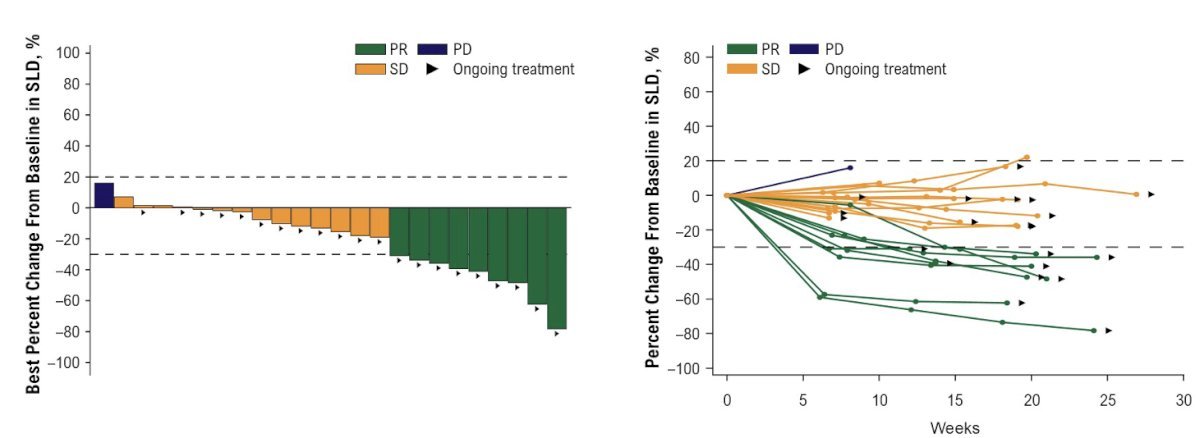
83% of patients had received ≥2 prior lines of therapy. The ORR was 33% in these patients (n=27), with 15% experiencing progressive disease.7
The results of the casdatifan + cabozantinib combination therapy from the ARC20 trial will be presented by Dr. Choueiri later in ASCO 2025. Of the 27 patients receiving this combination, 58% had received only prior IO therapy, and 42% had received prior IO + VEGF therapy. The ORR with this combination was 41%.
The planned phase III PEAK-1 trial will compare this combination, casdatifan + cabozantinib, to cabozantinib monotherapy in metastatic clear cell RCC patients who have received prior anti-PD-1/L- therapy.

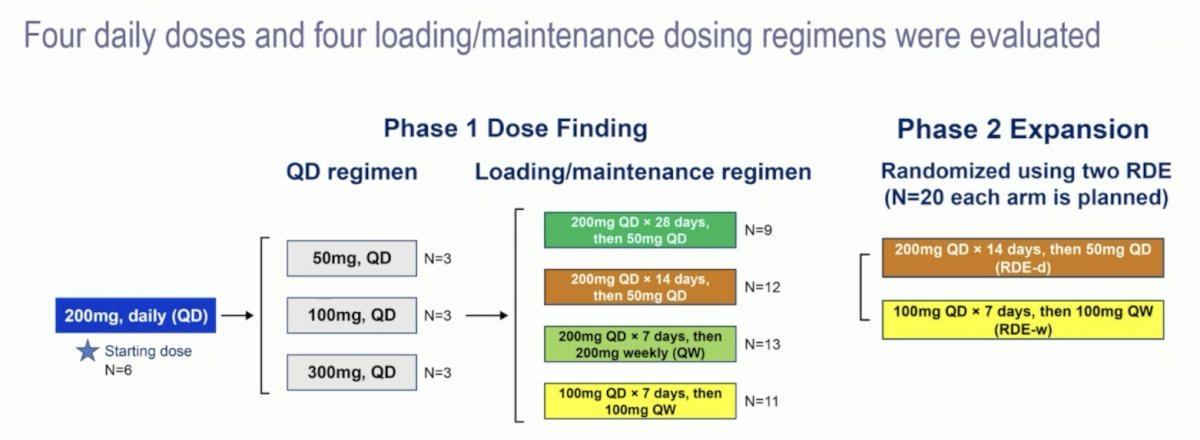
NKT2152 is another HIF-2α inhibitor being evaluated in the NKT2152-101 trial. This is an ongoing phase I/II trial (NCT05119335) that is investigating the safety, pharmacokinetics, pharmacodynamics, and clinical efficacy of NKT2152 in patients with advanced clear cell RCC. Adult patients with advanced clear cell RCC not amenable to standard therapy and progression after ≥1 prior regimen received NKT2152 in eight dose escalation cohorts: four daily and four loading/maintenance regimens, followed by a randomized expansion at two selected dose levels:
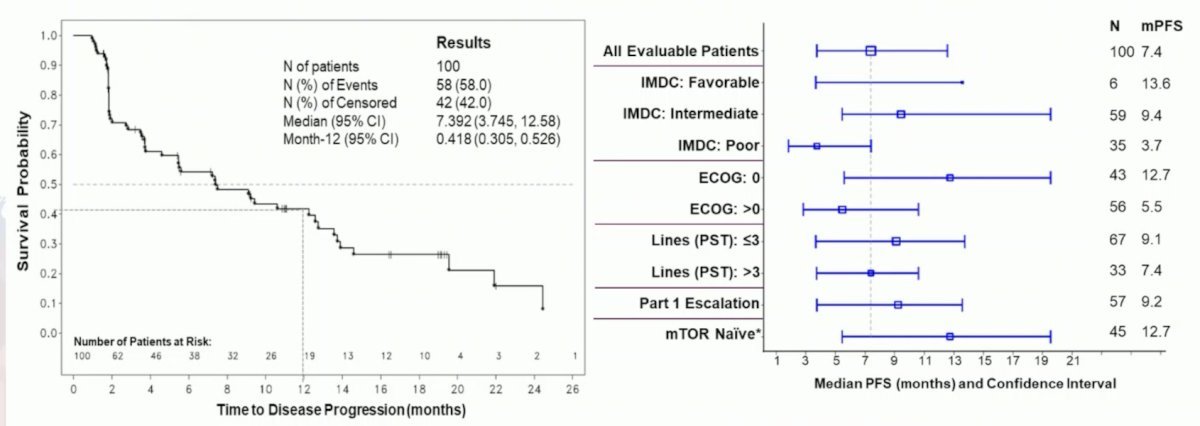
In 100 efficacy evaluable patients, the confirmed ORR was 20%.
The median PFS was 7.4 months, and the 12-month PFS rate was 42%.8
The pharmacologic and efficacy characteristics of HIF-2α inhibitors is summarized below:

Dr. McKay concluded her presentation on targeting HIF-2α as a new frontier in RCC therapy as follows:
- HIF-2α is a validated therapeutic target in RCC, and belzutifan is the 1st approved agent for the treatment of refractory RCC
- On pathway toxicity to HIF-2α inhibition includes anemia and hypoxia
- Belzutifan and casdatifan combinations are being explored in RCC

Presented by: Rana McKay, MD, Associate Professor, Department of Medicine, University of California, San Diego, CA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Barata P, Gulati S, Elliott A, Hammers HJ, Burgess E, Gartrell BA, et al. Renal cell carcinoma histologic subtypes exhibit distinct transcriptional profiles. J Clin Invest. 2024; 134(11):e178915.
- Rini BI, Powles T, Albiges L, et al. Final analysis of the phase III LITESPARK-005 study of belzutifan versus everolimus in participants with previously treated advanced clear cell renal cell carcinoma. Ann Oncol. 2024; 35(Suppl_2):LBA74.
- U.S. Food and Drug Administration. FDA approves belzutifan for advanced renal cell carcinoma. Silver Spring (MD): FDA; 2023 Dec 14. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-belzutifan-advanced-renal-cell-carcinoma.
- Ghatalia P, Agarwal N, Brugarolas J, et al. Safety and efficacy of two doses of belzutifan in patients with advanced renal cell carcinoma: results of the randomized phase II LITESPARK-013 study. Ann Oncol. 2023; 34(Suppl_2):Abstract 1881O.
- Choueiri TK, Merchan JR, Figlin R, McDermott DF, Arrowsmith E, Michaelson MD, et al. Belzutifan plus cabozantinib as first-line treatment for patients with advanced clear-cell renal cell carcinoma (LITESPARK-003): an open-label, single-arm, phase 2 study. Lancet Oncol. 2025; 26(1):64–73.
- Jonasch E, Donskov F, Iliopoulos O, Maughan BL, Wagner SJ, Gulati S, et al. Belzutifan for renal cell carcinoma in von Hippel–Lindau disease. N Engl J Med. 2021; 385(9):2036–46.
- Choueiri TK, Lee JL, Merchan J, et al. Casdatifan (Cas) monotherapy in patients with previously treated clear cell renal cell carcinoma (ccRCC): safety, efficacy and subgroup analysis across multiple doses from ARC-20, a phase 1 open-label study. J Clin Oncol. 2025; 43(5_suppl):441.
- Jonasch E, McGregor BA, Msaouel P, et al. NKT2152, a novel oral HIF-2α inhibitor, in participants with previously treated advanced clear cell renal cell carcinoma (accRCC): preliminary results of a Phase 1/2 study. Ann Oncol. 2024; 35(Suppl_2):Abstract 1690O.