(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to a State of the Science session on novel diagnostics and therapeutics in renal cell and urothelial carcinomas. Dr. Wulff-Burchfield discussed strategies for bridging innovation and community practice for the use of antibody-drug conjugates (ADCs) in urothelial carcinoma.
The concept of the “magic bullet” treatment for cancer dates back to Dr. Paul Ehrlich, who described this as the ultimate goal for antimicrobial and antineoplastic treatment.1 Work on early ADC iterations began as early as the 1980s, with monoclonal antibody development a crucial milestone for ADC innovation. Gemtuzumab ozgamicin was the first FDA-approved ADC (later withdrawn) in 2000, and as of ASCO 2025, seventeen are approved for the treatment of cancer.
ADCs are made of three components:2
- A monoclonal antibody (mAb) targeting a cell surface antigen
- Needs to be highly expressed on tumor cells and have limited expression on healthy tissues
- Linker molecule
- Stable in circulation with efficient release of the cytotoxic agent
- Payload drug:
- Must be highly potent
- Only 1-2% of payload drugs reach the tumor sites
- As of ASCO 2025, all approved ADCs have cytotoxic payloads, but this is expanding

What are the available ADCs in urothelial carcinoma? Enfortumab vedotin (EV) is a fully humanized monoclonal antibody directed toward nectin-4, with a monomethyl auristatin (MMAE) payload.3 Its key adverse effects are peripheral neuropathy and skin toxicity. It received accelerated FDA approval following the publication of the EV-201 trial (NCT03219333). This trial included patients with metastatic/unresectable urothelial carcinoma following platinum chemotherapy and immune checkpoint inhibitor (ICI) therapy. The objective response rate was 44% (complete: 12%, partial: 32%), with a median duration of response of 7.6 months.3

The randomized phase III EV-301 trial (NCT0347107) redemonstrated the efficacy of EV for advanced/unresectable urothelial carcinoma following prior treatment with platinum chemotherapy and ICI therapy.4 Compared to chemotherapy, EV demonstrated superior overall survival (median: 12.9 vs 9 months; HR: 0.70, p=0.001), progression-free survival (median: 5.6 vs 3.7 months; HR: 0.62, p<0.001), and objective response rate (40.6% vs 18%, p<0.001).4

Building on the success of earlier trials of EV and applying data suggesting that ADC-mediated cell death may increase tumor susceptibility to ICI therapy,5 the EV-302 trial (NCT04223856) investigated first-line EV + pembrolizumab versus platinum chemotherapy (+/-avelumab maintenance).5 The co-primary endpoints were PFS and OS. The combination of EV + pembrolizumab demonstrated superior PFS (median: 12.5 vs 6.3 months; HR: 0.45, p<0.001) and OS (median: 31.5 vs 16.5 months; HR: 0.47, p<0.001) versus platinum chemotherapy. Patients receiving EV + pembrolizumab also had superior ORRs (68% vs 44.4%, p<0.001). These results of the EV-302 trial led to the approval of EV + pembrolizumab as 1st line therapy for locally advanced/metastatic urothelial carcinoma.5

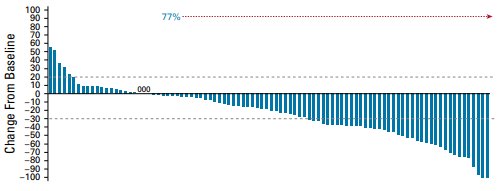
Sacituzumab govitecan (SG) is the second ADC approved for the treatment of urothelial carcinoma, although the approval was subsequently withdrawn. It is a humanized monoclonal antibody directed against trophoblast cell antigen 2 (Trop-2) with a topoisomerase 1 inhibitor (SN38) payload. Its key adverse effects are neutropenia/febrile neutropenia and gastrointestinal toxicity. The phase II TROPHY-U-01 trial (NCT03547973) included patients with metastatic/unresectable urothelial carcinoma with disease progression following platinum chemotherapy and ICI therapy. The ORR (primary outcome) was 28%. The median PFS and OS were 5.4 and 10.9 months, respectively.7
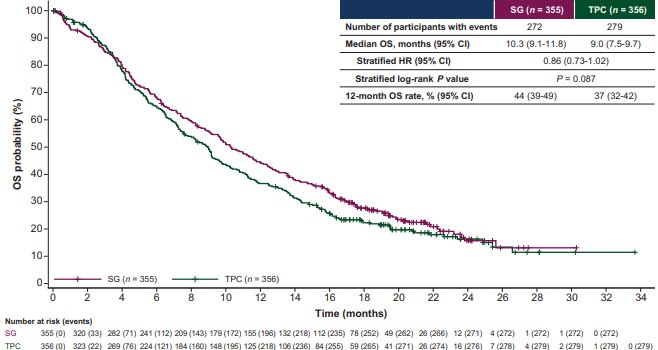
The phase III TROPiCS-04 trial (NCT04527991) evaluated SG versus standard chemotherapy for advanced/unresectable UCC for patients with prior treatment with platinum chemotherapy and ICI therapy. The median OS (primary outcome) was 10.3 versus 9 months (HR: 0.86, p=0.087). Following the TROPicS-04 trial, the FDA withdrew approval for SG for advanced/unresectable UCC.8
Trastuzumab deruxtecan (T-DXd) is a humanized monoclonal antibody targeting HER2, with a Topoisomerase 1 inhibitor (DX-8951) payload. The key adverse effects are gastrointestinal toxicity, cardiotoxicity, and interstitial lung disease. The DESTINY-Pantumor-01 trial evaluated T-DXd for patients with metastatic biliary, urothelial, cervical, endometrial, and pancreatic cancers with HER2 2+/3+ expression following ≥1 lines of therapy. In the urothelial carcinoma cohort, the ORR was 56.3%. The median PFS and OS were 7 and 12.8 months, respectively.9,10
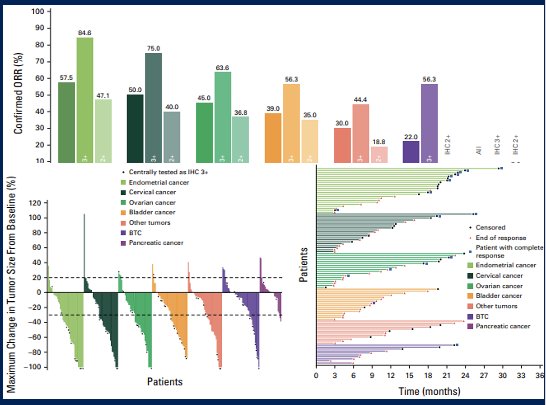
Following this data from DESTINY-Pantumor-01, as well as DESTINY-Lung01 and DESTINY-CRC02, TDXd received accelerated FDA approval for adults with advanced/unresectable HER2 positive (3+ by gastric assay) solid tumors. This is the first tumor agnostic approval for an ADC.
Disitamab vedotin (DV) is a humanized monoclonal antibody targeting HER2, with an MMAE payload.11 Its key adverse effect is peripheral sensory neuropathy. In the open label, phase II RC48-C005 (NCT03507166) and RC48-C009 (NCT03809013) trials, DV was investigated for patients with advanced/unresectable urothelial carcinoma with HER2 2+ or 3+ following chemotherapy. The ORR (primary outcome) was 50.5%, with complete and partial responses of 1.9% and 48.6%, respectively. Additionally, 32% of patients had stable disease. The median PFS and OS were 5.8 and 14.2 months, respectively.11 DV received FDA breakthrough designation in 2020 and is now approved for use in China.

What are the considerations for ADC implementation in urothelial carcinoma in community practice? Approximately 85% of patients treated for cancer in the US receive care in a community setting.12 Most oncologists (66%) have a scope of practice that reflects US cancer epidemiology.13 Oncologists practicing in the community setting have less access to clinical trials, may not be empowered to order molecular diagnostic tests for their patients, and experience variability in the interpretation of commercial next generation sequencing testing.14-17 Community oncologists also face unique financial pressures related to up-front costs for testing and medications, and increased administrative burden related to value-based care models.18-20
All of these and other factors contribute to variability in the pattern/timing of adoption of emerging cancer treatments. Earlier adoption of novel cancer treatments in community practice are associated with the following:21,22
- Urban location
- Independent practices
- Practices with more than 5 physicians
- Practice location within the same region as lead investigators on pivotal trials
This swimlane diagram summarizes the personnel, roles, and processes required to implement targeted therapy:
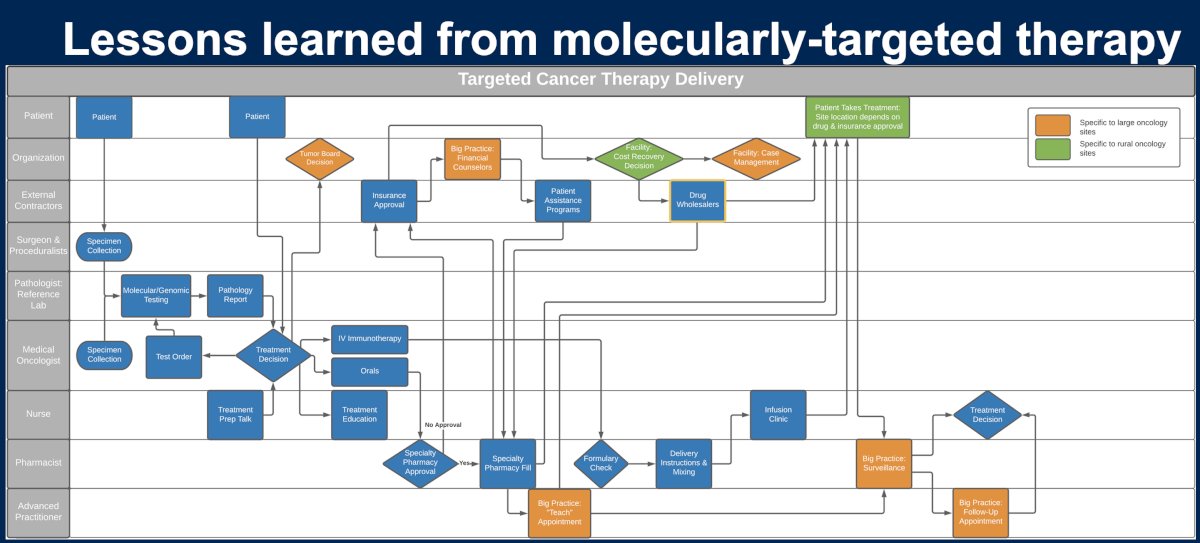
Studies suggest high enthusiasm and commitment on the part of community oncologists to provide molecularly targeted therapy.20 However, the enthusiasm is tempered by questions of sustainability for community oncologists to take sole responsibility to master targeted therapy indications for all malignancies at all stages. Targeted therapy adoption is most frequent and consistent for agents with the greatest survival benefit.22 Practices/health systems in which pathologists take a primary role in ordering molecular testing have been demonstrated to exhibit consistent and timely testing execution. Electronic health record (EHR) integration of molecular testing results facilitates implementation, but is rarely possible for all test results for any given practice.23 On-site CME training17 and molecular tumor boards23 can improve clinician comfort with molecular testing and positively impact ordering of and/or molecularly-targeted treatment.
Time and cost represent significant concerns for oncologists in community (especially rural) practice:
- Time
- Delay in results of molecular testing to drive decision-making
- Time of physicians and nurses to coordinate testing, obtain test results
- Cost
- Costs to quality of life for patients if clinicians lack experience in treating unique side effects
- Out of pocket costs for patients
- Variable payor reimbursement for targeted therapies depending on mode of treatment administration
- Up-front costs for drug acquisition
- Additional personnel required to send/receive testing orders, integrate into the EHR
What are lessons learned from ICI therapy? Adoption of ICI therapy has occurred broadly and swiftly by community oncologists, but frequency and timeframe for adoption varies by cancer. More common cancers appear to have been treated more consistently and expediently for more common malignancies. Prescribing novel therapeutics with unique side effect profiles (particularly if requiring additional subspecialty care for co-management) represents a disproportionate burden to oncologists in community oncology practice and the greatest burden to rural oncologists and those not affiliated with larger practice networks.24 Implementation has consistently followed guideline updates.25

What are some potential positive mediators?
- Role-realignment may promote more consistent ordering of molecular testing required for facilitation of targeted therapy
- Standardization of molecular test ordering by pathology is acceptable to pathologists, reduces work of oncologists and lag time for results, and may prompt consideration of targeted therapies for treating clinicians
- Rapid guideline adoption accelerates prescribing behavior for novel therapeutics
- Lead investigators for pivotal trials demonstrate regional influence; thus, steering committees/industry trial design should make efforts to diversify lead investigators in order to indirectly “share the wealth” of knowledge
- Specialized education, molecular tumor boards, and EHR integration promote incremental change in molecular testing and prescribing of novel cancer therapies and can be considered to support community oncologists depending on individual practice resources and needs
Dr. Wulff-Burchfield concluded as follows:
- Currently approved ADCs such as enfortumab vedotin and trastuzumab deruxtecan (for HER2 3+) have cemented the value of direct tumor killing strategies for urothelial carcinoma
- There is significant ongoing work to identify ideal therapeutic combinations, disease stages, treatment sequencing, and patient selection for ADCs.
- Community oncologists face unique clinical, financial, and logistical challenges when integrating novel therapies into practice, which can limit their availability to patients treated in this setting.
- With rapid advancements in urothelial cancer treatment, implementing successful strategies for targeted and ICI therapy (practice role re-alignment, targeted education, peer mentoring) and some unmet needs identified by targeted and ICI therapy (expanding the pool of lead investigators for GU trials) may promote faster, broader adoption of ADCs for urothelial cancer treated by community oncologists.
Presented by: Elizabeth Marie Wulff-Burchfield, MD, Associate Professor, Medical Oncology, University of Kansas Medical Center, Kansas City, Kansas
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Schwartz RS. Paul Ehrlich's magic bullets. N Engl J Med. 2004;350:1079–80.
- Beck A, Goetsch L, Dumontet C, et al. Strategies and challenges for the next generation of antibody-drug conjugates. Nat Rev Drug Discov. 2017; 16:315-37.
- Yu EY, Petrylak DP, O'Donnell PH, et al. Enfortumab vedotin after PD-1 or PD-L1 inhibitors in cisplatin-ineligible patients with advanced urothelial carcinoma (EV201): a multicentre, single-arm, phase 2 trial. Lancet Oncol. 2021; 22:872-82.
- Powles T, Rosenberg JE, Sonpavde GP, et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. N Engl J Med. 2021; 384:1125-35.
- Gerber HP, Sapra P, Loganzo F, et al. Combining antibody-drug conjugates and immune-mediated cancer therapy: What to expect? Biochem Pharmacol. 2016; 102:1-6.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024; 390:875-88.
- Loriot Y, Petrylak DP, Rezazadeh Kalebasty A, et al. TROPHY-U-01, a phase II open-label study of sacituzumab govitecan in patients with metastatic urothelial carcinoma progressing after platinum-based chemotherapy and checkpoint inhibitors: updated safety and efficacy outcomes. Ann Oncol. 2024; 35:392-401.
- Grivas P, Powles TB, Vulsteke C, et al. LBA9 TROPiCS-04, a randomized phase III study of sacituzumab govitecan (SG) vs chemotherapy (CT) in pretreated advanced urothelial carcinoma (aUC): Overall survival (OS) and safety analysis. Annal Oncol. 2024; 35:S1505-7.
- Li BT, Meric-Bernstam F, Bardia A, et al. Trastuzumab deruxtecan in patients with solid tumours harbouring specific activating HER2 mutations (DESTINY-PanTumor01): an international, phase 2 study. Lancet Oncol. 2024; 25:707-19.
- Meric-Bernstam F, Makker V, Oaknin A, et al: Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial. J Clin Oncol. 2024; 42:47-58.
- Sheng X, Wang L, He Z, et al. Efficacy and Safety of Disitamab Vedotin in Patients With Human Epidermal Growth Factor Receptor 2–Positive Locally Advanced or Metastatic Urothelial Carcinoma: A Combined Analysis of Two Phase II Clinical Trials. J Clin Oncol. 2023; 42:1391-402.
- Unger JM, Vaidya R, Hershman DL, et al. Systematic Review and Meta-Analysis of the Magnitude of Structural, Clinical, and Physician and Patient Barriers to Cancer Clinical Trial Participation. J Natl Cancer Inst. 2019; 111:245-55.
- Vandergrift JL, Gray BM, Barnhart BJ, et al: Opportunities for Maintenance of Certification to Better Reflect Scope of Practice Among Medical Oncologists. JCO Oncol Pract. 2020; 16:e641-8.
- Agha L, Molitor D. The Local Influence of Pioneer Investigators on Technology Adoption: Evidence from New Cancer Drugs. Rev Econ Stat. 2018; 100:29-44.
- Murthy VH, Krumholz HM, Gross CP. Participation in cancer clinical trials: race-, sex-, and age-based disparities. JAMA. 2004; 291:2720-6.
- Kuderer NM, Burton KA, Blau S, et al. Comparison of 2 Commercially Available Next-Generation Sequencing Platforms in Oncology. JAMA Oncol. 2017; 3:996-8.
- Levit LA, Kim ES, McAneny BL, et al: Implementing Precision Medicine in Community-Based Oncology Programs: Three Models. J Oncol Pract. 2019; 15:325-9.
- Six Challenges Facing Community Oncology Practices, Administrative ease, 2024.
- Vyas H. Community Oncology Is at a Tipping Point Thanks to Consolidation, Policy Problems, 2025.
- Ellis SD, Brooks JV, Birken SA, et al. Determinants of targeted cancer therapy use in community oncology practice: a qualitative study using the Theoretical Domains Framework and Rummler-Brache process mapping. Implement Sci Commun. 2023; 4:66. 2023
- Carroll CE, Landrum MB, Wright AA, et al. Adoption of Innovative Therapies Across Oncology Practices-Evidence From Immunotherapy. JAMA Oncol 2023; 9:324-33.
- Keating NL, Huskamp HA, Schrag D, et al. Diffusion of Bevacizumab Across Oncology Practices: An Observational Study. Med Care. 2018; 56:69-77.
- Gottesman O, Kuivaniemi H, Tromp G, et al. The Electronic Medical Records and Genomics (eMERGE) Network: past, present, and future. Genet Med. 2013; 15:761-71.
- Centers AoCC: Immuno-oncology in 2021: committed to the cutting edge of care, Immuno-Oncology Institute, 2021.
- Winzeler-Cotton A, Subramanian A, Kane K, et al: Rapid adoption of immunotherapy in community health systems, associated with changing treatment guidelines. J Clin Oncol. 2022; 40:e18610.