(UroToday.com) The 2025 ASCO annual meeting featured a urothelial carcinoma oral abstract session and a presentation by Dr. Dickon Hayne discussing ANZUP 1301, a randomized phase 3 trial of mitomycin + BCG as adjuvant intravesical therapy for high-risk non muscle invasive bladder cancer.
Intravesical BCG is the standard of care for high-risk non-muscle invasive bladder after maximal transurethral resection, which is given as induction followed by maintenance (at least 1 year) intravesical therapy. However, the availability and access to BCG have been a global challenge since 2013. As such, Dr. Hayne and colleagues sought to determine the efficacy and safety of intravesical treatment with BCG + mitomycin compared with BCG alone for high-risk BCG-naïve non muscle invasive bladder cancer.
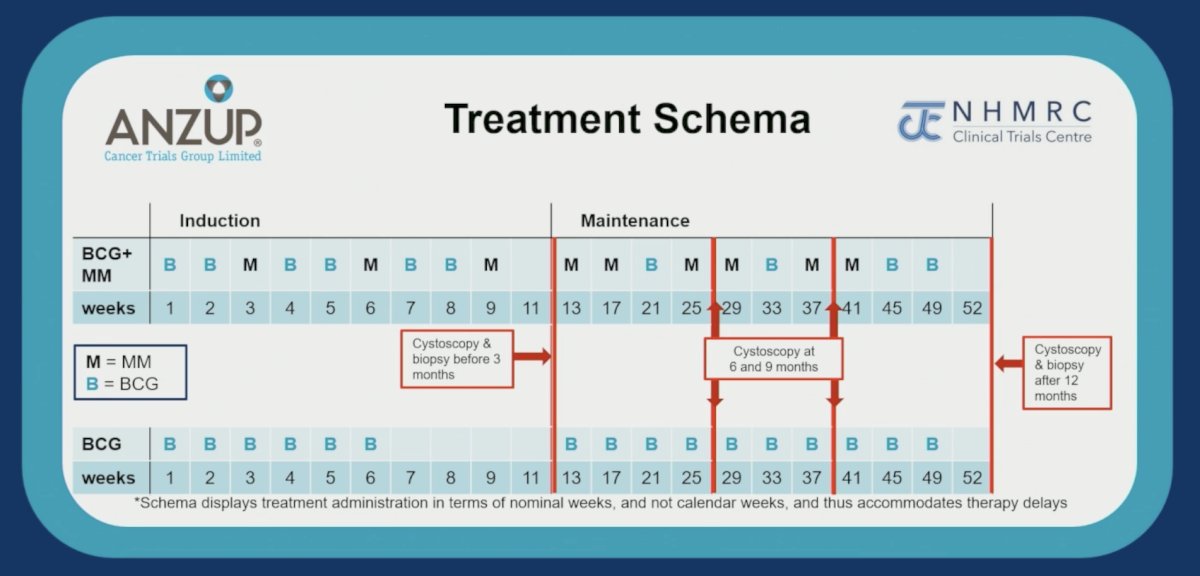
ANZUP 1301 was an open-label, randomized, phase 3 trial. Eligible participants had high-grade papillary urothelial cancer stages pTa/pT1, with concurrent CIS being allowed. Participants were randomly assigned to BCG + mitomycin versus BCG alone. The BCG + mitomycin regimen was weekly induction x 9 (BCG weeks 1, 2, 4, 5, 7, and 8; mitomycin weeks 3, 6, and 9) followed by 4-weekly maintenance x 9 (mitomycin weeks 13, 17, 25, 29, 37, and 41; BCG weeks 21, 33, and 45: total of 9 BCG doses). The BCG alone regimen was weekly induction x 6, then 4-weekly maintenance x 10: total of 16 BCG doses. The trial design and treatment schedule is as follows: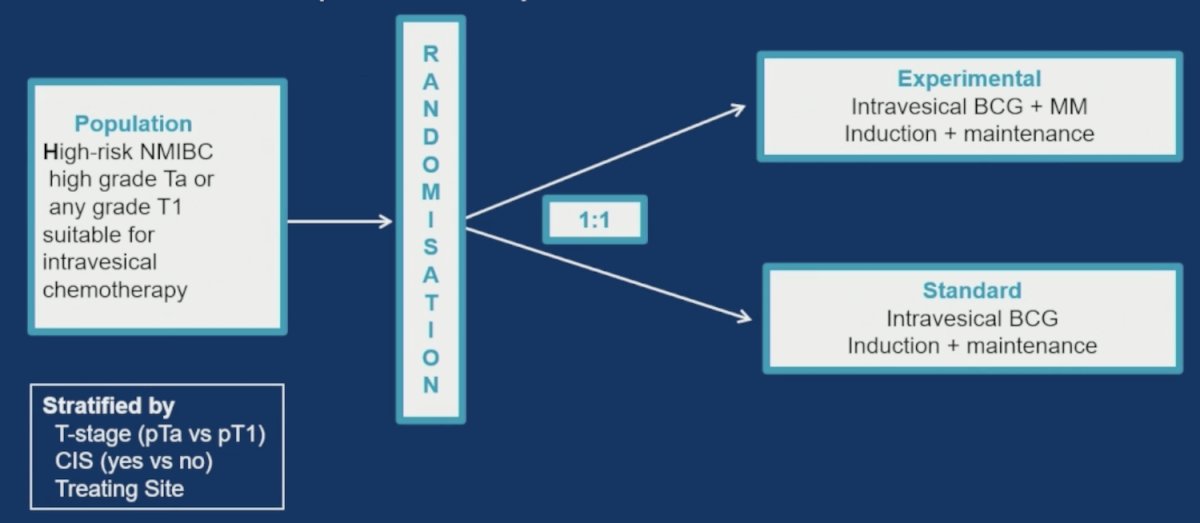
The primary endpoint was disease free survival at 2 years, and secondary outcomes included complete response on cystoscopy at 3 months, time-to-recurrence, time-to-progression, overall survival, and safety. The target sample size of 500 provided 85% power to detect an absolute improvement of 10% in disease free survival at 2 years with a type-1 error rate of 0.05.
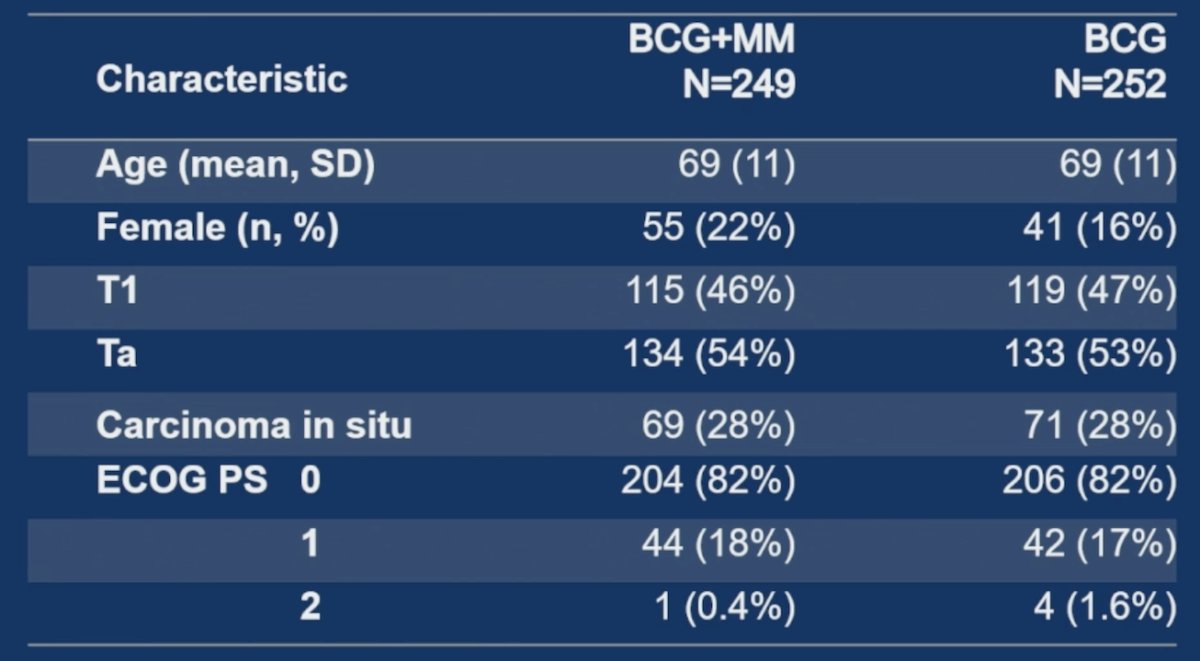
This trial enrolled 501 participants from December 2013 to May 2023: the mean age 69 years (SD 63-77), 53% had pTa disease, 47% had pT1 disease, and 28% had concurrent CIS:
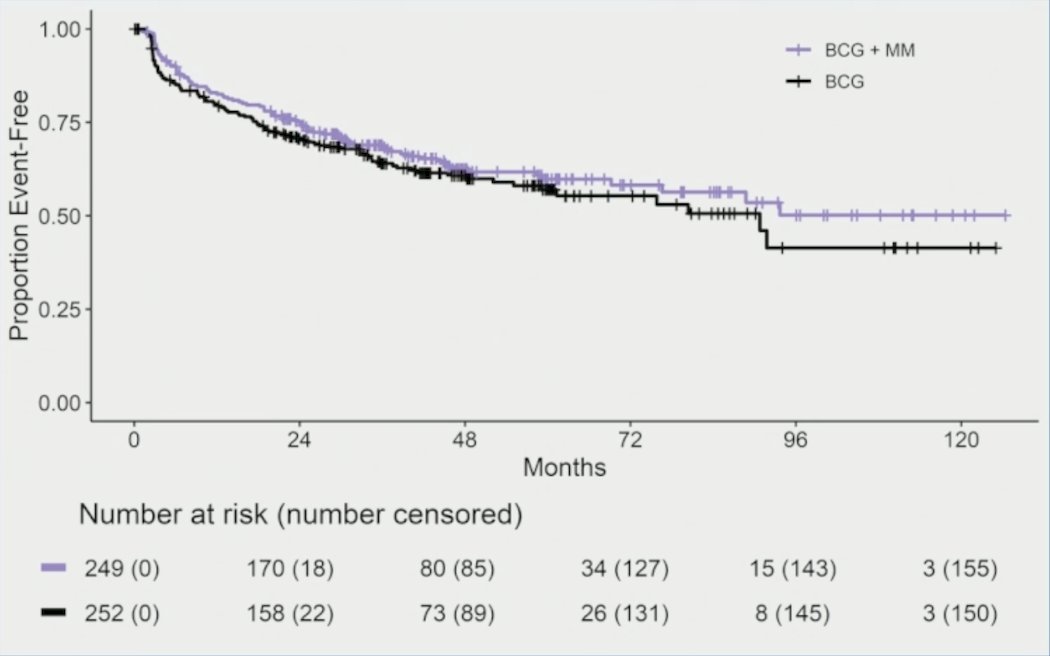
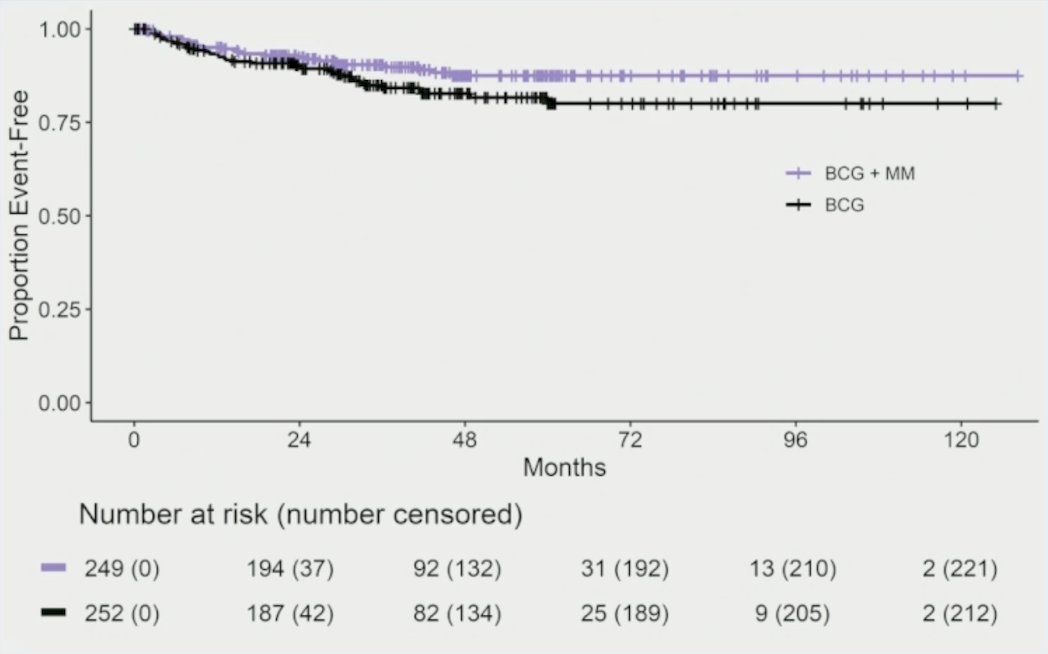
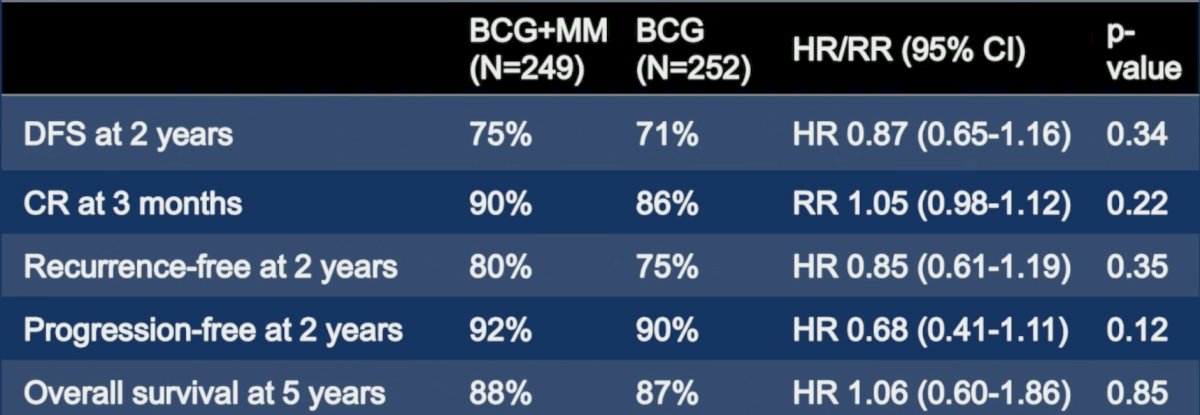
In this primary analysis, the median follow-up was 48 months (IQR 34-64) at the data cut-off of December 6, 2024. The disease free survival rate at 24 months in the BCG + mitomycin arm was 75% versus 71% for BCG alone (HR 0.87, 95% CI 0.65-1.16):
With regards to secondary endpoints, the complete response on cystoscopy at 3 month rate was 90% for BCG + mitomycin compared to 86% for BCG alone. The time to recurrence rate at 24 months was 80% for BCG + mitomycin compared to 75% for BCG alone (subdistribution HR 0.85, 95% CI 0.61-1.19):

Moreover, time to progression at 24 months was 92% for BCG + mitomycin versus 90% for BCG alone (subdistribution HR 0.68, 95% CI 0.41-1.11)
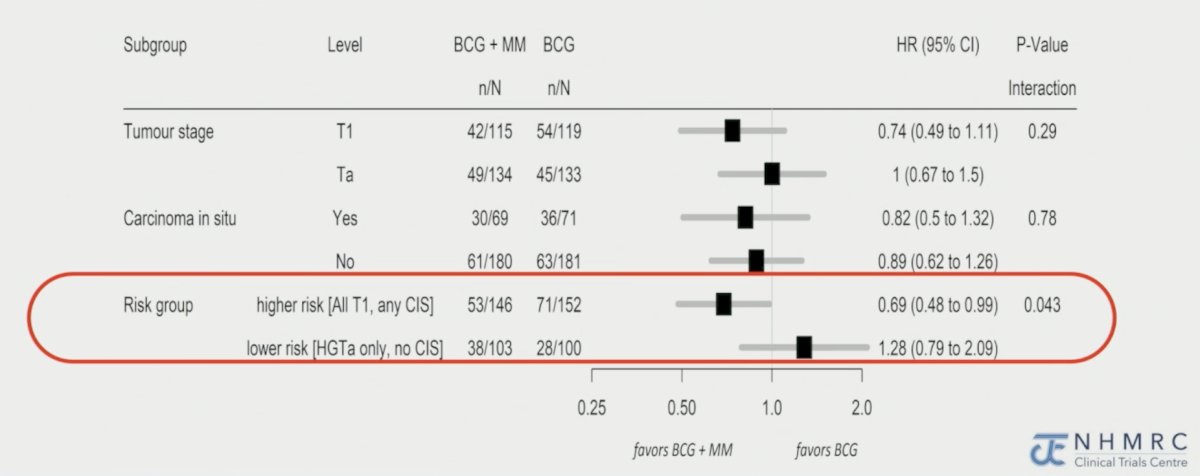
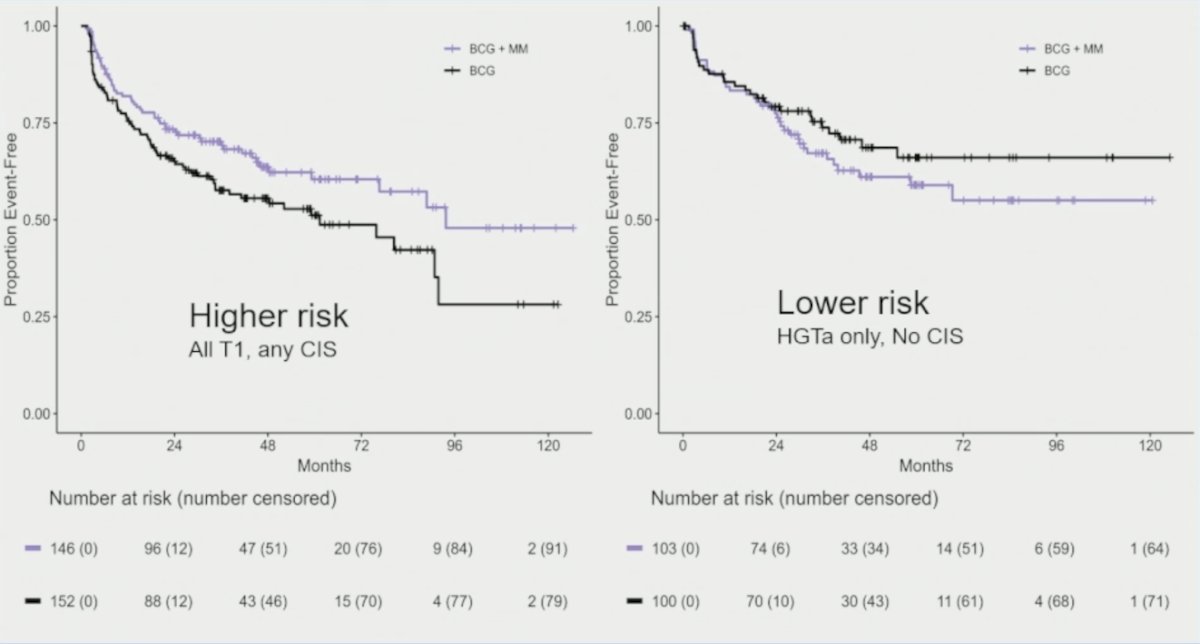
There was no difference in overall survival, with 26 deaths in the BCG + mitomycin arm (7 from bladder cancer) versus 23 in the BCG alone arm (5 from bladder cancer). Subgroup analyses for disease free survival suggest a potential role for BCG + mitomycin in patients with higher risk (all T1, any CIS) disease (HR 0.69, 95% CI 0.48-0.99):
A summary of all efficacy endpoints is as follows:
The numbers of participants with grade 3-5 adverse events were 43 in BCG + mitomycin versus 37 in BCG alone. The adverse event (of any grade) reported by the highest numbers of participants (BCG + mitomycin versus BCG alone) were fatigue (109 versus 110), renal/urinary (78 versus 83), and flu-like symptoms (34 versus 60):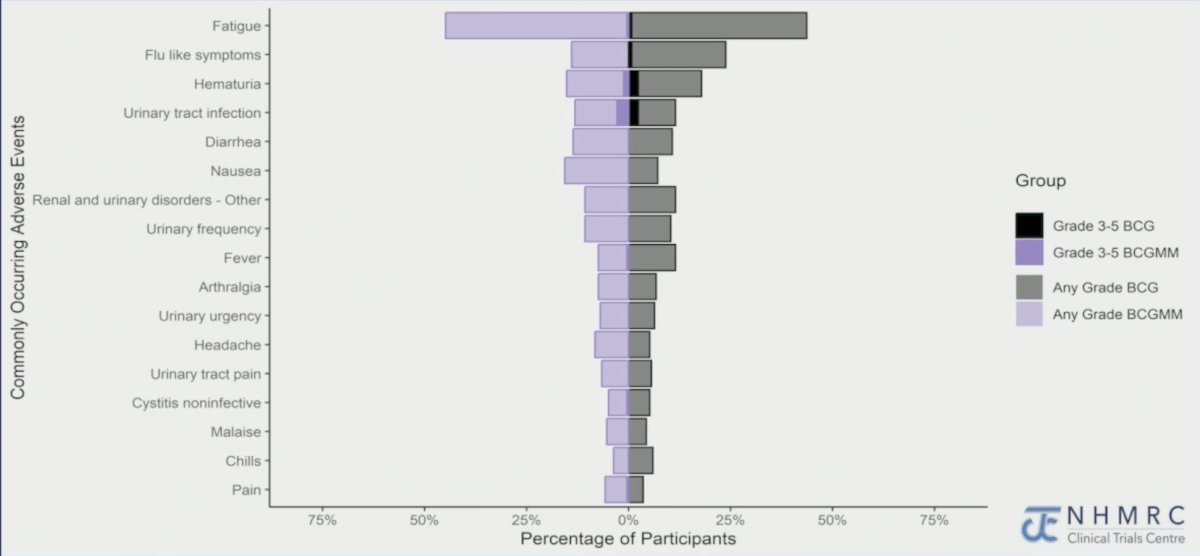
More participants had ≥75% of their planned doses with BCG + mitomycin than BCG alone (78% versus 68%; p = 0.02). The total numbers of instillations were higher for BCG + mitomycin than BCG alone (4,033 versus 3,383), whereas the total doses of BCG (2,056 versus 3,383), and median doses of BCG per patient (9 versus 16) were lower for BCG + mitomycin than BCG alone:

Dr. Hayne concluded his presentation discussing ANZUP 1301 with the following take-home points:
- BCG + mitomycin had similar efficacy and safety, but with fewer treatment discontinuations and fewer (40%) doses of BCG than BCG alone
- Higher-risk patients may do better with BCG + mitomycin
- BCG + mitomycin is a good alternative to BCG alone
- Wide adoption of the BCG + mitomycin regimen could alleviate the global BCG shortage
Presented by: Dickon Hayne, MD, FRCS, UWA Medical School, University of Western Australia, Perth, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.