(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the session Advancing Perioperative Treatment Options for Localized Muscle-Invasive Bladder Cancer: A Step Forward. Dr. Jonathan E. Rosenberg delved into how to move forward risk-Adaptive Neoadjuvant Chemotherapy and Adjuvant Immunotherapy for NMIBC.
Dr. Rosenberg opened his presentation by emphasizing that while perioperative therapy improves survival in patients with muscle-invasive bladder cancer (MIBC), the question of which patients benefit from which therapy or whether some need both remains unresolved. He reiterated that preoperative neoadjuvant cisplatin-based chemotherapy enhances event-free and overall survival. Although adjuvant chemotherapy alone has not shown an overall survival (OS) benefit in individual trials, meta-analyses support its use.1
The NIAGARA trial demonstrated that adding durvalumab to gemcitabine/cisplatin followed by adjuvant durvalumab significantly improves both event-free survival (EFS) and OS.2 Additionally, adjuvant immunotherapy with nivolumab or pembrolizumab improves DFS, with nivolumab showing a strong trend toward OS benefit. Dr. Rosenberg underscored the importance of risk stratification, noting that many patients are already cured with chemotherapy and surgery alone, and better selection could help avoid both overtreatment and undertreatment.3-5
Dr. Rosenberg structured his presentation around three key areas: i.) pathologic staging, ii.) circulating tumor DNA (ctDNA), iii.) PD-L1 status. He noted that historically, risk stratification for postoperative therapy in bladder cancer has been based largely on clinical intuition, with pathological findings following radical surgery serving as the primary guide. Adjuvant therapy has typically been considered for high-risk patients, defined as those with ≥pT2 or node-positive (N+) disease after neoadjuvant chemotherapy, or ≥pT3 or N+ disease in the absence of prior NAC. However, he emphasized a key limitation of this approach: low-risk patients may still relapse, while some high-risk patients do not, underscoring the need for more precise biomarkers to better inform treatment decisions.
Historically, pathologic stage has been a key determinant of long-term outcomes in bladder cancer, particularly following neoadjuvant chemotherapy. This was demonstrated in Dr. Grossman’s landmark 2003 trial published in the New England Journal of Medicine, which showed that patients treated with MVAC prior to radical cystectomy achieved a pathologic complete response (pCR; pT0N0) rate of 38% compared to 15% in those undergoing surgery alone. Notably, patients with pT0N0 disease had a 5-year OS rate of 85%, in stark contrast to 50% in those without complete response. These findings underscore that achieving a complete pathologic response is strongly associated with improved EFS and OS.6
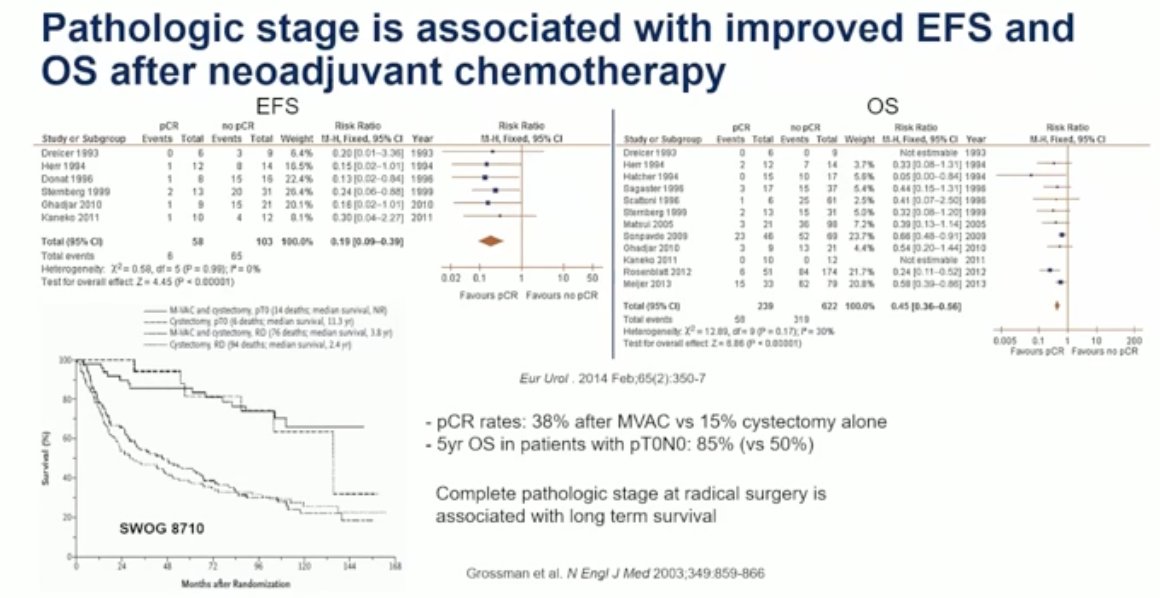
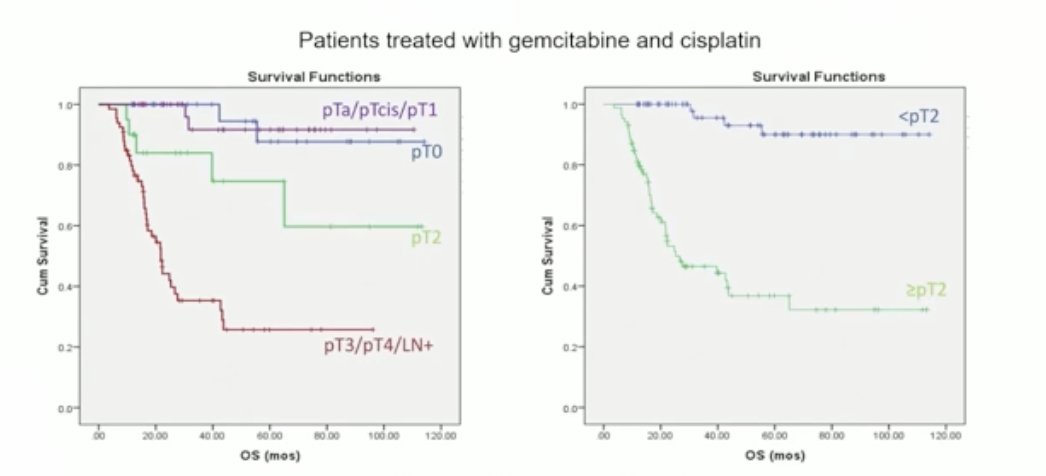
Dr. Rosenberg noted that while pCR has not been formally validated as a surrogate biomarker, it appears to correlate strongly with favorable outcomes in this setting. This raises a key clinical question: what pathologic stage should serve as the threshold for considering adjuvant therapy following neoadjuvant chemotherapy? Retrospective data from MSKCC suggest that patients with MIBC (≥pT2) treated with gemcitabine and cisplatin-based NAC derive significant benefit, supporting the use of post-NAC pathologic staging to guide adjuvant treatment decisions.
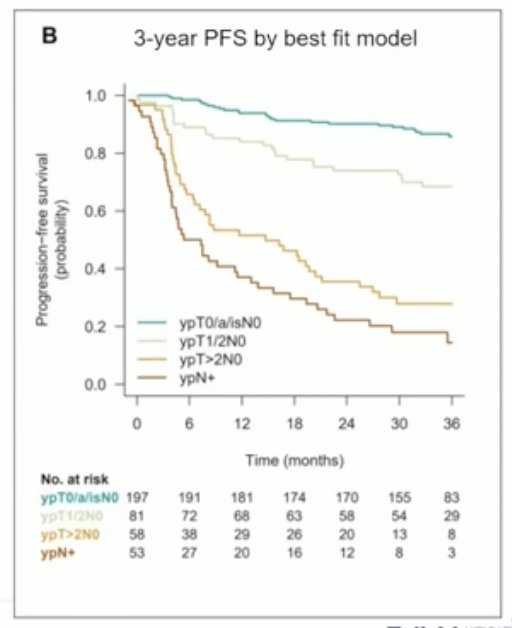
However, this relationship is not consistent across all trials. In the VESPER trial, outcomes for patients with ypT1 and ypT2 disease were similar. Within the neoadjuvant subset comparing ddMVAC to GC, patients with non-invasive disease (pT0/Tis/Ta) had comparable outcomes, while those with post-chemotherapy pT1N0 and pT2N0 tumors demonstrated similar survival patterns. Notably, patients with post-chemotherapy pT2 disease fared better than expected when compared to historical series. This raises an important clinical question: should patients with pT1 disease receive adjuvant therapy? Based on current evidence from a single trial, the answer remains unclear.1
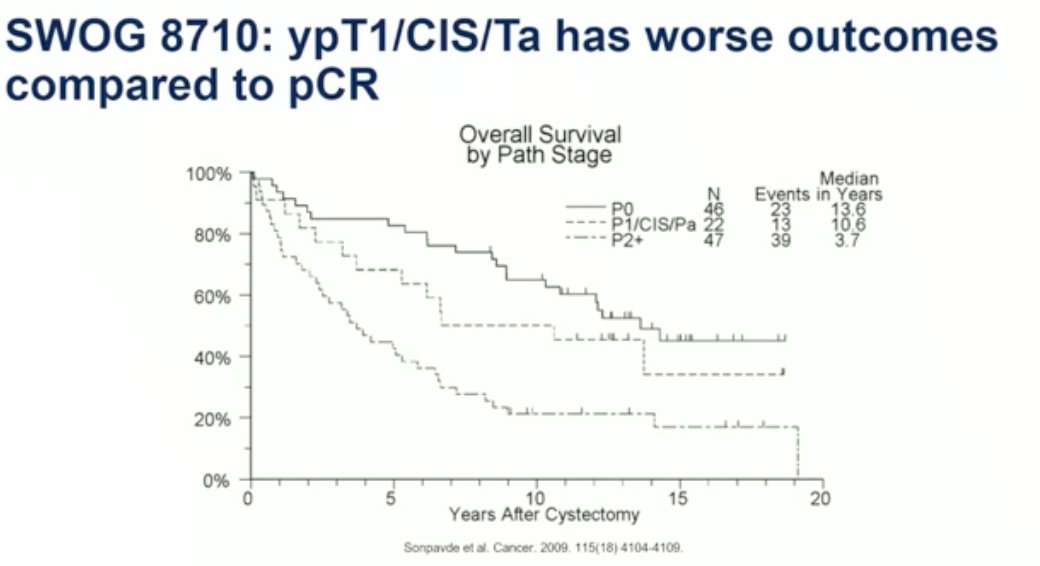
Moreover, in SWOG 8710, patients with ypT1/CIS/Ta disease in the chemotherapy arm had worse outcomes compared to those who achieved a pCR, as illustrated in the figure below.6
We have heard many times that it does not matter how you get to pCR it shows a survival advantage. Dr Rosenberg discussed data from the Nordic Cystectomy Trials 1 and 2 that suggest a pathologic complete response was associated with improved overall survival only in patients who received chemotherapy. The 5-year OS was 88.2% in chemotherapy-treated patients with pCR, compared to 57% in patients who achieved a pCR without prior chemotherapy (p=0.001). These findings highlight that pathologic stage alone does not fully capture the surrogate potential of pCR.
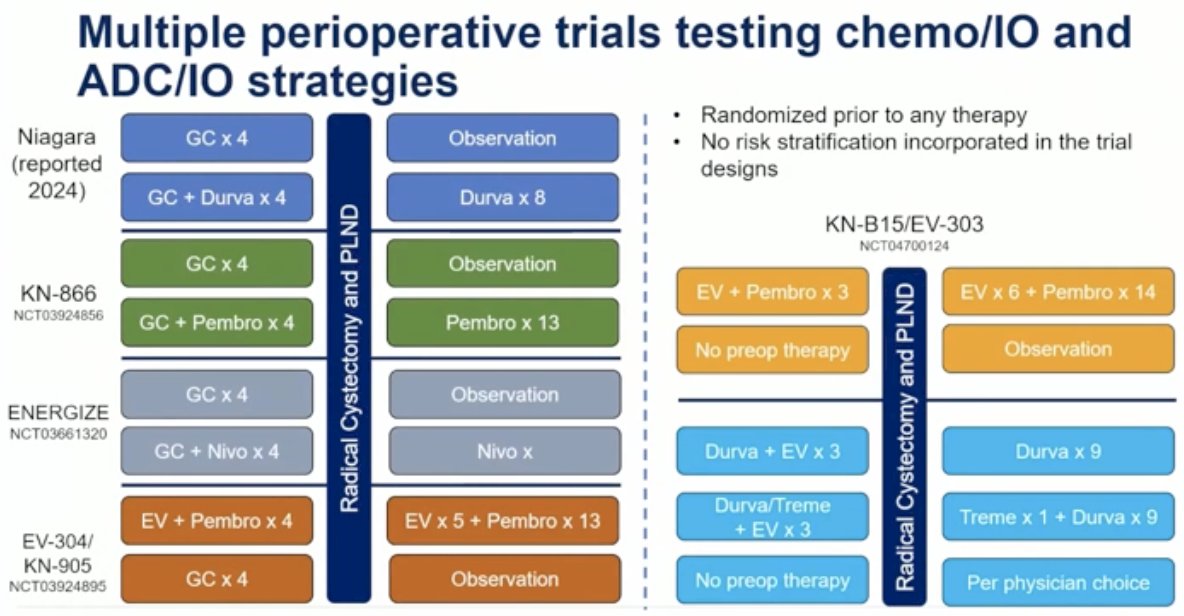
The NIAGARA trial has ushered in a new “sandwich approach” to perioperative therapy, shifting the previous paradigm of neoadjuvant cisplatin-based chemotherapy followed by adjuvant immunotherapy guided by pathologic stage.1 We are now entering an era where the same or similar treatments are administered both before and after surgery. Whether this represents the optimal strategy remains to be seen; alternative approaches may prove more effective. Unfortunately, none of the current studies have adopted a risk-adapted design. As Dr. Rosenberg noted, multiple perioperative trials are evaluating chemotherapy, immunotherapy, and ADC-based strategies, but all were randomized prior to any treatment and did not incorporate risk stratification into their designs.
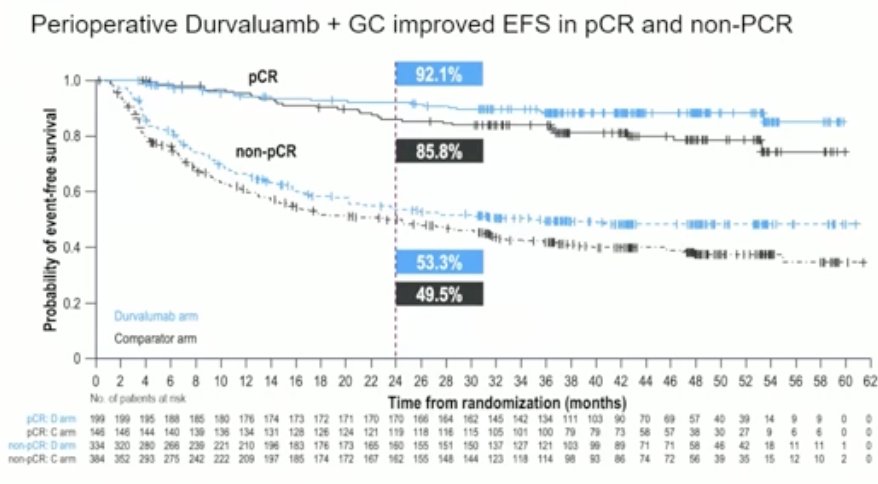
We now know that all patients appear to benefit from perioperative therapy, regardless of pathological outcomes. In NIAGARA, durvalumab improved event-free survival (EFS) across all pathologic stages at radical cystectomy, including in patients without pathologic downstaging. Similar trends were observed for overall survival (OS), with both pathologic responders (pCR) and non-responders deriving benefit. However, no postoperative risk assessment was performed in the trial. This raises an important question: do all patients truly need adjuvant durvalumab?2
The elephant in the room remains circulating tumor DNA (ctDNA). We know that its presence is prognostic, detectable ctDNA after radical surgery is strongly associated with an increased risk of recurrence. While ctDNA-negative patients tend to have better outcomes, relapse still occurs in some. Retrospective data from the IMvigor010 trial, despite its negative overall result, suggest that ctDNA-positive patients may benefit from adjuvant atezolizumab. However, no prospective phase III data to date have validated how to incorporate ctDNA alongside pathologic staging to guide treatment decisions in the adjuvant setting.5
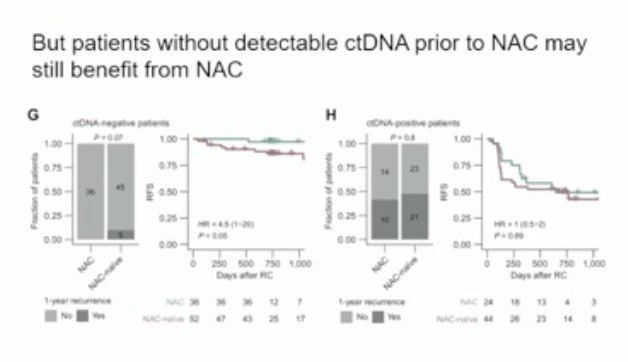
Emerging data confirm that ctDNA is a strong prognostic marker in MIBC. Its presence correlates with worse outcomes at multiple timepoints: prior to neoadjuvant chemotherapy (NAC), following NAC but before radical cystectomy, and post-cystectomy. At each stage, detectable ctDNA consistently identifies patients at higher risk of recurrence, reinforcing its potential role in dynamic risk stratification throughout the treatment course. However, patients without detectable ctDNA prior to NAC may still benefit from NAC, as shown in the survival curves below.
Analysis from the IMvigor010 trial, a negative study of adjuvant atezolizumab, revealed that ctDNA-negative patients not only failed to benefit from treatment but may have experienced worse outcomes compared to observation alone.5

Importantly, over 30% of patients who are ctDNA-negative still go on to relapse, underscoring that this biomarker, while promising, is not yet perfect. In IMvigor010, patients with detectable ctDNA derived a disease-free survival (DFS) benefit from adjuvant atezolizumab. This raises a critical question: if a more effective drug were used, would we have seen improved outcomes even in the ctDNA-negative group?
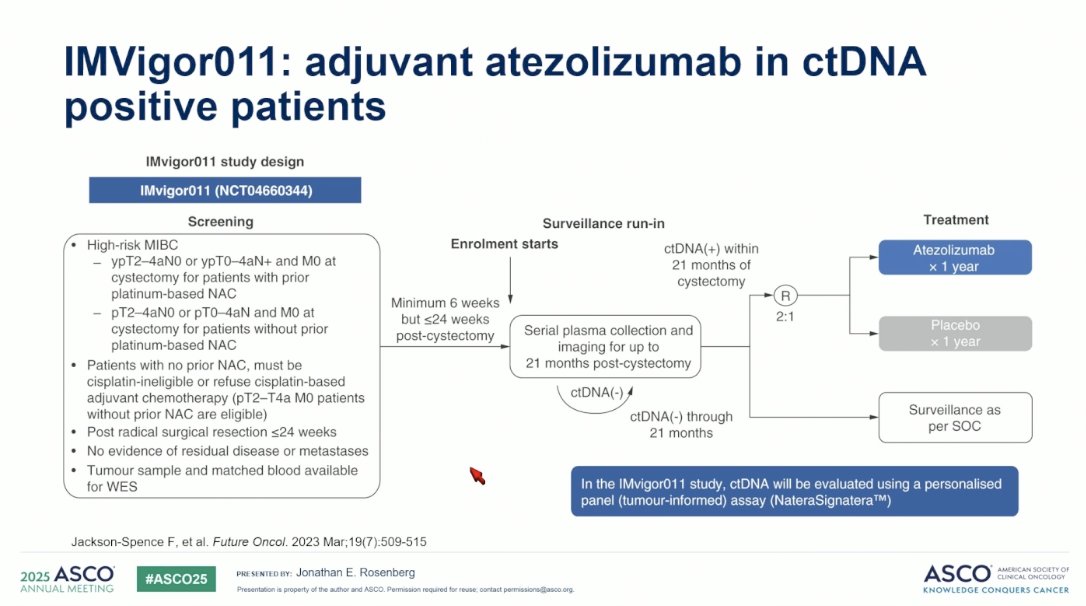
IMvigor011 is a biomarker-selected, randomized phase III trial evaluating adjuvant atezolizumab versus placebo in patients with MIBC, based on ctDNA status after RC. The study aims to determine whether ctDNA can effectively guide adjuvant immunotherapy decisions by selecting patients at higher risk of recurrence who may benefit from additional treatment.7
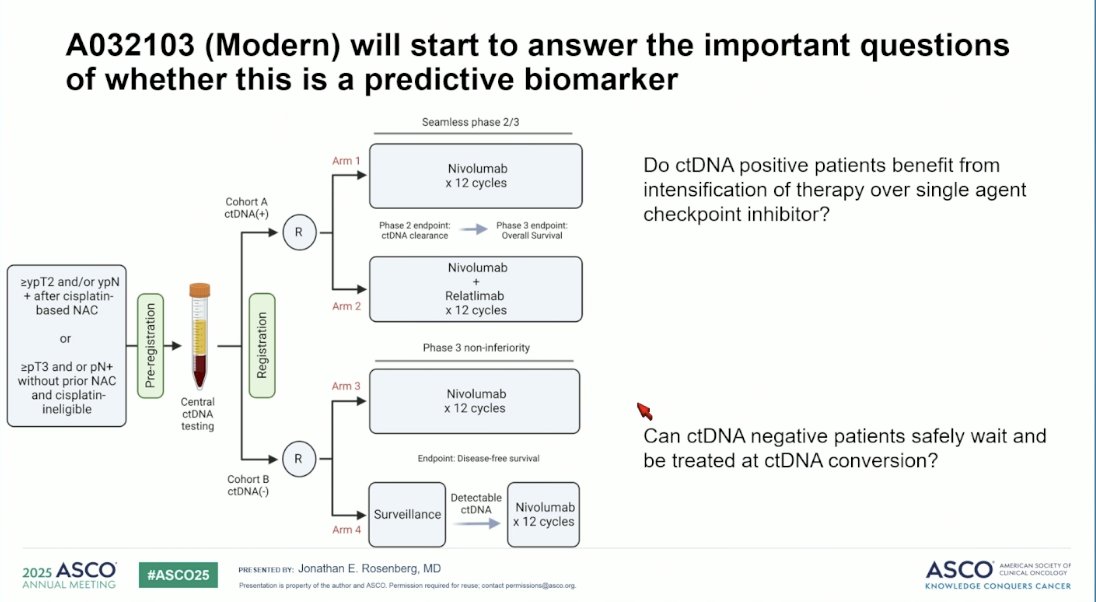
Moreover, the MODERN (A032103) trial is designed to address two key clinical questions: Is adjuvant immunotherapy necessary for ctDNA-negative patients, and do ctDNA-positive patients benefit from treatment intensification beyond single-agent checkpoint inhibition? This is a phase 2/3 trial evaluating ctDNA-guided adjuvant immunotherapy following RC. ctDNA-positive patients are randomized to receive nivolumab alone or in combination with relatlimab, while ctDNA-negative patients are randomized to either surveillance or nivolumab, aiming to determine whether treatment can be safely deferred until ctDNA conversion.8
Dr. Rosenberg highlighted that while PD-L1 status has demonstrated clinical utility in guiding immune checkpoint blockade across multiple cancer types, it has not been widely adopted as a clinically useful biomarker in urothelial cancer in the U.S. In contrast, the European Medicines Agency (EMA) has restricted the use of adjuvant nivolumab to patients whose tumors are PD-L1 positive, reflecting a regional divergence in biomarker-driven treatment decisions.
In the CheckMate 274 study, adjuvant nivolumab demonstrated a significant improvement in disease-free survival (DFS) and showed a trend toward improved overall survival (OS) in an unselected population of patients with urothelial carcinoma following radical cystectomy as shown below.3

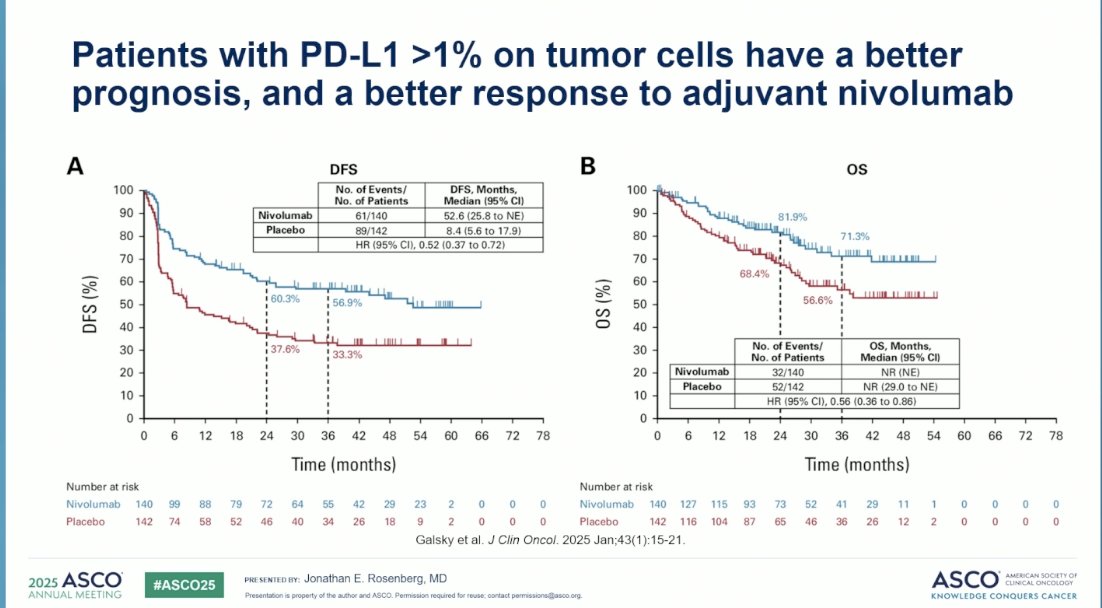
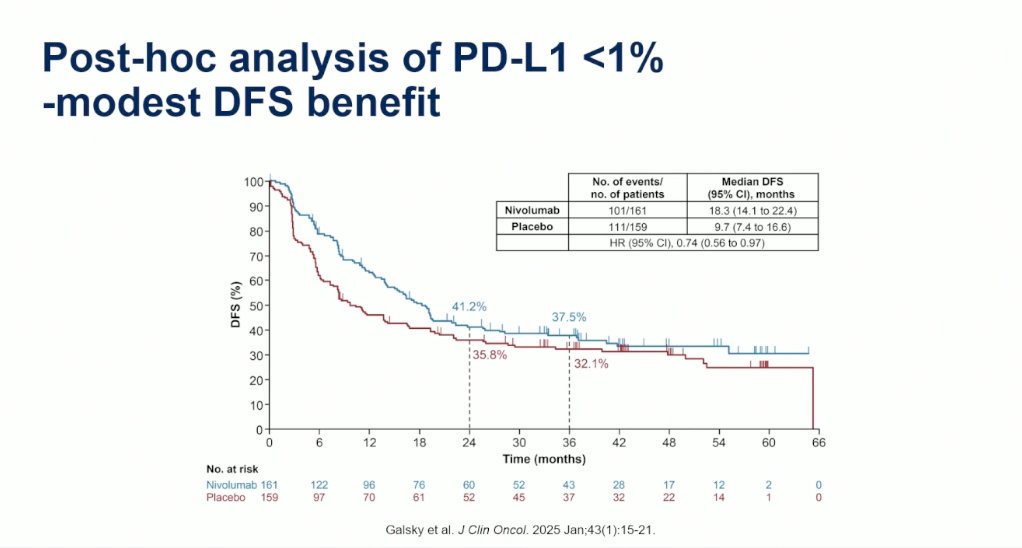
An exploratory analysis of CheckMate 274, showed that in patients with PD-L1 expression ≥1% experience significantly better outcomes when treated with adjuvant nivolumab, demonstrating notably improved disease-free and overall survival compared to PD-L1 negative patients with a HR for OS of 0.56 (95% CI, 0.36 to 0.86) in the PD-L1 ≥1 population. This highlights the potential utility of PD-L1 as a predictive biomarker for selecting patients who may derive the greatest benefit from immune checkpoint blockade in the adjuvant setting.9

Dr. Rosenberg concluded his presentation with the following key takeaways:
- Perioperative treatment is now a standard of care for cisplatin-eligible patients following the NIAGARA trial, without the need for risk stratification.
- The role of ctDNA following surgery in the perioperative setting remains unclear; ongoing studies like the MODERN trial may clarify its utility in the future.
- PD-L1 status is considered in some regions, but it is not currently used in clinical decision-making in the United States.
- At least five phase III trials evaluating perioperative strategies are underway and are expected to further shape and evolve the treatment landscape.
Presented by: Jonathan E. Rosenberg, MD, Genitourinary Oncologist at Memorial Sloan Kettering Cancer Center, New York, NY.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Pfister C, Gravis G, Fléchon A, Soulié M, Guy L, Laguerre B, Mottet N, Joly F, Allory Y, Harter V, Culine S; VESPER Trial Investigators. Randomized Phase III Trial of Dose-dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin, or Gemcitabine and Cisplatin as Perioperative Chemotherapy for Patients with Muscle-invasive Bladder Cancer. Analysis of the GETUG/AFU V05 VESPER Trial Secondary Endpoints: Chemotherapy Toxicity and Pathological Responses. Eur Urol. 2021 Feb;79(2):214-221. doi: 10.1016/j.eururo.2020.08.024. Epub 2020 Aug 28. PMID: 32868138.
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021;384(22):2102–2114.
- Apolo AB, Ballman KV, Sonpavde G, Berg S, Kim WY, Parikh R, Teo MY, Sweis RF, Geynisman DM, Grivas P, Chatta G, Reichert ZR, Kim JW, Bilen MA, McGregor B, Singh P, Tripathi A, Cole S, Simon N, Niglio S, Ley L, Cordes L, Srinivas S, Huang J, Odegaard M, Watt C, Petrylak D, Hoffman-Censits J, Wen Y, Hahn O, Mitchell C, Tan A, Streicher H, Sharon E, Moon H, Woods M, Halabi S, Perez Burbano G, Morris MJ, Rosenberg JE. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2025 Jan 2;392(1):45-55. doi: 10.1056/NEJMoa2401726. Epub 2024 Sep 15. PMID: 39282902; PMCID: PMC11698643.
- Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(4):525–537.
- Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL, deVere White RW, Sarosdy MF, Wood DP Jr, Raghavan D, Crawford ED. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003 Aug 28;349(9):859-66. doi: 10.1056/NEJMoa022148. Erratum in: N Engl J Med. 2003 Nov 6;349(19):1880. PMID: 12944571.
- Powles T, Loriot Y, Bellmunt J, et al. IMvigor011: A Phase III study of adjuvant atezolizumab in patients with muscle-invasive bladder cancer (MIBC) guided by circulating tumor DNA (ctDNA). Ann Oncol. 2021;32(suppl_5):S1314. doi:10.1016/annonc/annonc720
- Galsky MD, Srinivas S, Grivas P, et al. A032103: Phase II/III trial of ctDNA-guided therapy in urothelial cancer (MODERN). J Clin Oncol. 2023;41(16_suppl):TPS4612. doi:10.1200/JCO.2023.41.16_suppl.TPS4612
- Galsky MD, Witjes JA, Gschwend JE, Milowsky MI, Schenker M, Valderrama BP, Tomita Y, Bamias A, Lebret T, Shariat SF, Park SH, Agerbaek M, Jha G, Stenner F, Ye D, Giudici F, Dutta S, Askelson M, Nasroulah F, Zhang J, Brophy L, Bajorin DF. Adjuvant Nivolumab in High-Risk Muscle-Invasive Urothelial Carcinoma: Expanded Efficacy From CheckMate 274. J Clin Oncol. 2025 Jan;43(1):15-21. doi: 10.1200/JCO.24.00340. Epub 2024 Oct 11. PMID: 39393026; PMCID: PMC11687940.