(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the session Advancing Perioperative Treatment Options for Localized Muscle-Invasive Bladder Cancer: A Step Forward. Dr. Maria Jose Ribal discussed the Integration of Universal Perioperative Immunotherapy in this disease space.
Dr. Ribal opened by highlighting how immunotherapy has transformed the treatment landscape of bladder cancer. What began as a breakthrough in advanced disease now holds the potential to redefine curative strategies in earlier stages. However, to understand this shift, we must reflect on the journey from disruption to evolution in perioperative therapy for muscle-invasive bladder cancer. It has been over 20 years since neoadjuvant chemotherapy (NAC) was first offered prior to surgery, dating back to 2003.1 Yet two decades later, we still lack reliable markers to predict who will respond. As Dr. Ribal noted, these unanswered questions will continue to challenge clinical decision-making in everyday practice.
An option is a universal perioperative treatment approach, in which immunotherapy is administered both before and after surgery to maximize curative potential in MIBC. This strategy ensures that all patients receive the potential benefit of immunotherapy early in the treatment course and may enhance the immune response while the tumor antigen is still present. As Dr. Ribal emphasized, this approach is justified by the inherently aggressive nature of MIBC and its high risk of recurrence. In contrast, a risk-adapted model may delay immune checkpoint inhibition (ICI) and risk leaving some patients undertreated, while we still don’t have biomarkers in clinical practice for a risk-adapted approach.
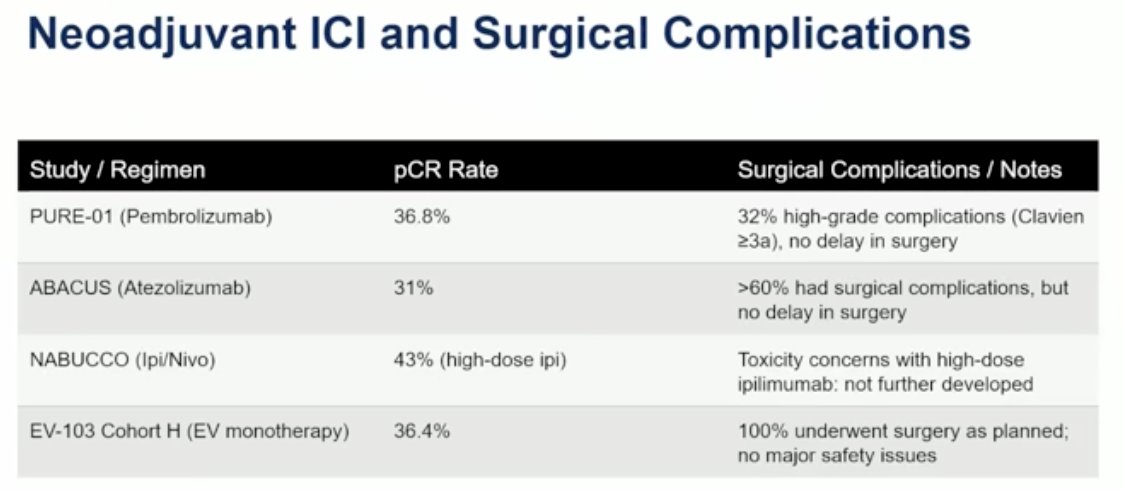
The PURE-01 study demonstrated that neoadjuvant pembrolizumab is safe and can induce a high pathologic complete response (pCR) rate of 42%. These durable responses support early use of ICIs. Importantly, neoadjuvant immunotherapy did not compromise surgical outcomes, reinforcing its feasibility and safety prior to radical cystectomy. While biomarkers did not reliably guide patient selection, this further supports the rationale for a universal approach.
This strategy is not limited to pembrolizumab similar approaches have been tested across multiple trials, including atezolizumab in ABACUS, enfortumab vedotin and ICI combinations in EV-103, and nivolumab plus ipilimumab in the NABUCCO study. Collectively, these findings lay the foundation for the current perioperative paradigm.2-4
Neoadjuvant immunotherapy and immunochemotherapy lay the foundation for emerging perioperative strategies in MIBC. Durable responses can be achieved with immunotherapy alone, even in the absence of chemotherapy, reinforcing its role in cisplatin-eligible patients. This supports a more inclusive, not selective approach to treatment. Importantly, preoperative immunotherapy does not compromise surgical feasibility or outcomes, further validating its routine use. While biomarker-driven selection remains a challenge due to current limitations, these uncertainties support the rationale for a universal approach one that is both safer and more equitable.
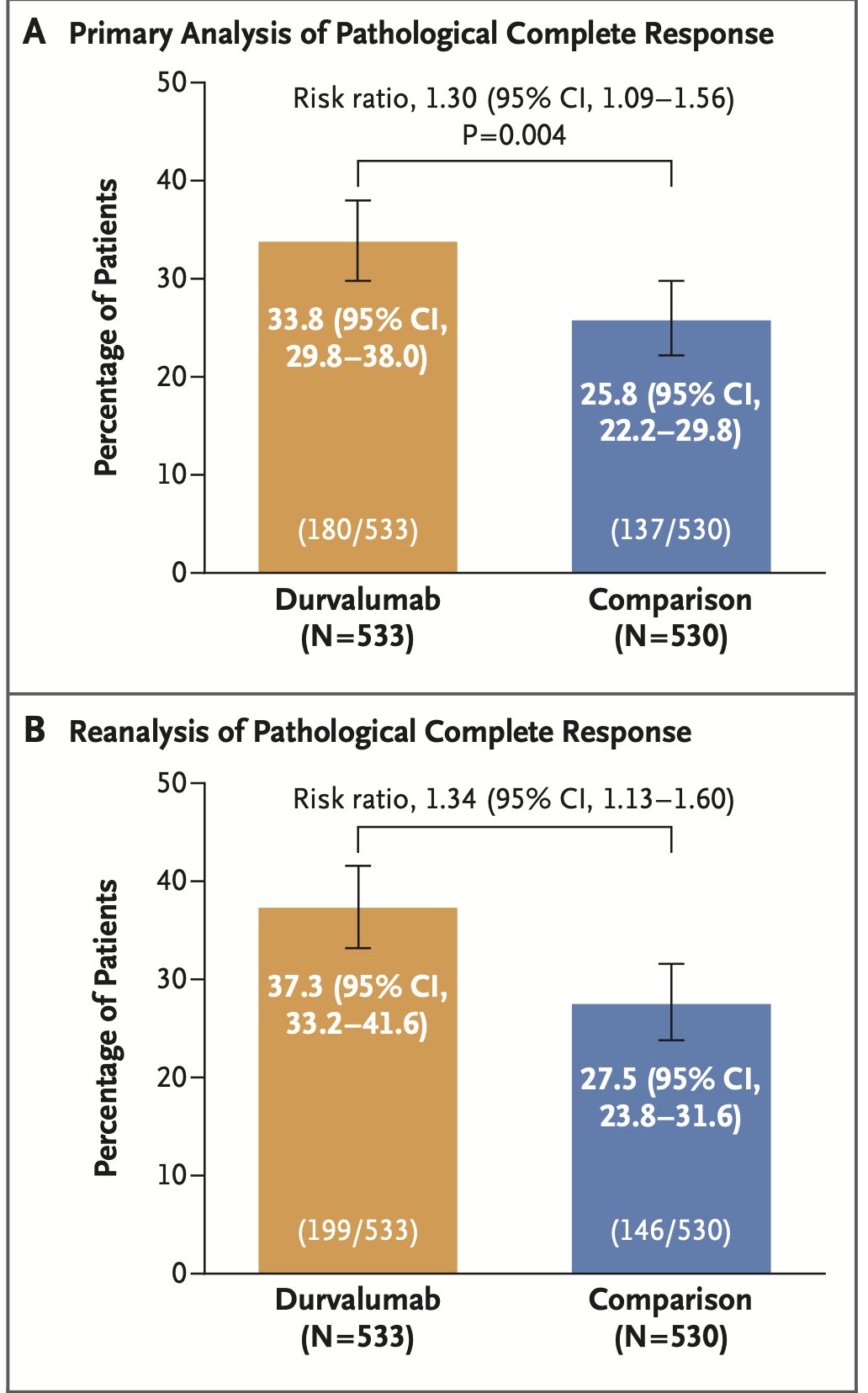
One trial that has helped reshape the field of MIBC is the NIAGARA study, presented at ESMO last year. This trial evaluated neoadjuvant gemcitabine and cisplatin combined with durvalumab for four cycles, followed by radical cystectomy and then adjuvant durvalumab for up to eight additional cycles. This regimen was compared to standard-of-care NAC followed by surgery. The co-primary endpoints were EFS) and pCR, both of which were met.5 pCR was 37% in the experimental arm vs. 27% in the control arm, in the second analysis.
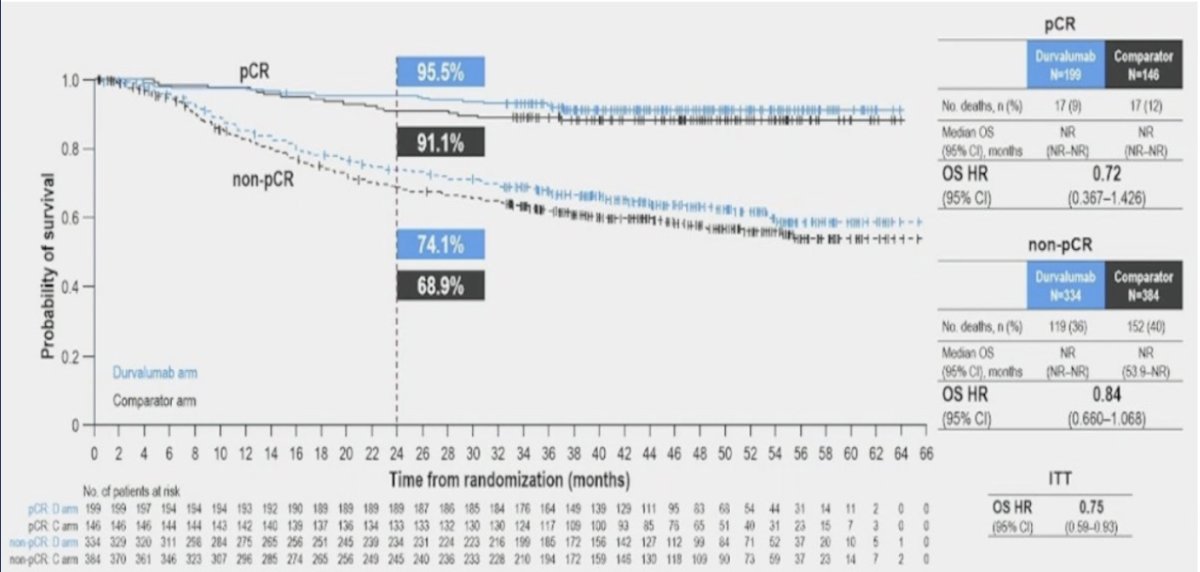
A post-hoc analysis of the NIAGARA trial demonstrated that durvalumab improved event-free and overall survival regardless of whether patients achieved a pathologic complete response or not, reinforcing the benefit of a perioperative approach across pathologic subgroups, as illustrated below.
The toxicity profile of the “sandwich” approach in NIAGARA was manageable. Immune-related adverse events occurred in 21% of patients receiving durvalumab, with only 3% experiencing grade 3/4 events. The most common imrAEs were thyroid-related, 10% developed hypothyroidism, and 3% hyperthyroidism. Most adverse events were manageable and had resolved by the time of data cutoff. Surgical outcomes were not compromised: complications were similar across arms, 95% of patients underwent radical cystectomy within 70 days of neoadjuvant therapy, and 75% were able to complete all eight cycles of adjuvant durvalumab. These findings support the safety and feasibility of perioperative immunotherapy and led to regulatory approval of this approach by both the FDA and EMA in 2024.
However, it’s important to critically assess any new treatment paradigm, including the universal perioperative approach. Key questions remain unanswered. First, the independent value of adjuvant therapy is unclear; trials like NIAGARA do not distinguish the contribution of neoadjuvant versus adjuvant durvalumab. Second, there is a real risk of overtreatment: 30–40% of patients achieve a pCR do all of them need adjuvant ICI? Third, while current data are reassuring, the potential surgical impact of neoadjuvant immunotherapy must be continuously monitored. Finally, the absence of validated biomarkers remains a challenge; tools like ctDNA and PD-L1 expression could help tailor escalation or de-escalation strategies.

Due to its design, the NIAGARA trial cannot address several key questions. It was intended to evaluate the perioperative “sandwich” strategy as a unified approach, rather than to isolate the individual contributions of the neoadjuvant combination or adjuvant durvalumab. Nor was it designed to assess the potential for de-escalation in patients achieving a pCR. The observed survival benefits in both pCR and non-pCR groups may reflect sustained neoadjuvant immune activity rather than a definitive role for adjuvant therapy. Notably, the absolute OS benefit in the pCR subgroup was just 4%, raising the question of whether this difference is clinically meaningful.
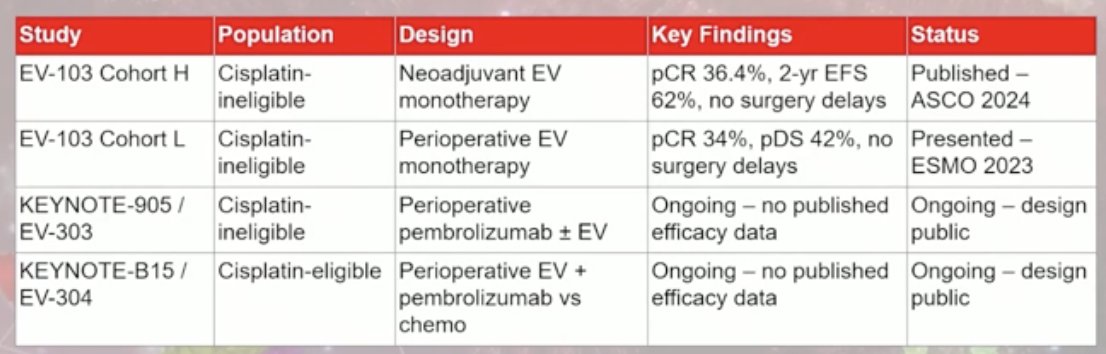
Dr. Ribal emphasized the need for new trial designs to address a key limitation of the NIAGARA study: its inability to disentangle the specific contributions of neoadjuvant versus adjuvant therapy. Future studies should evaluate agents like enfortumab vedotin (EV) in each phase independently and in combination to determine their individual and additive effects. Encouragingly, several trials are already underway aiming to answer these critical questions.
The control arm of the NIAGARA trial had several key limitations. First, adjuvant immune checkpoint inhibitors were not permitted, control patients did not receive nivolumab, which has since become a standard of care for high-risk patients based on CheckMate 274.6 Second, the trial restricted neoadjuvant chemotherapy to gemcitabine-cisplatin, excluding dose-dense MVAC, a valid and widely used alternative regimen. Lastly, there was no incorporation of biomarker-guided strategies such as ctDNA, limiting the ability to identify which patients might truly benefit from adjuvant therapy and raising concerns about potential overtreatment.
However, despite the limitations of the control arm in NIAGARA, these do not invalidate the benefits observed. The improvements in event-free and overall survival represent meaningful clinical progress. Even if the comparator was suboptimal, the perioperative strategy demonstrated in NIAGARA is feasible, safe, and effective. A universal immunotherapy approach ensures early exposure to treatment, offering protection during a period of high risk while we continue to refine biomarker-driven strategies.
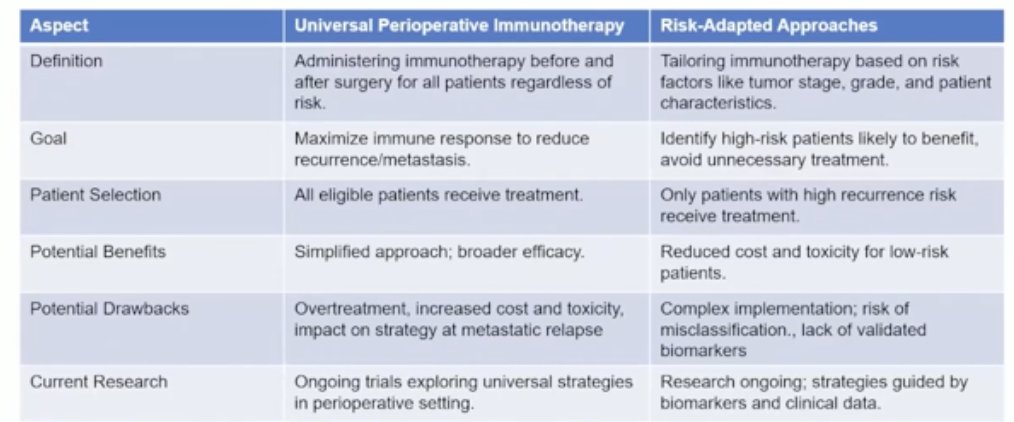
Dr. Ribal emphasized that we are now at a crossroads with the emergence of universal perioperative immunotherapy. This approach aims to maximize the immune response early, with the goal of reducing recurrence and metastatic progression. However, it may come at the cost of overtreatment, increased toxicity, and higher healthcare expenditures. The long-term impact of this strategy on outcomes after metastatic relapse also remains uncertain. Alternatively, a risk-adapted approach could offer a more tailored solution with the caveat that we don’t have validated biomarkers to guide treatment decisions.
Dr. Ribal concluded her presentation with the following key points:
- The NIAGARA trial showed a clear EFS and OS benefit with the perioperative strategy as a whole.
- Without knowing which phase is critical, the safest option is to offer full coverage (Universal perioperative treatment) to all eligible patients.
- Universal does not mean rigid, it can evolve with biomarkers and future data.
- In the absence of validated selection tools, overtreatment is safer than undertreatment.
- In bladder cancer, we are living in exciting times, especially in the metastatic setting, while current efforts are aiming to reshape how we treat localized disease.
- Our goal should be to offer curative therapy to these patients, because we should be able to cure them.
Presented by: Maria Jose Ribal, MD, PhD, Head of the Urologic Oncology Section. Hospital Clinic Barcelona. Barcelona, Spain.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL, deVere White RW, Sarosdy MF, Wood DP Jr, Raghavan D, Crawford ED. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003 Aug 28;349(9):859-66. doi: 10.1056/NEJMoa022148. Erratum in: N Engl J Med. 2003 Nov 6;349(19):1880. PMID: 12944571.
- Necchi A, Anichini A, Raggi D, Briganti A, Massa S, Lucianò R, Colecchia M, Giannatempo P, Mortarini R, Bianchi M, Farè E, Monopoli F, Colombo R, Gallina A, Salonia A, Messina A, Ali SM, Madison R, Ross JS, Chung JH, Salvioni R, Mariani L, Montorsi F. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J Clin Oncol. 2018 Dec 1;36(34):3353-3360. doi: 10.1200/JCO.18.01148. Epub 2018 Oct 20. PMID: 30343614.
- Szabados B, Kockx M, Assaf ZJ, van Dam PJ, Rodriguez-Vida A, Duran I, Crabb SJ, Van Der Heijden MS, Pous AF, Gravis G, Herranz UA, Protheroe A, Ravaud A, Maillet D, Mendez MJ, Suarez C, Linch M, Prendergast A, Tyson C, Stanoeva D, Daelemans S, Rombouts M, Mariathasan S, Tea JS, Mousa K, Sharma S, Aleshin A, Banchereau R, Castellano D, Powles T. Final Results of Neoadjuvant Atezolizumab in Cisplatin-ineligible Patients with Muscle-invasive Urothelial Cancer of the Bladder. Eur Urol. 2022 Aug;82(2):212-222. doi: 10.1016/j.eururo.2022.04.013. Epub 2022 May 14. PMID: 35577646.
- O'Donnell PH, Milowsky MI, Petrylak DP, Hoimes CJ, Flaig TW, Mar N, Moon HH, Friedlander TW, McKay RR, Bilen MA, Srinivas S, Burgess EF, Ramamurthy C, George S, Geynisman DM, Bracarda S, Borchiellini D, Geoffrois L, Maroto Rey JP, Ferrario C, Carret AS, Yu Y, Guseva M, Homet Moreno B, Rosenberg JE. Enfortumab Vedotin With or Without Pembrolizumab in Cisplatin-Ineligible Patients With Previously Untreated Locally Advanced or Metastatic Urothelial Cancer. J Clin Oncol. 2023 Sep 1;41(25):4107-4117. doi: 10.1200/JCO.22.02887. Epub 2023 Jun 27. PMID: 37369081; PMCID: PMC10852367.
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021;384(22):2102–2114.