(UroToday.com) The 2025 ASCO annual meeting featured a urothelial carcinoma oral abstract session and a presentation by Dr. Thomas Powles discussing circulating tumor DNA in patients with muscle invasive bladder cancer who received perioperative durvalumab in NIAGARA. In the phase 3 NIAGARA trial of patients with cisplatin-eligible muscle invasive bladder cancer, the addition of perioperative durvalumab to neoadjuvant chemotherapy demonstrated a statistically significant and clinically meaningful improvement in event-free survival and overall survival compared with neoadjuvant chemotherapy alone, and a 10% higher pathological complete response rate, with a manageable safety profile and no impact on the feasibility of surgery.1 Given these results, perioperative durvalumab + neoadjuvant chemotherapy was approved for use in muscle invasive bladder cancer by the US FDA on March 28, 2025. At the 2025 ASCO annual meeting, Dr. Powles reported a planned exploratory analysis of ctDNA and association with clinical outcomes from NIAGARA.
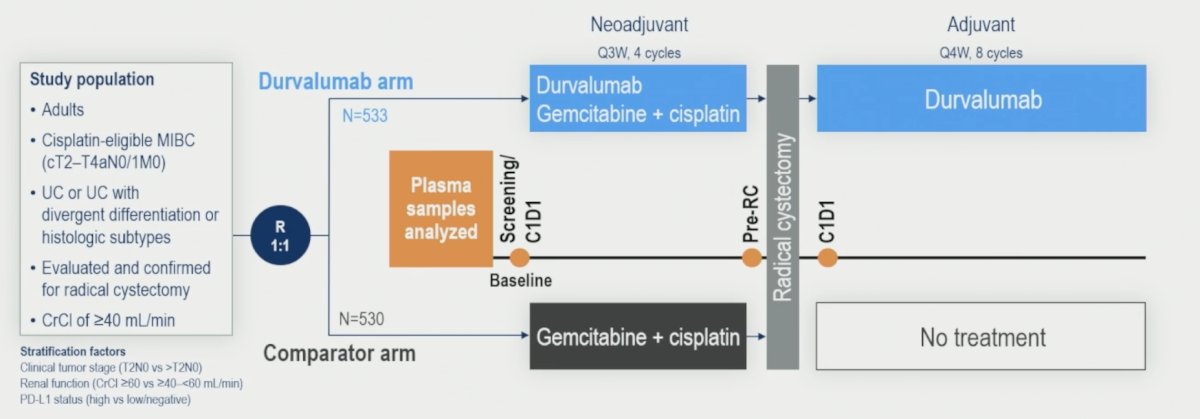
NIAGARA enrolled cisplatin-eligible patients with muscle invasive bladder cancer (cT2-T4aN0/1M0) planned for radical cystectomy. Patients were randomized 1:1 to receive either neoadjuvant durvalumab (1500 mg IV every 3 weeks) and neoadjuvant chemotherapy (cisplatin + gemcitabine IV every 3 weeks) for 4 cycles followed by radical cystectomy, then adjuvant durvalumab monotherapy (1500 mg IV every 4 weeks) for 8 cycles (durvalumab arm), or neoadjuvant chemotherapy followed by radical cystectomy alone (comparator arm). Dual primary endpoints were pathological complete response and event-free survival, with disease-free survival as a secondary endpoint. Plasma ctDNA was assessed using the Signatera personalized, tumor-informed molecular residual disease assay. ctDNA was assessed at baseline (screening or neoadjuvant C1D1, n = 460), after neoadjuvant treatment prior to radical cystectomy (pre-radical cystectomy, n = 422), and at C1D1 of the adjuvant phase (post-radical cystectomy, n = 345):
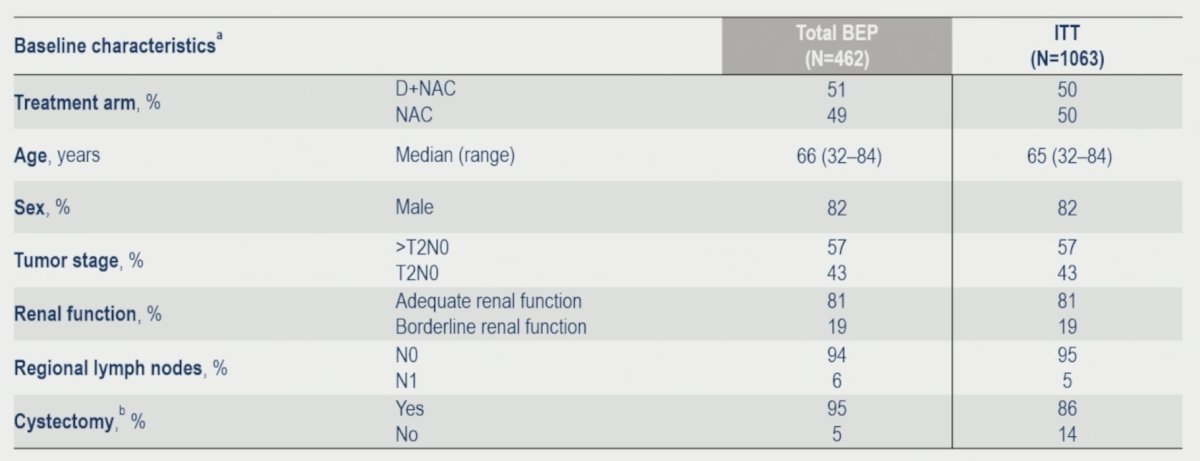
Of 1,063 randomized patients, 462 comprised the biomarker-evaluable population (237 durvalumab arm; 225 comparator arm), and patient characteristics were similar to the ITT population:
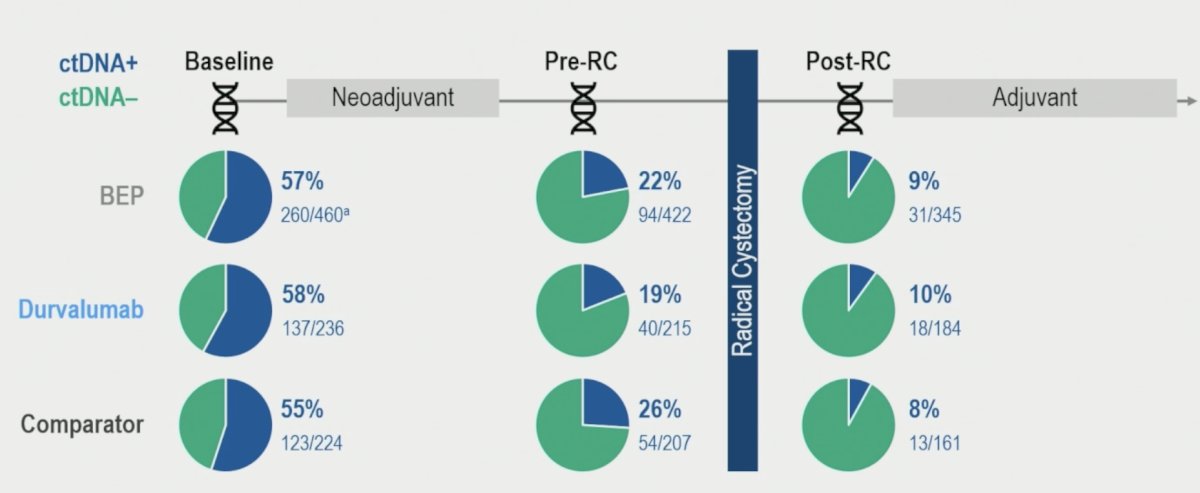
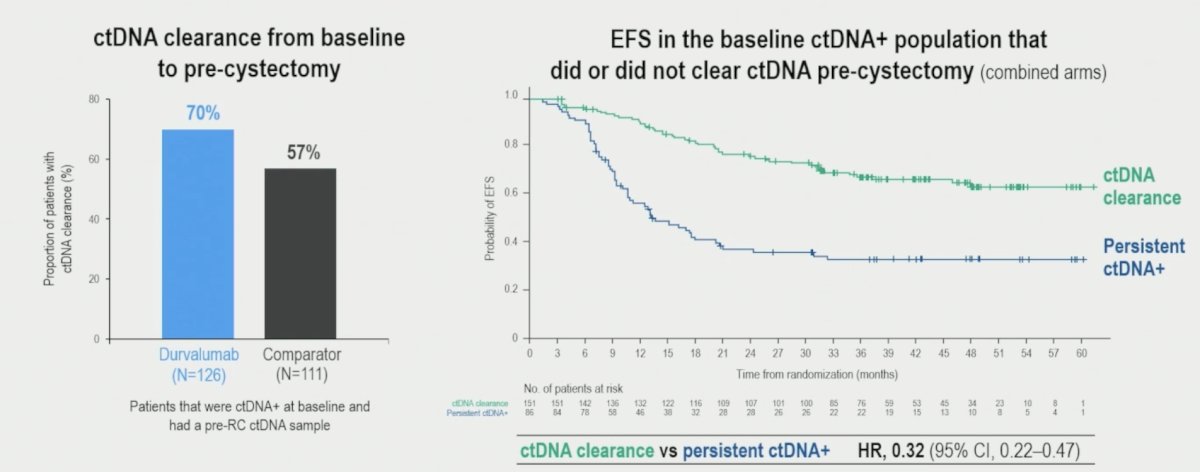
Overall, the ctDNA+ rate at baseline was 57% (260/460) and decreased to 22% (94/422) after neoadjuvant treatment at pre-radical cystectomy. ctDNA clearance rates from baseline to pre-radical cystectomy were 39% in the durvalumab arm and 29% in the comparator arm. Overall ctDNA+ rate post-radical cystectomy was 9% (31/345):
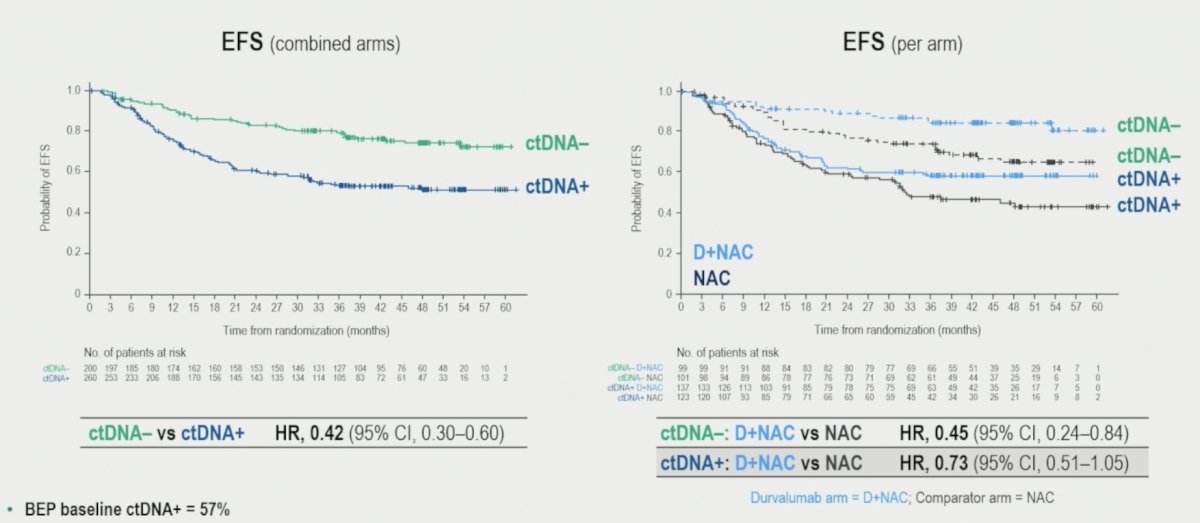
The event-free survival benefit in the durvalumab arm versus the comparator arm was observed in both the baseline ctDNA+ and ctDNA− groups:
Additionally, ctDNA clearance was higher in the durvalumab arms and prognostic for event free survival (HR 0.32, 95% CI 0.22-0.47):
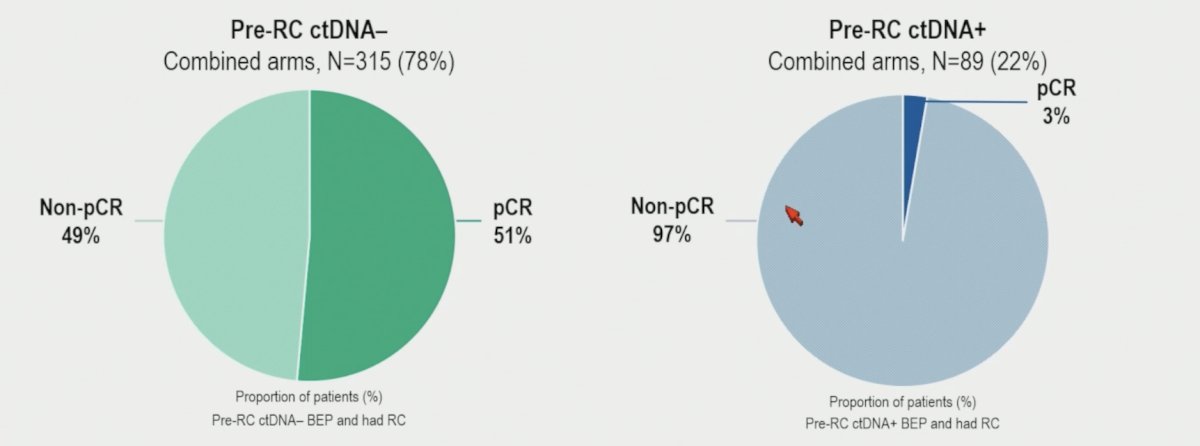
Pre-radical cystectomy ctDNA- status was not associated with pathological complete response, however, ctDNA+ status was highly correlated with non-pathological complete response:
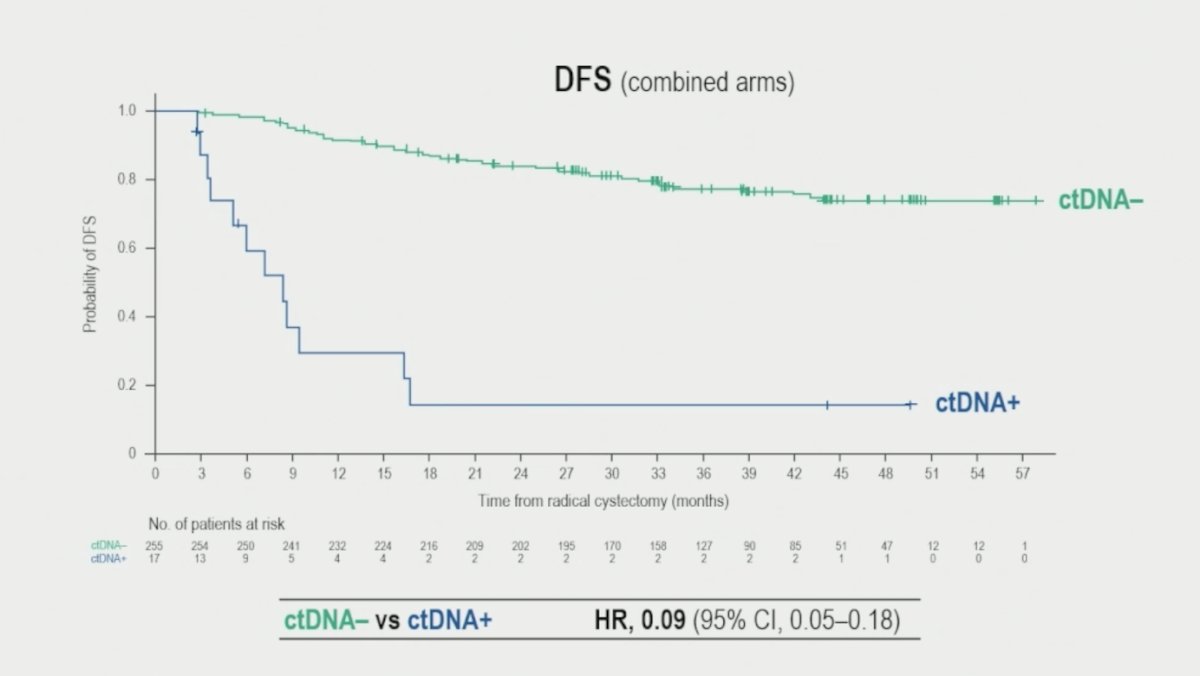
Furthermore, post-radical cystectomy, ctDNA detection was highly prognostic for disease free survival (HR 0.09, 95% CI 0.05-0.18):
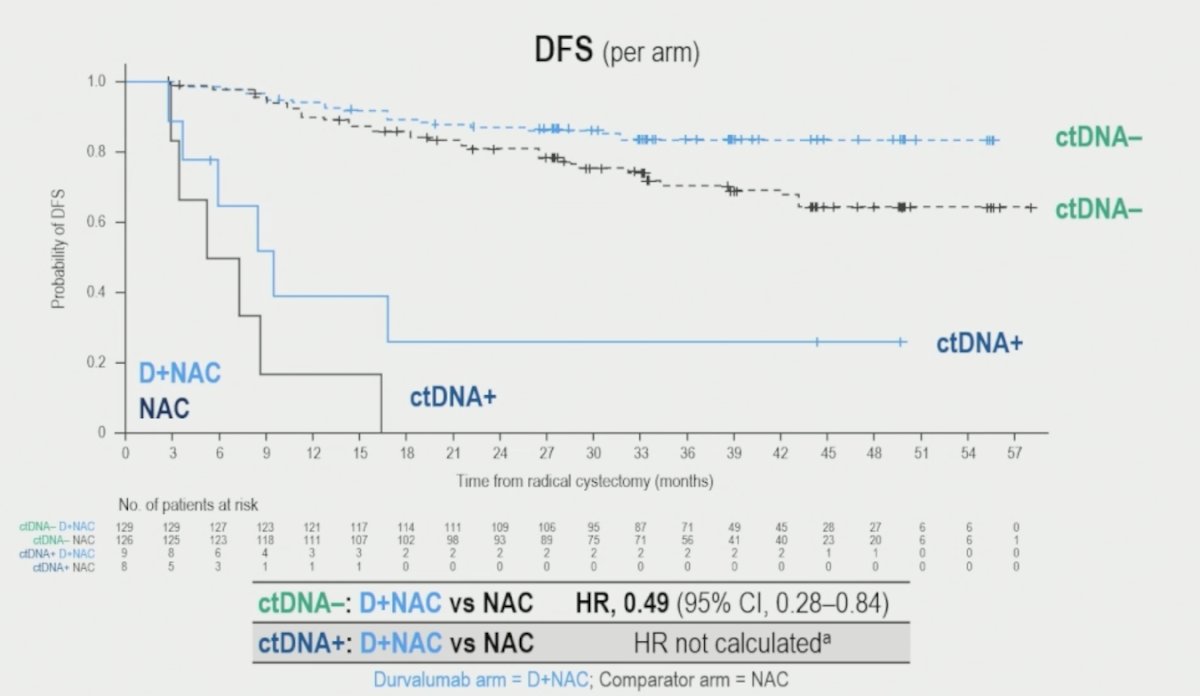
Perioperative durvalumab + neoadjuvant chemotherapy provided a disease free survival benefit to patients with ctDNA- status (HR 0.49, 95% CI 0.28-0.84), however, there was minimal benefit, if any, to those with ctDNA+ status:
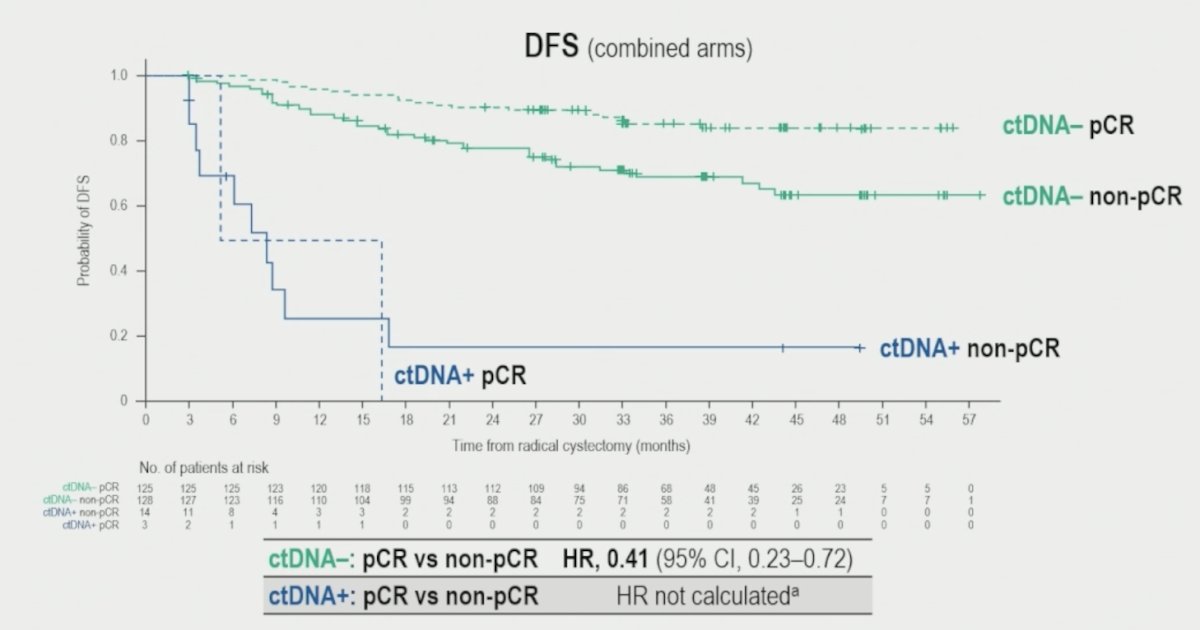
In the ctDNA- population, patients with pathological complete response had a better disease free survival prognosis (HR 0.41, 95% 0.23-0.72):
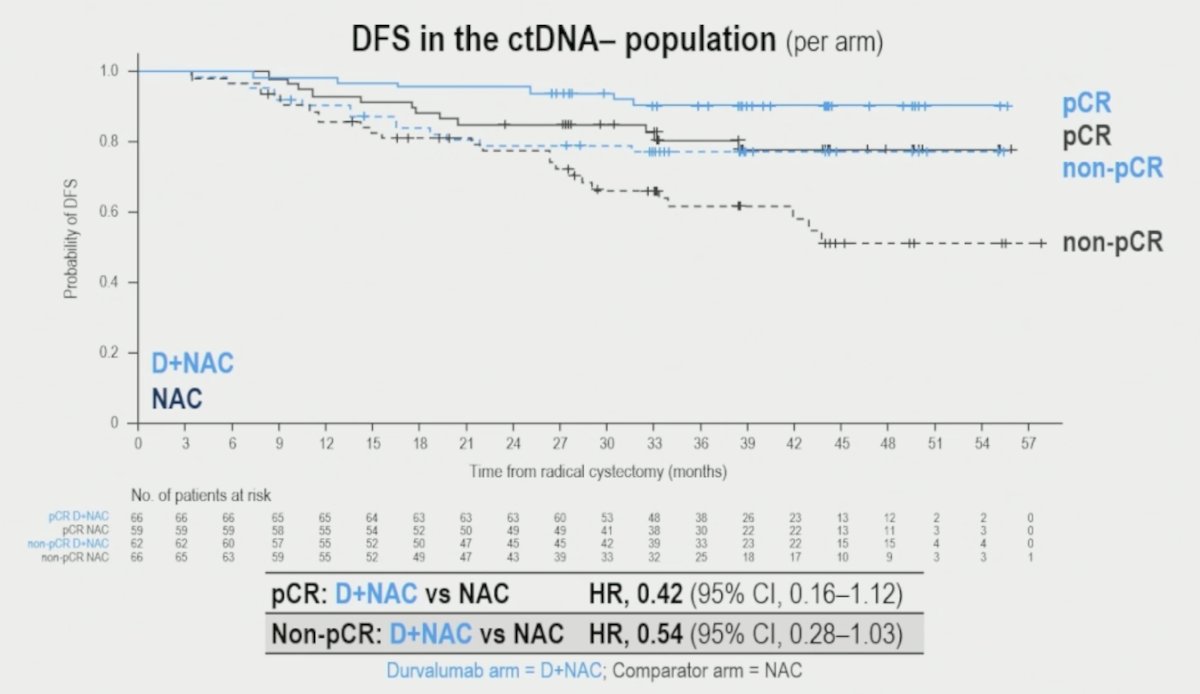
Finally, patients with ctDNA- status, with (HR 0.42, 95% CI 0.16-1.12) or without (HR 0.54, 95% CI 0.28-1.03) pathological complete response, benefited from perioperative durvalumab + neoadjuvant chemotherapy:
Dr. Powles concluded his presentation discussing circulating tumor DNA in patients with muscle invasive bladder cancer who received perioperative durvalumab in NIAGARA with the following take home points:
- Using the Signatera assay, 57% of patients had ctDNA+ status at baseline, dropping to 22% after neoadjuvant treatment, and 9% after cystectomy in the total biomarker evaluable population
- ctDNA status was highly prognostic at baseline, and before and after cystectomy:
- Event free survival was improved for patients with baseline ctDNA- versus ctDNA+ status (HR 0.42)
- Event free survival was also improved with ctDNA clearance versus persistently positive after neoadjuvant treatment (HR 0.32)
- Disease free survival was improved for patients with post-cystectomy ctDNA- versus ctDNA+ (HR 0.09)
- ctDNA clearance rate after neoadjuvant treatment was 13% higher for patients in the durvalumab arm versus comparator arm
- ctDNA+ status pre-cystectomy was associated with a very low likelihood of pathological complete response
- 91% of patients were ctDNA- after cystectomy, and, in this population, perioperative durvalumab + neoadjuvant chemotherapy, provided disease free survival benefit irrespective of pathological complete response
- Perioperative durvalumab + neoadjuvant chemotherapy provided event free survival benefit irrespective of baseline ctDNA status
- These analyses from NIAGARA highlight the potential utility of ctDNA as a prognostic biomarker and further support the role of perioperative durvalumab in muscle invasive bladder cancer
Presented by: Thomas Powles, MD, Barts Cancer Institute, Experimental Cancer Medicine Centre, Queen Mary University of London, St Bartholomew’s Hospital, London, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References: