(UroToday.com)The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a kidney and bladder cancers poster session. Dr. Nataliya Mar presented the 3-year efficacy results of EV-103 Cohort H of neoadjuvant enfortumab vedotin (EV) monotherapy in cisplatin-ineligible patients with muscle invasive bladder cancer (MIBC).
MIBC patients who are ineligible for cisplatin therapy and are planned for a radical cystectomy have no neoadjuvant treatment options available with proven survival benefits.1 EV, an antibody-drug conjugate (ADC) directed against Nectin-4, is approved as monotherapy for patients with locally advanced/metastatic urothelial carcinoma (la/mUC) who have previously received a PD-1 or PD-L1 inhibitor and platinum-based chemotherapy, or who are ineligible for cisplatin-containing chemotherapy and have previously received ≥1 prior line of therapy.2 EV in combination with pembrolizumab is the standard of care in global treatment guidelines and is approved for use in patients with previously untreated la/mUC.3
EV-103 (NCT03288545) is a phase 1b/2, multicohort study assessing EV as monotherapy or in combination with other anticancer therapies, including pembrolizumab, in la/mUC and MIBC.4,5
In a previous report from Cohort H of EV-103, EV neoadjuvant monotherapy showed encouraging activity in cisplatin-ineligible MIBC patients:6
- Among 22 patients who received EV neoadjuvant treatment, 8 patients (36%) achieved a pathologic complete response (pCR) and 11 patients (50%) achieved pathologic downstaging
- The 2-year event-free survival (EFS) rate was 62%
Herein, Dr. Mar presented the updated 3-year efficacy results, including event-free survival (EFS), overall survival (OS), subsequent cancer-related therapy, safety, and tolerability, from Cohort H of the EV-103 study.
The key baseline characteristics are shown in the table below:

Of the 22 patients, 19 (86%) completed all 3 cycles of neoadjuvant EV, and the median duration of treatment was 2.1 months. All enrolled patients underwent surgery within the protocol window (within 4–12 weeks of the last EV dose) without any delays. The median follow-up was 49.7 months.
The most common reason for cisplatin ineligibility was a creatinine clearance of ≥30 to <60 mL/min (55%), followed by grade ≥2 hearing loss (45.5%).

The median EFS by investigator assessment was 40.1 months. The estimated EFS rates at 24 and 36 months were 62% and 57%, respectively. The median EFS has not been reached for patients with pCR and was 19 months for patients without pCR.

While the median OS was not reached, the 24- and 36-month OS rates were 77% and 68%, respectively.

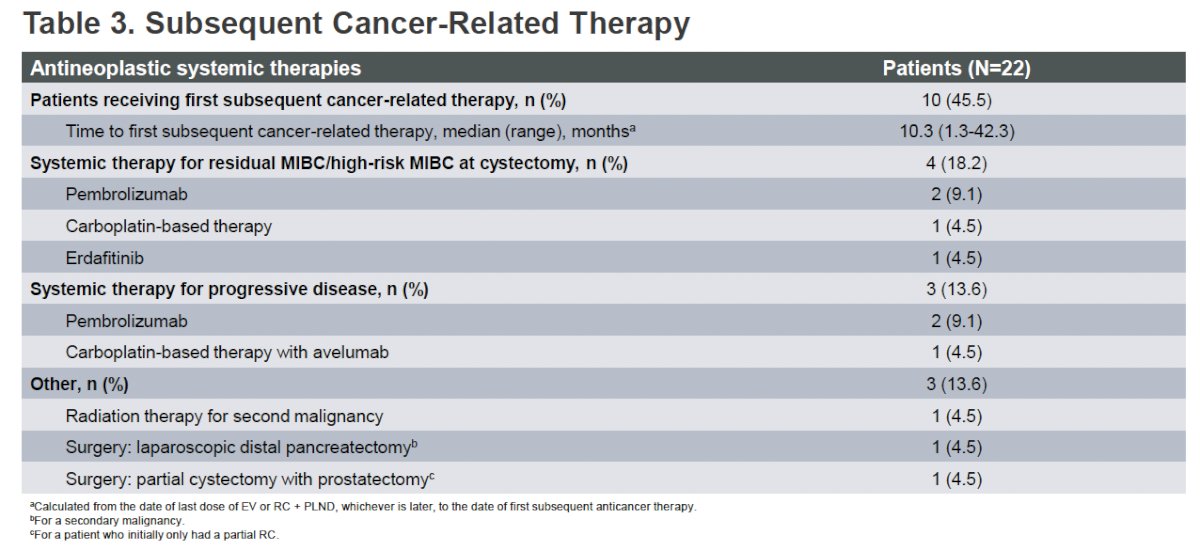
Subsequent cancer-related therapies following study treatment discontinuation are shown in the table below. 45.5% of patients received a first subsequent cancer-related therapy, at a median time of 10.3 months. 4/22 patients (18%) received systemic therapy for residual MIBC or high-risk MIBC at cystectomy, most commonly pembrolizumab (9%). Three patients (14%) received systemic therapy for progressive disease.
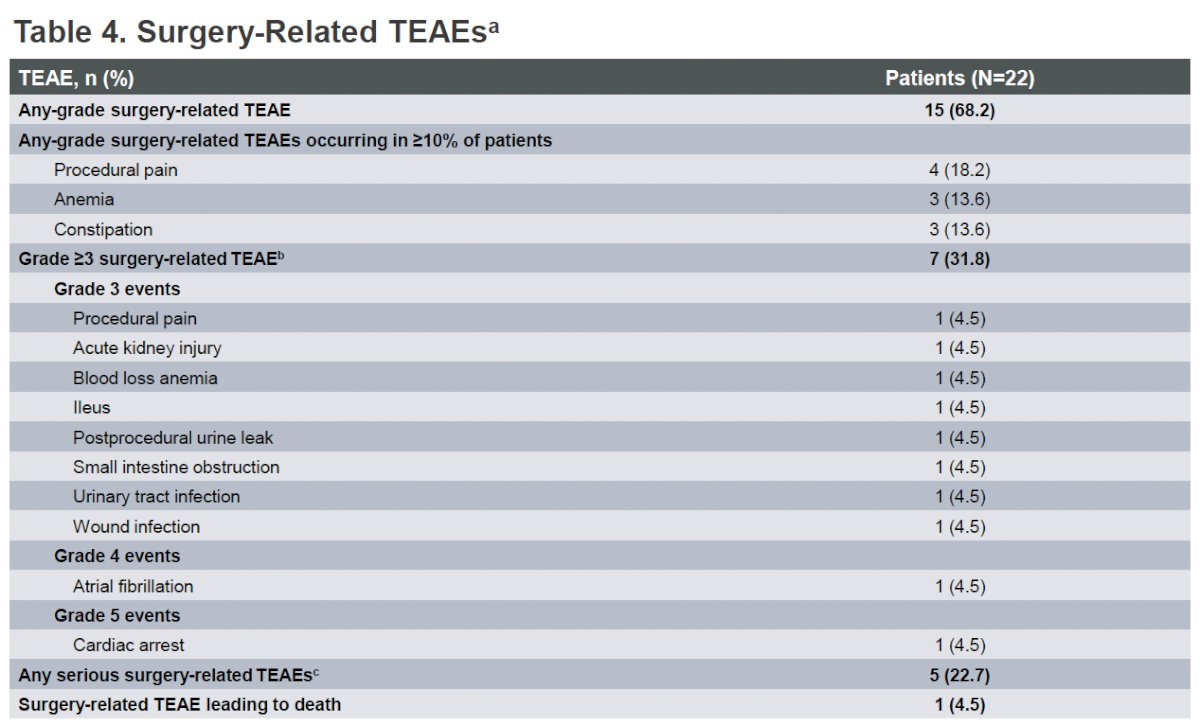
Any-grade surgery-related treatment-emergent adverse event (TEAE) was observed in 68% of patients. Grade ≥3 TEAEs were observed in 32%. Any serious surgery-related TEAE was observed in 5/22 (22.7%) patients.
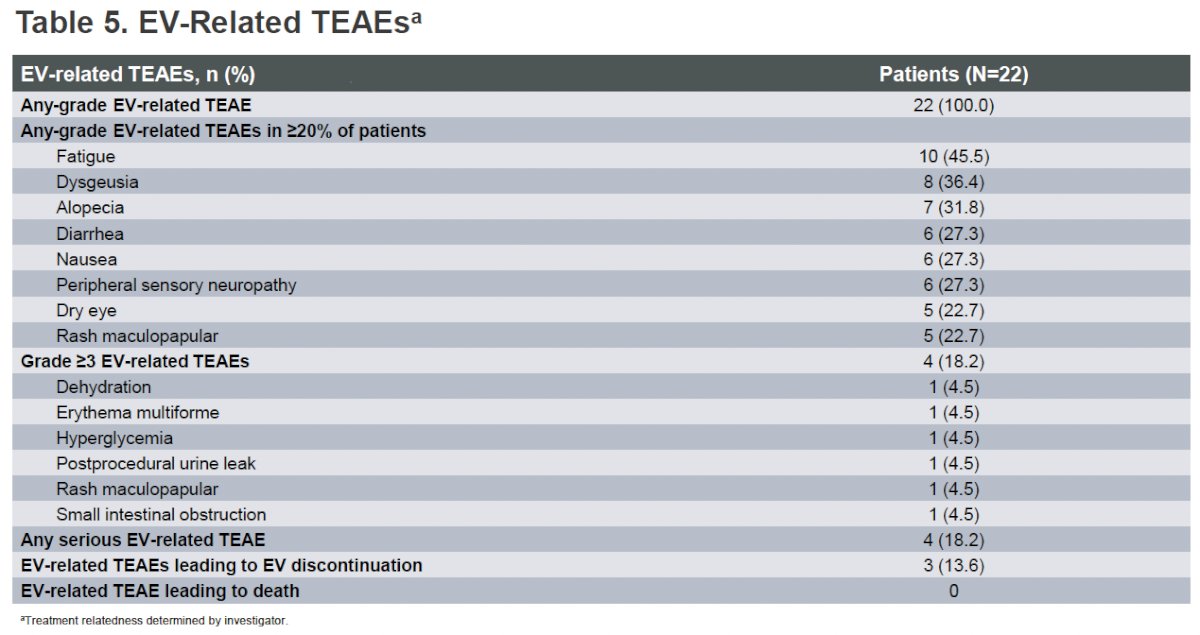
Any-grade EV-related TEAE was observed in all 22 patients, most commonly fatigue (46%), dysgeusia (36%), and alopecia (32%). Grade ≥3 EV-related TEAEs were observed in 4/22 patients (18%).
Adverse events of special interest are summarized below:

Dr. Mar concluded as follows:
- Based on 3-year efficacy results, neoadjuvant EV monotherapy treatment continued to show encouraging antitumor activity in cisplatin-ineligible MIBC patients, with median EFS and OS exceeding historical real-world data in cisplatin-ineligible patients following RC alone7,8
- The safety profile was generally manageable and consistent with the known AE profile of EV in other settings
- These prospective data provide valuable insights in an otherwise understudied patient population
- Phase III trials evaluating perioperative EV plus pembrolizumab in patients with MIBC who are cisplatin ineligible and eligible (KN-905/EV-303, KN-B15/EV-304) are ongoing9,10
Presented by: Nataliya Mar, MD, Medical Oncologist, Associate Professor, Department of Medicine, University of California Irvine, Irvine, CA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Flaig TW, Agarwal N, Grivas P, et al. Enfortumab vedotin plus pembrolizumab in advanced urothelial carcinoma: updated efficacy and safety. Poster presented at: American Society of Clinical Oncology (ASCO) Annual Meeting; 2023 Jun 2–6; Chicago, IL. Poster 4595.
- Pfizer Inc. PADCEV (enfortumab vedotin-ejfv). New York, NY: Pfizer; 2025. Accessed 2025 June 2.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. N Engl J Med. 2023;389(22):2031–44.
- Hoimes CJ, Tagawa ST, Agarwal N, et al. A randomized phase II study of immune checkpoint inhibition with or without chemotherapy in metastatic urothelial cancer. J Clin Oncol. 2023;41(1):22–31.
- National Cancer Institute (NCI). A study of enfortumab vedotin alone or with other therapies for treatment of urothelial cancer (EV-103) [clinical trial identifier NCT03288545]. ClinicalTrials.gov.
- O’Donnell P, Petrylak DP, Grivas P, et al. Clinical outcomes with enfortumab vedotin in previously treated urothelial carcinoma: updated analysis. Poster presented at: American Society of Clinical Oncology (ASCO) Annual Meeting; 2024 May 31–Jun 4; Chicago, IL. Poster 4564.
- Li R, Sridhar SS, Necchi A, et al. Novel perioperative strategies in muscle-invasive bladder cancer: advances in immunotherapy and antibody–drug conjugates. Eur Urol Oncol. 2024;7(3):614–24.
- Rose R, Gayed B, Josephson DY, et al. Cisplatin-ineligible muscle-invasive bladder cancer demonstrates poor long-term outcomes following immediate radical cystectomy and presents opportunity for neoadjuvant pembrolizumab. Presented at: Southeastern Section of the American Urological Association (SESAUA) 2023 Annual Meeting; 2023 Mar 15–19; Miami, FL.
- National Cancer Institute (NCI). Perioperative enfortumab vedotin (EV) plus pembrolizumab (MK-3475) versus neoadjuvant chemotherapy for cisplatin-eligible muscle invasive bladder cancer (MIBC) (MK-3475-B15/KEYNOTE-B15/EV-304) [clinical trial identifier NCT04700124]. ClinicalTrials.gov. https://clinicaltrials.gov/study/NCT04700124. Accessed 2025 May 13.
- National Cancer Institute (NCI). Perioperative pembrolizumab (MK-3475) plus cystectomy or perioperative pembrolizumab plus enfortumab vedotin plus cystectomy versus cystectomy alone in participants who are cisplatin-ineligible or decline cisplatin with muscle-invasive bladder cancer (MK-3475-905/KEYNOTE-905/EV-303) [clinical trial identifier NCT03924895]. ClinicalTrials.gov. https://clinicaltrials.gov/study/NCT03924895. Accessed 2025 May 13.