(UroToday.com) The 2025 ASCO annual meeting featured a kidney cancer rapid oral abstract session and a presentation by Dr. James Geller discussing results of AREN1721, a randomized phase 2 trial of axitinib + nivolumab combination therapy versus single agent nivolumab for the treatment of TFE/translocation RCC across all age groups. Translocation RCC accounts for approximately 50% of pediatric RCC and 1-5% of RCC cases overall. Translocation RCC, driven by TFE3 or TFEb fusions or amplifications (TFEb), are often aggressive with no existing standard for systemic therapy.
AREN1721 was a prospective randomized COG-led NCTN phase 2 trial of nivolumab + axitinib combination therapy versus axitinib alone (closed early for feasibility) versus nivolumab alone in children and adults with advanced unresectable or metastatic translocation RCC. Prior exposure to anti-PD1/PDL1 therapies or axitinib was prohibited. The primary endpoint was progression-free survival, defined as the time from randomization to the earliest of disease progression based on immune-modified RECIST criteria or death. The final protocol version targeted enrollment of 28 eligible patients to detect a hazard ratio of 0.40 for the comparison of nivolumab + axitinib versus nivolumab alone using a one-sided log-rank test with alpha = 0.15.
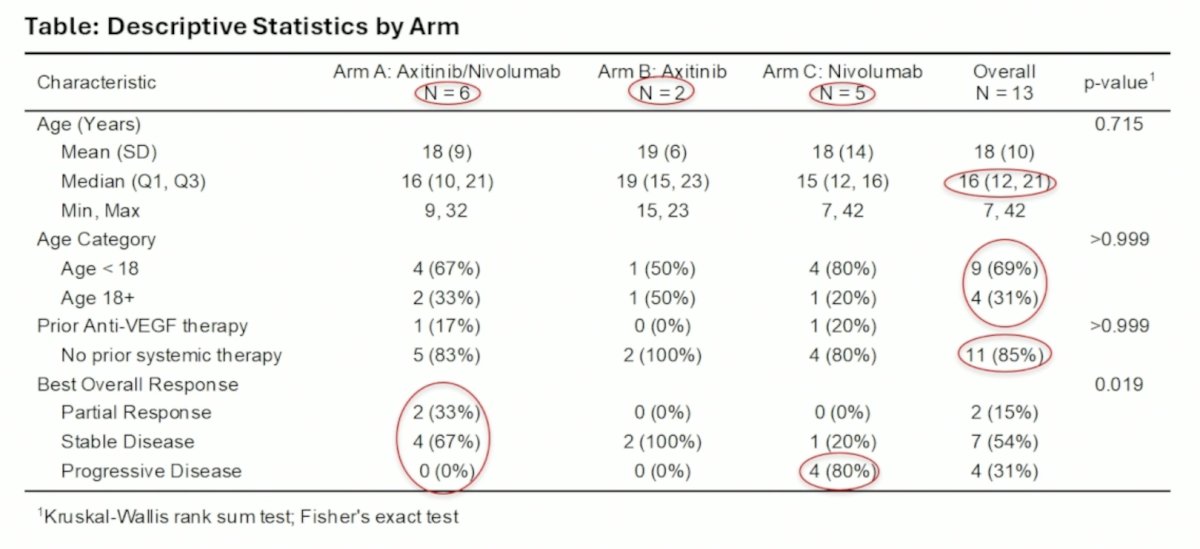
Despite aggressive approaches for trial recruitment, AREN1721 was closed after enrolling 15 patients (13 eligible) from 2019 to 2023 secondary to poor accrual. There were no unexpected toxicities. The median age was 16 years (range 7-42), with 9/13 age < 18 years, and 9/13 were male. Six patients were randomized to nivolumab + axitinib, two to axitinib alone, and five to nivolumab alone. Thirty-three percent of patients randomized to nivolumab + axitinib experienced partial response, compared to 0% in the other arms, and 0% of patients on the combination arm experienced primary disease progression:
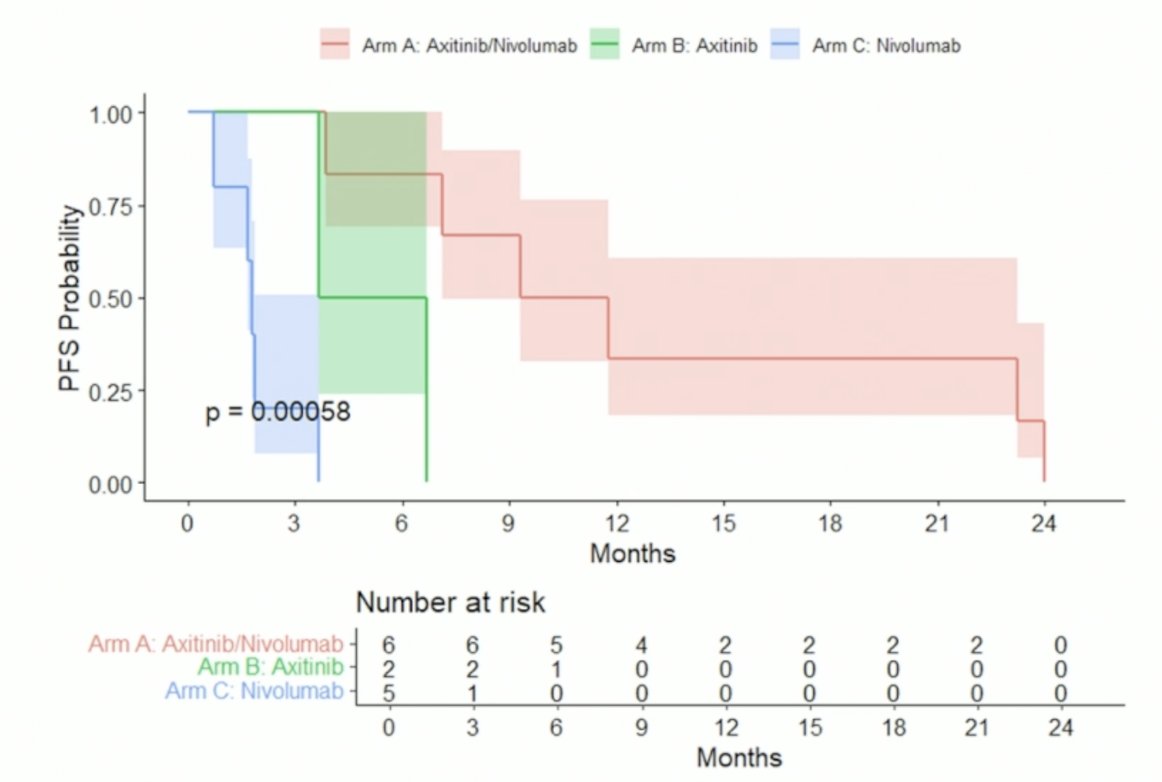
The addition of axitinib to nivolumab significantly improved progression-free survival (p = 0.0004), extending median progression-free survival from 1.8 to 10.5 months:
Overall survival also improved (p = 0.003) with the addition of axitinib:

Dr. Geller concluded his presentation discussing results of AREN1721, a randomized phase 2 trial of axitinib + nivolumab combination therapy versus single agent nivolumab for the treatment of TFE/translocation RCC across all age groups with the following take home points:
- Nivolumab + axitinib combination therapy was statistically more active than nivolumab single agent therapy, which itself was inactive
- Whether anti-PD1 pathway inhibitors add benefit to anti-VEGF therapy for translocation RCC remains to be determined
Presented by: James I. Geller, MD, Cincinnati Children's Hospital Medical Center, Cincinnati, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Pediatric-Inspired Trial Tests IO-TKI Combo for Translocation Renal Cell Carcinoma - James Geller