(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to a kidney and bladder cancers poster session. Dr. Guillermo de Velasco presented SOGUG-NEOWIN, an ongoing phase II, open-label, multicenter, multinational interventional trial evaluating the efficacy and safety of erdafitinib monotherapy and the combination of erdafitinib plus cetrelimab as neoadjuvant treatment in cisplatin-ineligible patients with muscle-invasive bladder cancer harboring FGFR gene alterations.
Dr. De Velasco noted that the standard of care treatment for localized MIBC remains neoadjuvant cisplatin combination chemotherapy followed by radical cystectomy (RC). However, many patients are cisplatin ineligible. Immune checkpoint inhibitors (ICIs) have altered the treatment landscape of metastatic urothelial cancer (mUC), including for those who are cisplatin-ineligible. Based on these results, ICIs are being explored as neoadjuvant treatment in resectable UC, with preliminary data suggesting anti-tumor activity.
Erdafitinib is a Fibroblast Growth Factor Receptor (FGFR) inhibitor, which has shown efficacy in mUC with select FGFR2/3 mutations/fusions.1 Erdafitinib plus cetrelimab demonstrated clinically meaningful activity in patients with newly diagnosed FGFR-altered mUC in the phase II NORSE trial.2 This study will assess whether erdafitinib plus cetrelimab will improve the pathological complete response (pCR) rate in patients with FGFR-mutated MIBC who are candidates for RC and are ineligible for or refuse neoadjuvant cisplatin-based therapy.
The study design is summarized below. Patients with FGFR-mutated cT2-4aN0-1M0 urothelial carcinoma planned for RC, who are ineligible for or refuse neoadjuvant cisplatin-based chemotherapy, will be assigned to one of two cohorts:
- Erdafitinib daily for 9-12 weeks (n=45)
- Erdafitinib daily + cetrelimab for 9-12 weeks (n=45)
Following completion of therapy, patients would be planned for a radical cystectomy within 2-6 weeks and followed for 36 months.
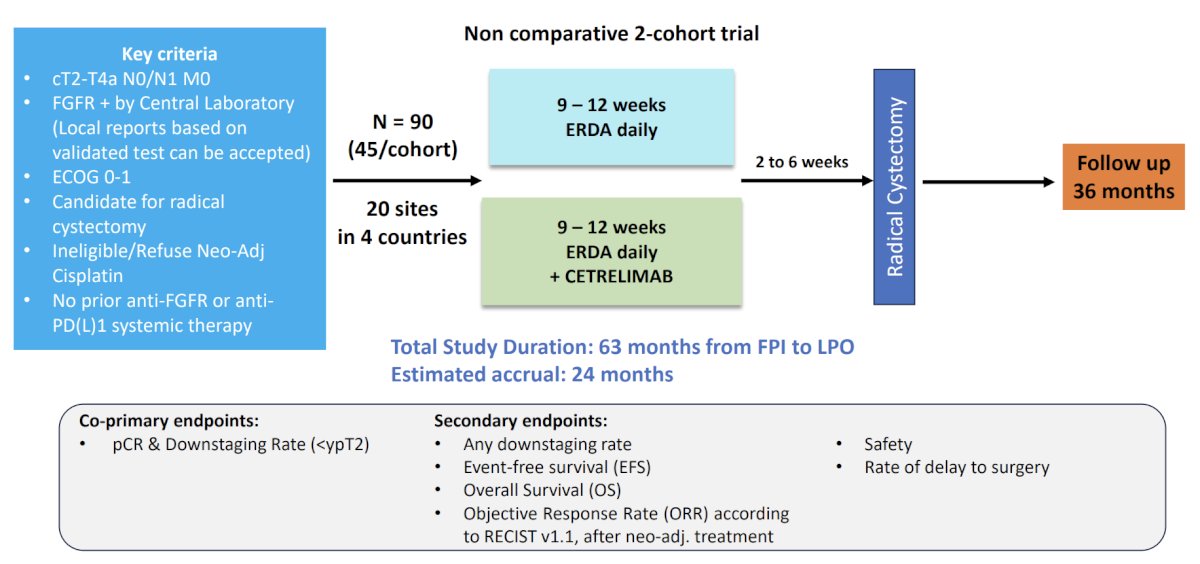
The co-primary endpoints are pCR and pathologic downstaging (i.e., <ypT2). Key secondary endpoints are:
- Any downstaging rate
- Event-free survival
- Overall survival
- Objective response rate
- Safety
- Rate of delay to surgery
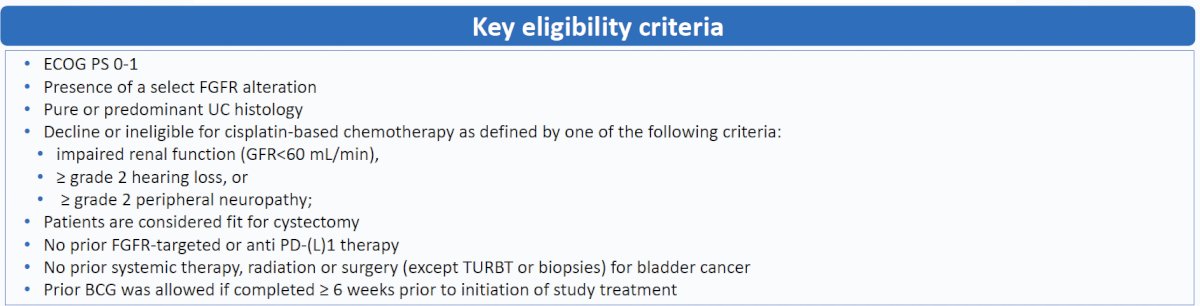
The key eligibility criteria are summarized below:
The trial is approved in four countries (France, Italy, Spain, and the UK). The first patient was pre-screened on January 31, 2024. As of March 31, 2025, 91 patients were pre-screened, 9 were FGFR2/3 positive, and 5 were enrolled.
Presented by: Guillermo de Velasco, MD, PhD, Medical Oncologist, Hospital 12 de Octubre, Madrid, Spain
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Loriot Y, Necchi A, Park SH, et al. Erdafitinib in Locally Advanced or Metastatic Urothelial Carcinoma. N Engl J Med 2019 Jul 25;381(4):338-348.
- Ravi P, Morris MJ, McGregor BA, et al. Lutetium-177–PSMA-617 plus enzalutamide versus enzalutamide alone in metastatic castration-resistant prostate cancer: Results from the randomized Phase 2 NORSE trial. Presented at: 2024 ASCO Genitourinary Cancers Symposium (ASCO GU); January 25–27, 2024; San Francisco, CA. Abstract 139.