(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a biomarkers in kidney cancer session. Dr. Renee Saliby presented the results of a randomized, 1st line clinical trial evaluating gut-associated checkpoint as a prognostic biomarker in metastatic renal cell carcinoma (RCC).
In recent years, the case for the microbiome, particularly the gut microbiome, as a key player in cancer has grown tremendously. There is increasing evidence that the microbiome is an active participant in tumorigenesis and progression. It shapes immune responses and influences treatment outcomes. Dr. Saliby noted that it is now being recognized as a ‘hallmark of cancer’, a foundational element alongside genomic instability, immune evasion, and other core traits.1,2 This represents a paradigm shift, with tremendous implications for how we study, diagnose, and treat cancer moving forward.

While the exact mechanisms through which the microbiome exerts its effects on cancer development and progression remain to be definitively determined, Dr. Saliby highlighted one emerging pathway – Yonekura and colleagues showed that extraintestinal tumors can induce a form of stress ileopathy characterized by anatomical and functional changes in the gut leading to increased sympathetic signaling. This in turn increases gut permeability and creates a niche for sustained dysbiosis, particularly favoring gram-positive species from the Enterocloster genus. This results in a feedback loop that fuels cancer progression from a distance.3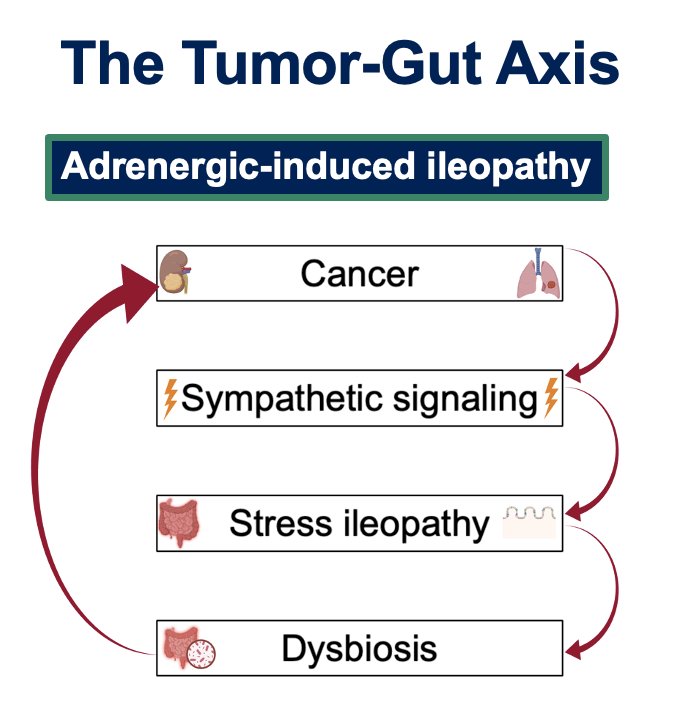
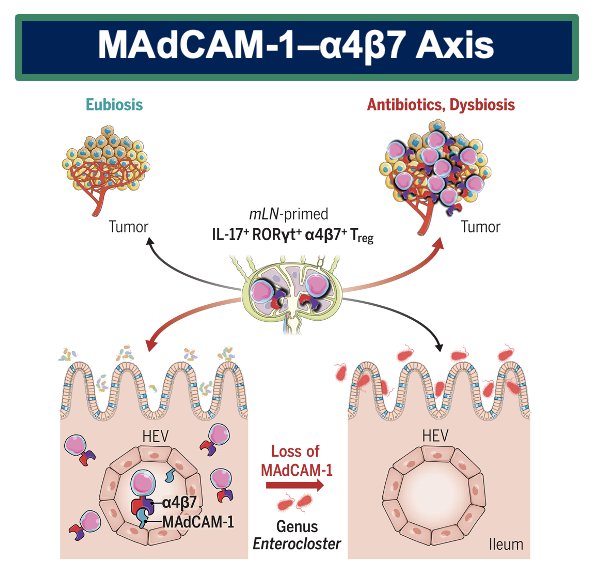
A similar gut permeability theory has also been evaluated by Fidelle et al, as illustrated below. Gut dysbiosis downregulates mucosal addressin cell adhesion molecule 1, MAdCAM-1, a gut-specific adhesion molecule that controls the migration of immune cells. In the context of gut dysbiosis, the downregulation of MAdCAM-1 leads to an exodus of immunosuppressive/regulatory T cells, known as Tr17 cells. They migrate to the tumor and tumor-draining lymph nodes, where they actively impair the efficacy of immune checkpoint blockade.4
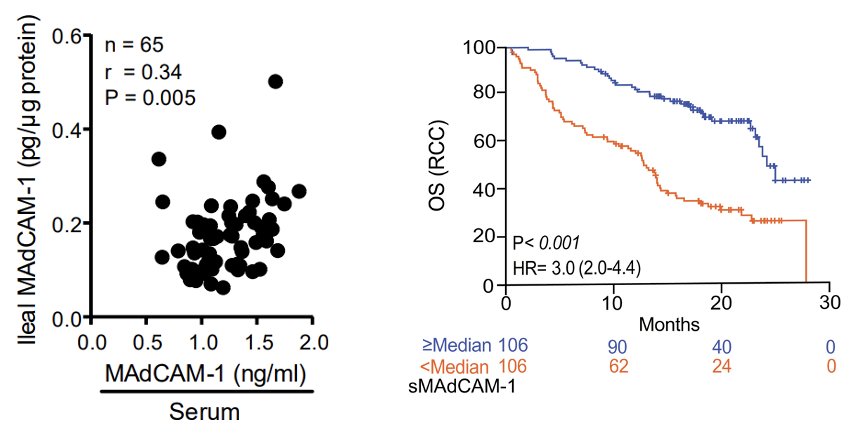
Importantly, serum MAdCAM-1 is representative of ileal MAdCAM-1, which means that we can reliably evaluate the gut microbiome using the serum level of MAdCAM-1. In patients receiving immunotherapy, low serum levels of soluble MAdCAM-1 were associated with gut dysbiosis and worse outcomes in renal, bladder, and lung cancers.4
Dr. Saliby and colleagues hypothesized that soluble MAdCAM-1 can serve as a biomarker of clinical outcomes in patients receiving first-line therapy for metastatic RCC. To this end, the study investigators performed an ad hoc analysis of the JAVELIN Renal 101 trial.5 Eligible patients with untreated, advanced RCC with a clear cell component were randomized to avelumab + axitinib versus sunitinib therapy. Patients underwent baseline blood collection prior to Day 1 of Cycle 1, when soluble MAdCAM-1 levels were measured and were correlated with progression-free (PFS) and overall survivals (OS).
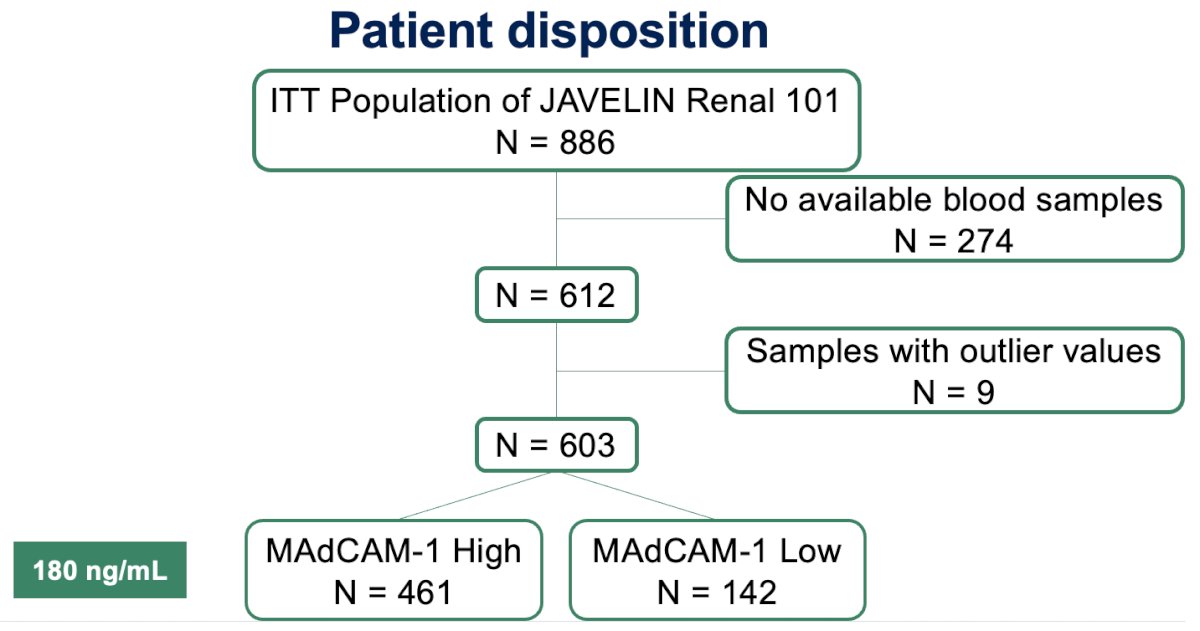
Of the 866 patients originally included in this trial, 612 patients with available treatment plasma samples were included. After excluding a small number of samples with outlier values, the final cohort included 603 patients. To stratify patients, they used the Contal and O’Quigley method – Martingale Residual to define an optimal cutoff for soluble MAdCAM-1—determined to be 180 ng/mL. Based on this threshold, they identified 461 patients with high MAdCAM-1 levels and 142 with low levels.
The baseline characteristics are summarized below. Both groups—high and low MAdCAM-1—were representative of the broader mRCC population. The median age was 61 years, approximately 75% were male, and around 60% fell into the intermediate IMDC risk category. Overall, the cohort reflects what is typically seen in real-world metastatic RCC.
IMDC poor risk patients had lower MAdCAM-1 levels, compared to those with IMDC favorable and intermediate risk disease. Additionally, patients who had not undergone a prior nephrectomy prior to systemic therapy initiation had lower MAdCAM-1 levels.

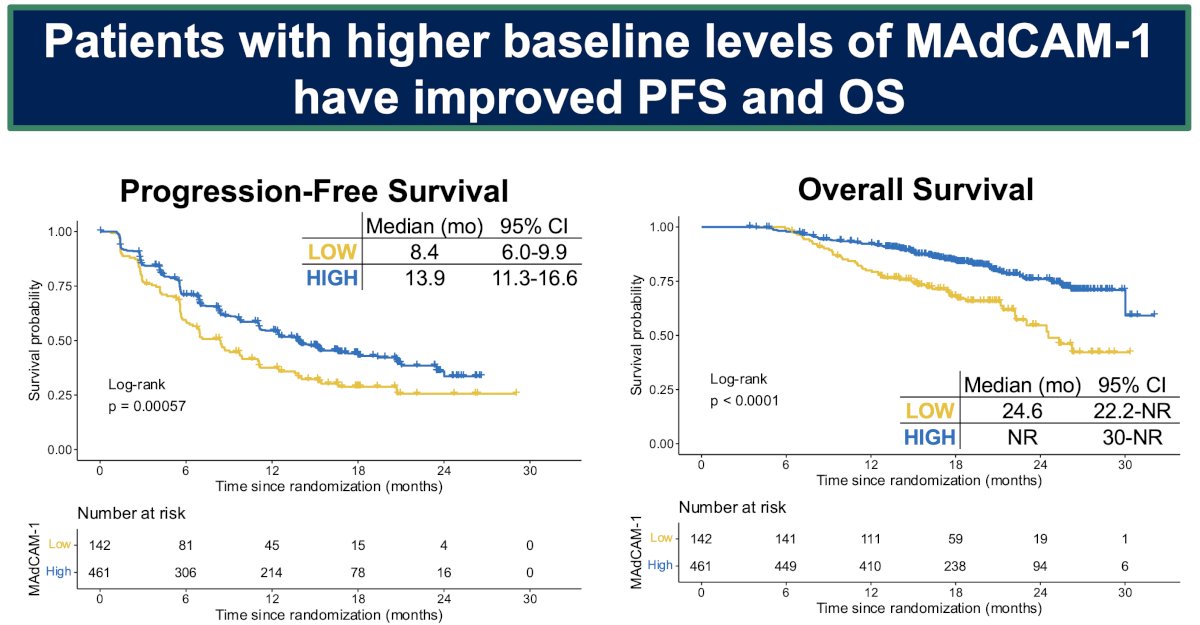
Patients with higher levels of soluble MAdCAM-1 (above 180 ng/mL) had significantly better survival outcomes. Their median progression-free survival was 13.9 months compared to 8.4 months in the low MAdCAM-1 group (p<0.01). A similar pattern was observed for OS – median OS was not yet reached in the high MAdCAM-1 group, versus 24 months in the low group (p<0.01).
These superior survival outcomes were observed irrespective of treatment received, highlighting MAdCAM-1 as a prognostic biomarker. In the avelumab + axitinib-treated patients, the median PFS was 18 versus 8.7 months in the MAdCAM-1 high and low groups, respectively. In sunitinib-treated patients, the corresponding values were 11.1 and 6.9 months, respectively.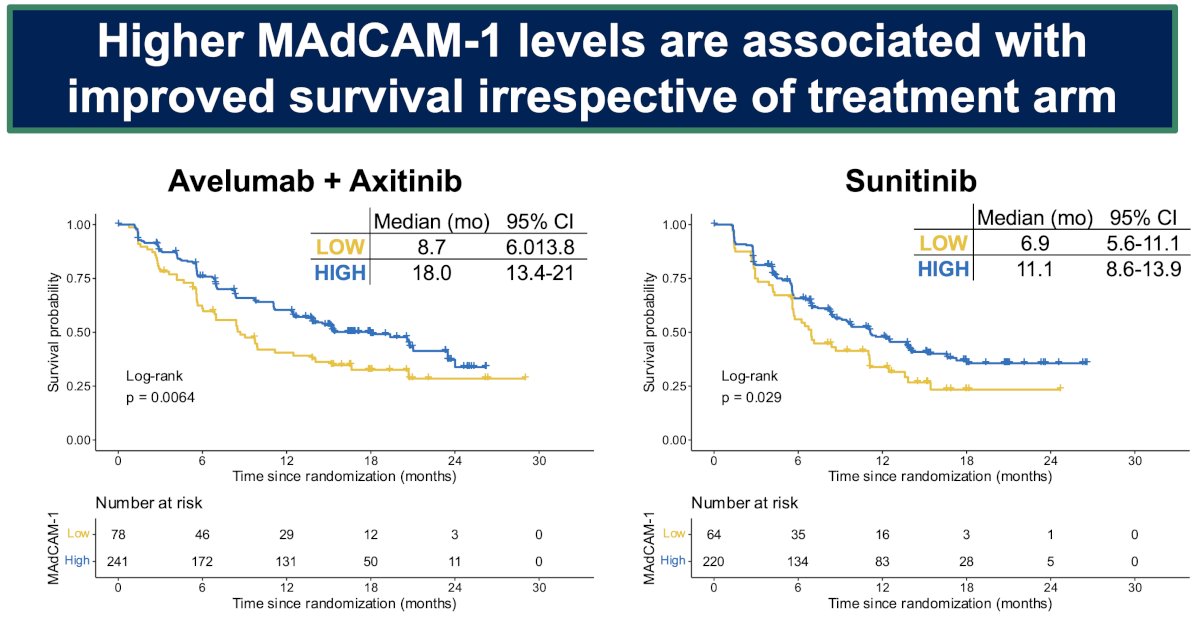
Multivariable modes adjusted for body mass index (BMI), prior nephrectomy status, and IMDC risk group confirmed serum MAdCAM-1 levels as significant predictors of PFS and OS.
Important limitations to this study include the following:
- Retrospective nature
- No data on antibiotics and other microbiome modulators
- Both arms contain a VEGF-TKI (known to alter the microbiome)
Dr. Saliby concluded as follows:
- Circulating levels of MAdCAM-1 are prognostic in metastatic RCC
- Patients with metastatic RCC and low MAdCAM-1 levels may benefit from microbiota-centered interventions
- Future steps include implementation of biomarker-targeted trials investigating microbiota-targeted interventions
Presented by: Renee Maria Saliby, MD, MSc, Resident Physician, Department of Medicine, Yale School of Medicine, New Haven, CT
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Hanahan D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022;12(1):31–46.
- Morad G, Helmink BA, Sharma P. Hallmarks of response, resistance, and toxicity to immune checkpoint blockade. Cell. 2021; 184(21): 5309–37.
- Yonekura S, Henning NJ, Filderman JN. Cancer Induces a Stress Ileopathy Depending on β-Adrenergic Receptors and Promoting Dysbiosis that Contributes to Carcinogenesis. Cancer Discov. 2022; 12 (4): 1128–1151.
- Fidelle M, et al. A microbiota-modulated checkpoint directs immunosuppressive intestinal T cells into cancers. Science. 2023; DOI: 10.1126/science.abo2296.
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. 2019; 380(12):1103-1115.