(UroToday.com) The 2023 American Society of Clinical Oncology (ASCO) annual meeting held in Chicago, IL between June 2nd and June 6th was host to a prostate, testicular, and penile cancers oral abstract session. Professor Karim Fizazi presented updated results of TALAPRO-2, concurrently published in The Lancet today, which is a phase 3 randomized clinical trial evaluating talazoparib + enzalutamide versus placebo + enzalutamide as 1st line treatment for metastatic castrate resistant prostate cancer (mCRPC) patients harboring homologous recombination repair (HRR) gene alterations.
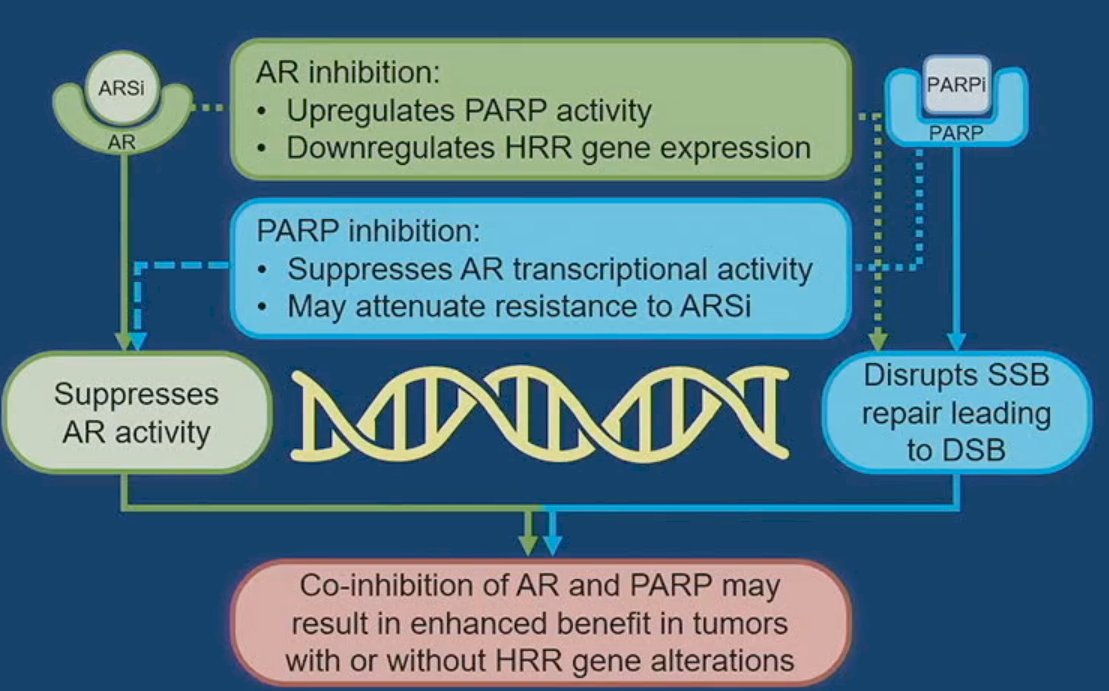
Enzalutamide monotherapy is a current standard of care approach for the 1st line treatment of mCRPC patients.1 In TALAPRO-1, talazoparib monotherapy (1 mg/day) showed durable antitumor activity and manageable safety in patients with heavily pre-treated mCRPC with HRR gene alterations.2 It has been suggested that poly (adenosine diphosphate-ribose) polymerase (PARP) inhibitors, such as talazoparib, may have a synergistic mechanism of action with androgen receptor signaling inhibitors (ARSIs). PARP inhibitors upregulate androgen receptor signaling, enhancing ARSI activity. Conversely, ARSIs inhibit the transcription of some HRR genes, inducing an HRR deficiency-like state, potentiating PARPi activity.3-5
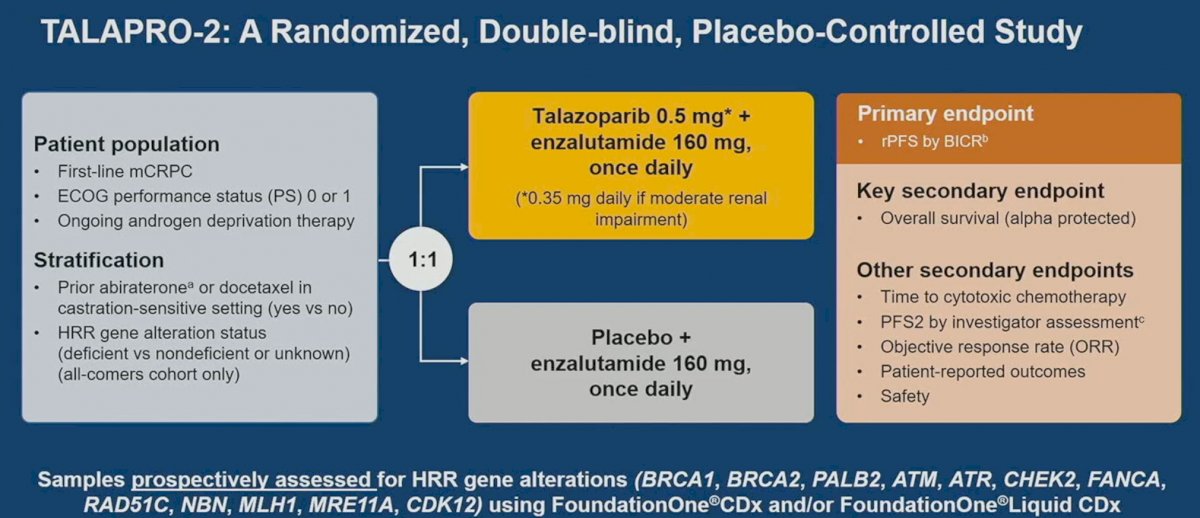
TALAPRO-2 is a phase III randomized, double-blind, placebo-controlled trial that evaluated the combination of talazoparib and enzalutamide in the 1st line treatment setting for mCRPC patients. Patients were randomized 1:1 to talazoparib 0.5 mg once daily (reduced dose from standard of 1.0 mg) plus enzalutamide 160 mg once daily versus placebo + enzalutamide. Prior use of docetaxel and abiraterone in the mHSPC, but not mCRPC setting, was permitted. No prior use of an androgen receptor inhibitor was permitted. Similar to PROpel, this was a biomarker unselected cohort of ‘all comers’, although randomization was stratified by HRR gene alteration status (deficient versus non-deficient or unknown). The primary endpoint was radiographic progression-free survival (rPFS), assessed via blinded independent central review (BICR). OS was a key secondary endpoint.
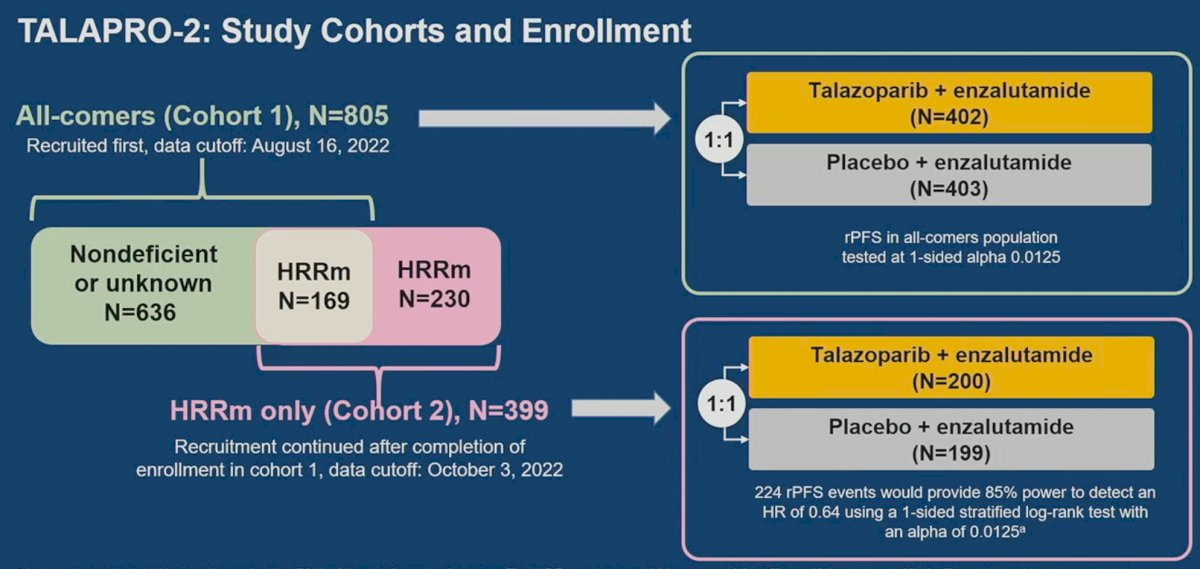
TALAPRO-2 initially recruited the ‘all-comers’ cohort of 805 patients (Cohort 1). Patients within this cohort were randomized to talazoparib + enzalutamide versus placebo + enzalutamide. Analysis of this cohort demonstrated statistically significant improvements in rPFS by BICR with combination talazoparib + enzalutamide (HR: 0.63, 95% CI: 0.51 – 0.78, p<0.001). Next, a further 230 patients with known HRR mutations were recruited, and along with the 169 HRR mutated patients from Cohort 1, formed Cohort 2 (n=399). These 399 patients were randomized in a 1:1 fashion as well to the two treatment arms as demonstrated below:
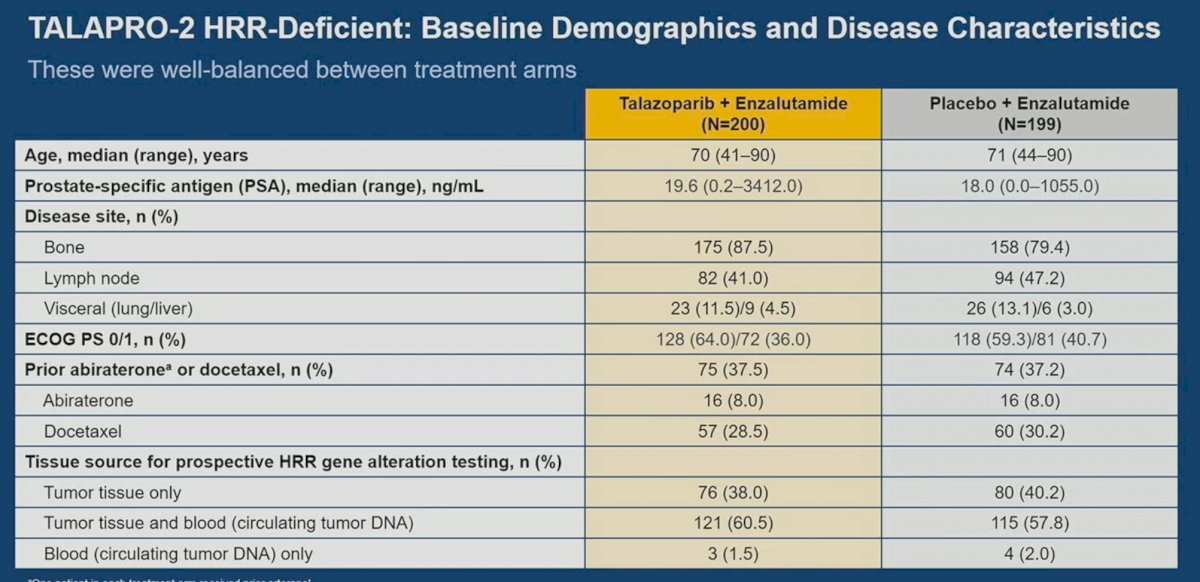
In this report, Dr. Fizazi presented the analysis of Cohort 2. Baseline patient characteristics were well-balanced between the two arms of this cohort. 8% had received prior abiraterone and approximately 30% had received docetaxel. The tissue source for determining HRR mutational status included tumor tissue for over 98% of patients.
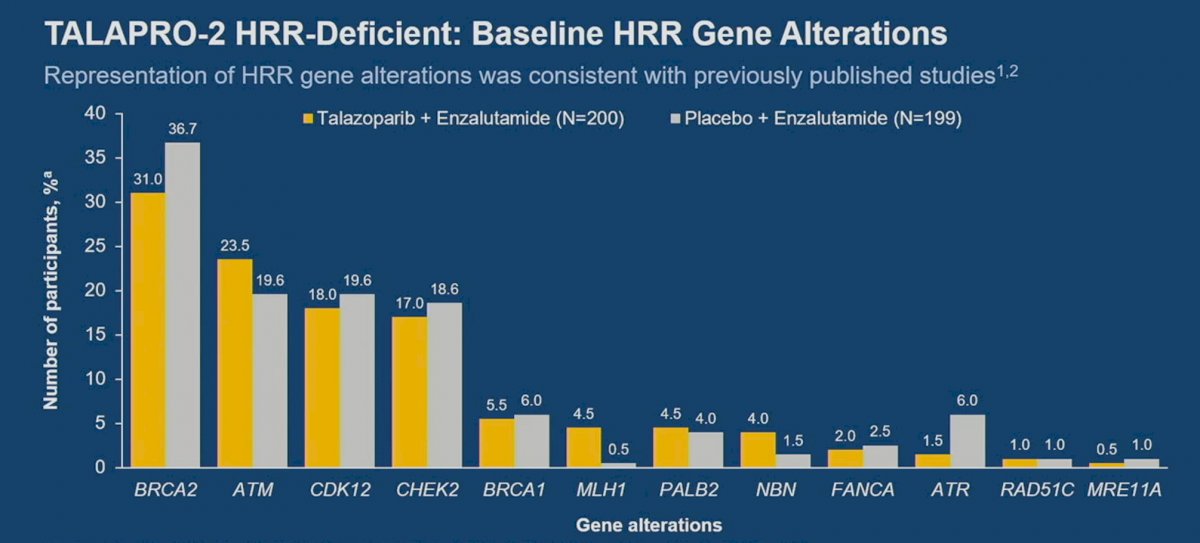
In this HRR mutated cohort, BRCA2 mutations were the most common accounting for about 34% of total mutations, followed by ATM (20-24%), and CDK12 (18-20%).
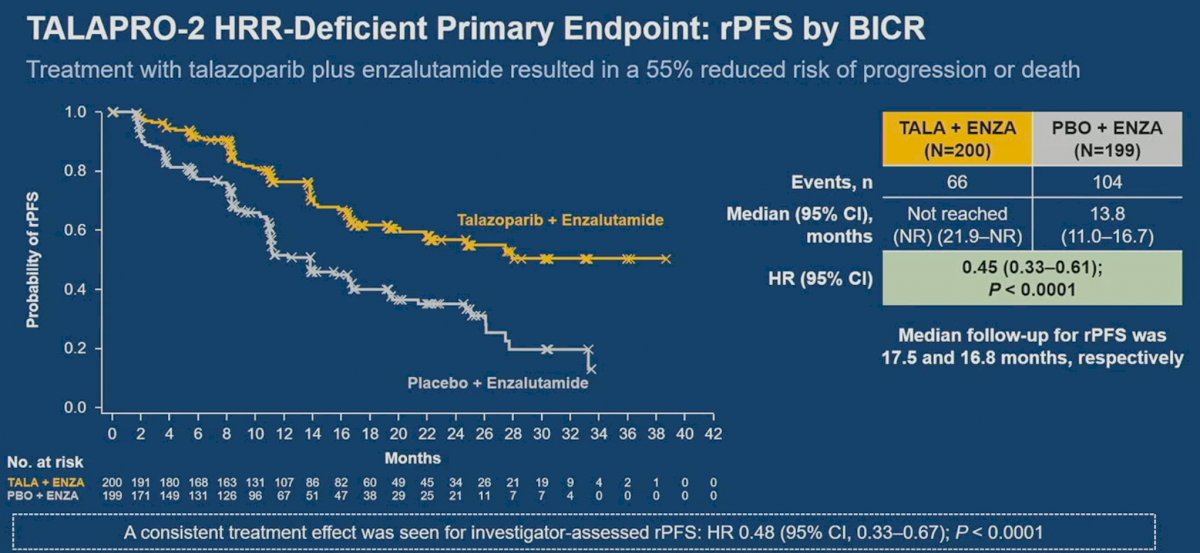
At a median follow-up of 16.8-17.5 months, the combination of talazoparib + enzalutamide was associated with significant improvements in rPFS with a median rPFS not reached in the intervention arm versus 13.8 months in the placebo/enzalutamide arm (HR: 0.45, 95% CI: 0.33 – 0.81, p<0.0001).
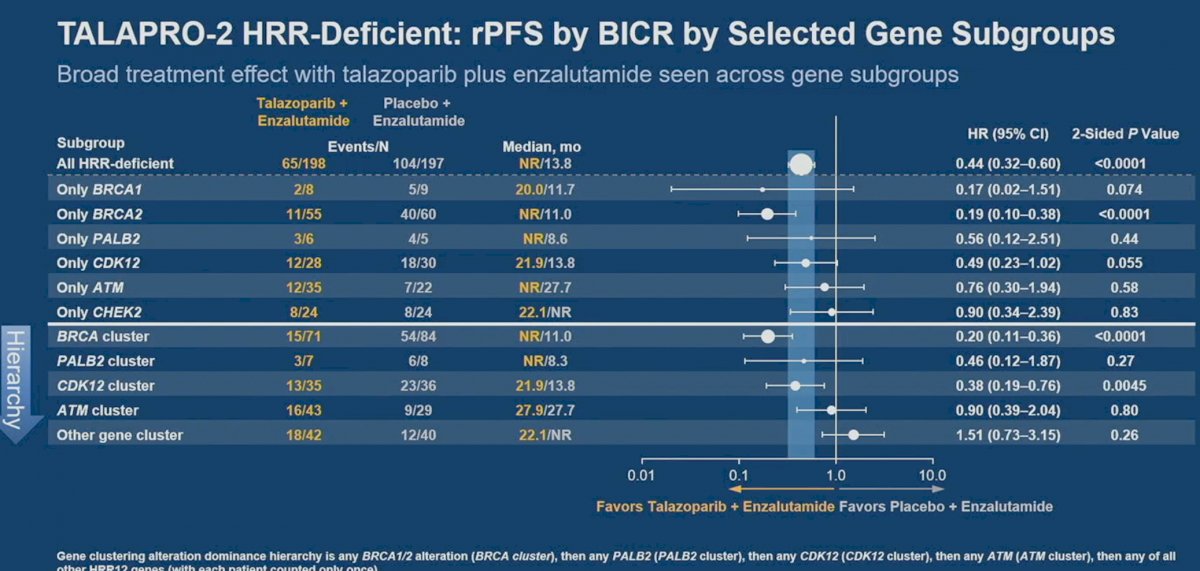
On subgroup analysis, consistent rPFS benefits were observed across the majority of the subgroups. Of note, patients who had received prior abiraterone or docetaxel still derived a significant rPFS benefit from this combination (HR: 0.43, 95% CI: 0.26 – 0.70, p=0.0006). Consistent with the existing literature, BRCA2 patients had the highest magnitude of benefit with this combination approach (HR: 0.20, 95% CI: 0.11-0.36, p<0.0001).
rPFS analysis by select gene subgroups demonstrated that this combination conferred benefits in the BRCA1 mutated patients, as well, with the upper boundary of the confidence interval crossing the null effect of 1 secondary to the small sample size (9 patients with 5 events). Gene cluster analysis demonstrated that rPFS benefits were limited to the BRCA cluster, with no significant rPFS improvements in the PALB2, CDK12, ATM, and other gene clusters.
Overall survival data remains immature (24% maturity overall). There appears to be an early signal for OS benefits in this HRR mutated cohort (HR: 0.69, 95% CI, 0.46 – 1.03, p=0.068).

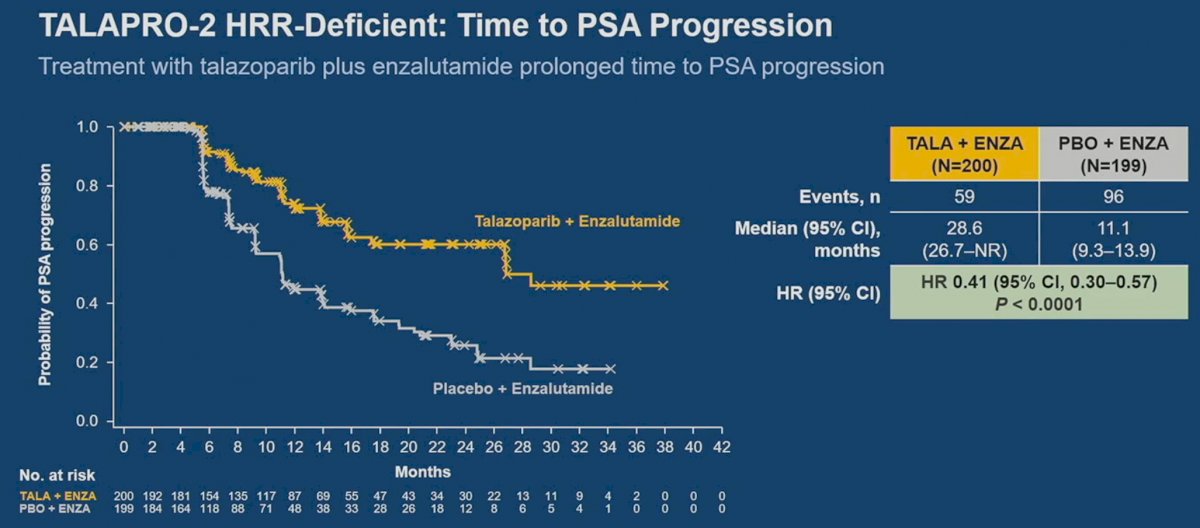
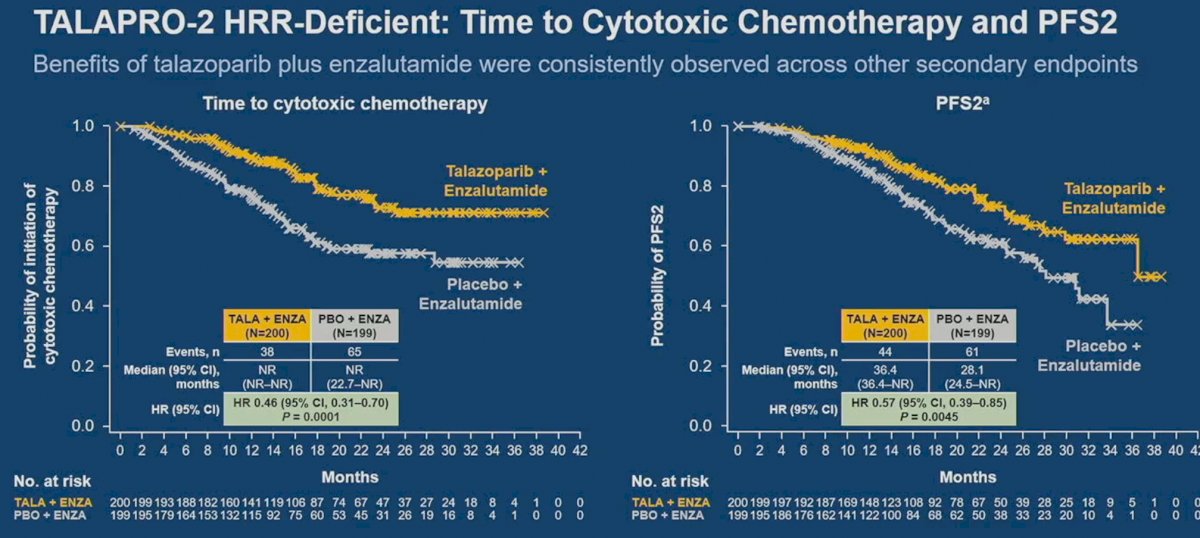
Other secondary endpoints such as time to PSA progression (HR: 0.41, 95% CI: 0.30 – 0.57, p<0.001), time to cytotoxic chemotherapy (HR: 0.46, 95% CI: 0.31 – 0.70, p=0.0001), and time to second progression-free survival (HR: 0.57, 95% CI: 0.39 – 0.85, p=0.0045) favored combination enzalutamide + talazoparib. An objective response rate of 67.1% was observed with combination talazoparib + enzalutamide versus 40% in the placebo/enzalutamide arm.
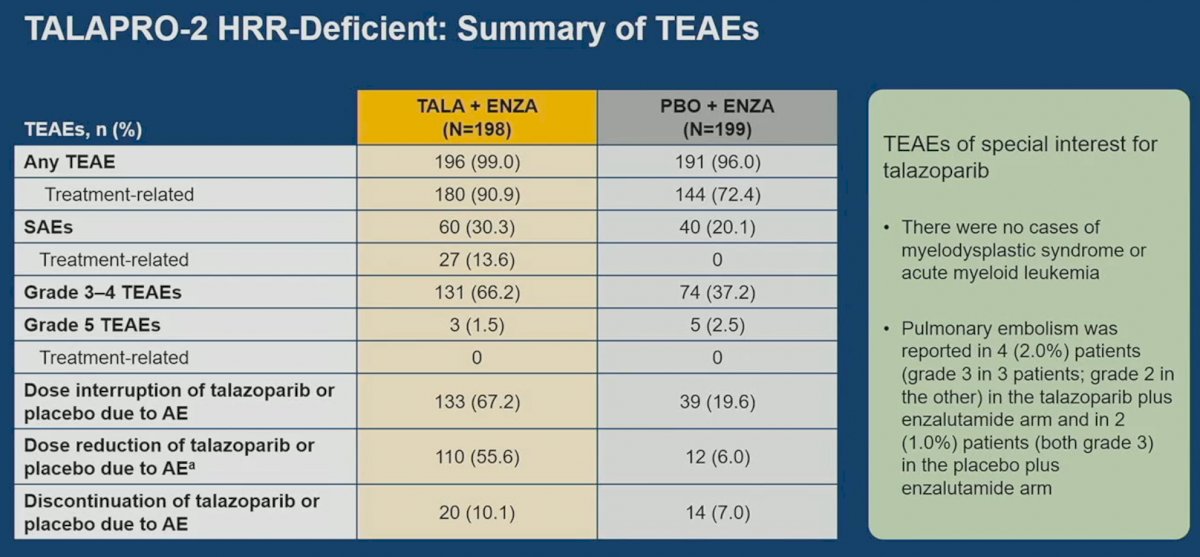
With regards to treatment-emergent adverse events (TEAEs), grade 3 or worse TEAEs were observed in 66% and 37% of patients, respectively. Dose interruptions (67% versus 20%) and dose reductions (56% versus 6%) were more common in the talazoparib + enzalutamide arm. Grade 3 or worse treatment-emergent anemia was observed in 39% and 16% of patients in the intervention and control arms, respectively.

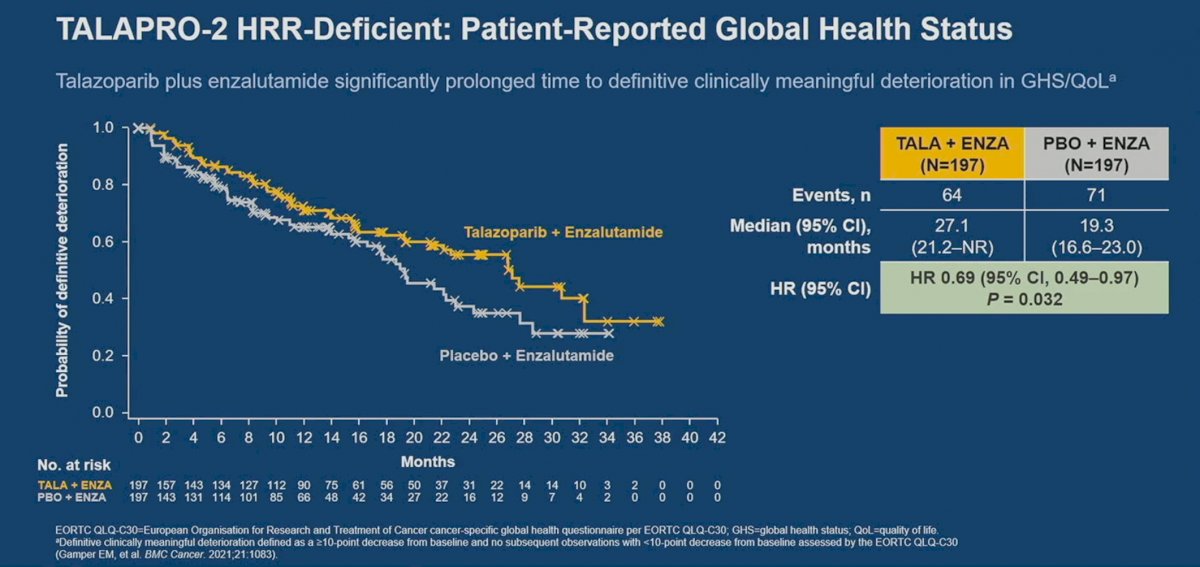
Patient-reported global health status in this cohort favored the intervention arm, with talazoparib + enzalutamide significantly prolonging the time to definitive clinically meaningful deterioration in global health status/quality of life.
Dr. Fizazi concluded as follows:
- In this large, randomized trial involving mCRPC patients with HRR gene alterations, talazoparib plus enzalutamide resulted in a statistically significant and clinically meaningful improvement in rPFS by BICR, compared to placebo plus enzalutamide.
- The rPFS benefit was greater for patients with BRCA alteration (HR: 0.20, 95% CI: 0.11 – 0.36, p <0.0001) compared to those with non-BRCA alterations (HR: 0.68, 95% CI: 0.46 – 1.02, p=0.06).
- Although OS data remains immature, there appears to be a favorable trend towards improved survival for patients with HRR gene alterations (HR: 0.69, 95% CI: 0.46 – 1.03, p=0.068).
- No new safety signals were identified, with treatment-emergent anemia the most common grade 3-4 TEAE
- Time to definitive clinically meaningful deterioration in global health status/quality of life was significantly prolonged with talazoparib plus enzalutamide versus placebo plus enzalutamide.
- Talazoparib in combination with enzalutamide, if approved, has the potential to become a first-line treatment option for patients with mCRPC and HRR gene alterations.
Presented by: Karim Fizazi, MD, PhD, Professor, Department of Medicine, Institut Gustave Roussy, Paris, France
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 2 – Tues, June 6, 2023.
References:
- Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371(5):424-433.
- De Bono JS, Mehra N, Scagliotti GV, et al. Talazoparib monotherapy in metastatic castration-resistant prostate cancer with DNA repair alterations (TALAPRO-1): an open-label, phase 2 trial. Lancet Oncol. 2021;22(9):1250-1264.
- Asim M, Tarish F, Zecchini HI, et al. Synthetic lethality between androgen receptor signalling and the PARP pathway in prostate cancer. Nat Commun 2017; 8: 374.
- Schiewer MJ, Goodwin JF, Han S, et al. Dual roles of PARP-1 promote cancer growth and progression. Cancer Discov 2012; 2: 1134-49.
- Li L, Karanika S, Yang G, et al. Androgen receptor inhibitor-induced “BRCAness” and PARP inhibition are synthetically lethal for castration-resistant prostate cancer. Sci Signal 2017; 10: eaam7479.
- Agarwal N, Azad A, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): a randomised, placebo-controlled, phase 3 trial. The Lancet. 2023.