(UroToday.com) Dr. Pedro Barata provided a nice discussion about novel therapeutic agents for castration resistant prostate cancer.
He focused on two abstracts today (both covered by UroToday):- Abstract 5018: Phase I dose-escalation results of prostate-specific membrane antigen-targeted radionuclide therapy (PSMA-TRT) with alpha-radiolabeled antibody 225Ac-J591 and beta-radioligand 177Lu-PSMA I&T
Presented by: Scott T. Tagawa, MD, FASCO, FACP, MS | Weill Cornell Medicine, Division of Hematology & Medical Oncology, NewYork-Presbyterian Hospital
- Abstract 5019: Final results from phase I study of PSCA-targeted chimeric antigen receptor (CAR) T cells in patients with metastatic castration resistant prostate cancer (mCRPC)
Presented by: Tanya B. Dorff, MD | Department of Medical Oncology & Experimental Therapeutics, City of Hope Comprehensive Cancer Center
He first began by highlighting the progress we have made in the management of mCRPC, Starting with chemotherapy, we have seen the introduction of targeted therapy, novel hormonal agents, and radiopharmaceuticals.

However he notes that remissions remain the exception and not the rule, so there is still room for significant improvement.
They started by first focusing on PSMA (prostate specific membrane antigen), reviewing its structure and function. He again highlighted the fact that it is overexpressed in prostate cancer, particularly in more advanced stage prostate cancer.
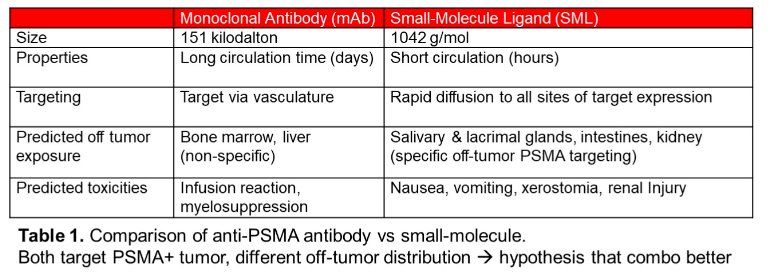
However, PSMA may be targeted by antibodies (mAb) or small molecules (SML), with different kinetics and biodistribution. mAb may have longer circulation time and marrow exposure but have decreased access to luminal PSMA expression (e.g. salivary glands, intestine, kidney). In contrast, SML diffuses to all sites of PSMA expression and then excreted. These differences are summarized below:
When looking at the radionuclide itself, alpha radionuclides emit more energy over shorter range vs beta. Pre-clinical data combining mAb and SML targeting supports synergy, with enhanced uptake and retention of SML.
He then talked about the current status of PSMA based radioligand therapy (RLT), which is currently dominated by 177Lu-PSMA-617. The VISON trial established this as the new SOC for patients with mCRPC who progress on taxases and novel hormonal therapies. But, as seen below, there is a push to move this therapy into earlier stages:
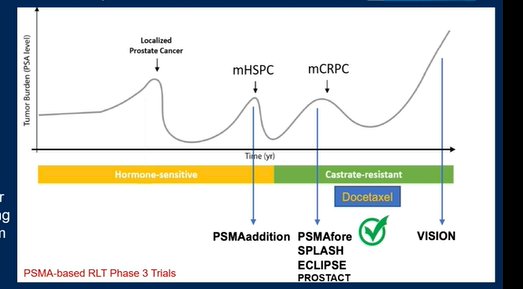
Important phase 3 trials include in the metastatic hormone sensitive space.
As we try to improve outcomes in patients treated with radioligand therapy, one way is to increase synergy with other therapies, including PARP inhibitors, immunotherapy, or an alpha/beta emitter tandem.
Focusing now on tandem therapy with alpha and beta emitters, he did highlight some data about sequencing.
- 177-Lu-PSMA-617 (which is a beta emitter) after Ra-223 (which is an alpha emitter) is safe and effective
- Alpha-based RLT after beta-based RLT also appears to be safe and have continued antitumor activity
He did highlight that there are already some retrospective based analysis looking at the combination of alpha beta tandem therapies, typically 225-Ac-PSMA-617 and 177-Lu-PSMA-617. These few retrospective series with small numbers of patients appeared to show reasonable antitumor effectiveness, including patients previously treated patients with beta-emitter RLT. He man adverse effect appears to be xerostomia.
He delved into Dr. Tagawa’s data and abstract. Theirs was a phase I dose-escalation results of a phase I/II trial investigating combo 225Ac-J591 with 177Lu-PSMA-I&T (aka PNT2002). Eligibility criteria include progressive mCRPC, ≥1 prior AR pathway inhibitor (ARPI), prior chemo (or unfit/refuse), ≥1 lesion with SUVmax >liver. Many of these patients were heavily pretreated.
As of 5/1/2023, 5 pts remain on study, including 1 with an undetectable PSA at 13 months after 2 cycles of treatment. With follow up ongoing, 17 (94%) with PSA decline, 11 (61%) with PSA50. PSA response is summarized in the figures below:

The safety profile was well tolerated – thrombocytopenia was found to be the dose limiting toxicity. Xerostomia and nausea were the most common side effects.
His main take home points for this trial were that there is good rationale to combine alpha with beta based RLT in PSMA+ selected cohorts. There is evidence of preliminary activity in a heavily pretreated population but there are stoma and thrombocytopenia are frequent and can be a limiting factor. He notes that there is relatively short followup, thereby limiting the ability to reach any clinically meaningful endpoint such as rPFS or OS.
- The key next steps are to clarify the role of tandem therapy in RLT-naïve vs. progressors on beta-based RLT.
He then at this point switched gears to the emergence of CAR-T therapy. As background, he notes that cancer progression results in increased genomic alterations and increase in neoantigens. CAR-T cells are “self” T cells engineered to target a specific antigen. they are highly specialized and highly personalized treatment available only in a few centers with specialized expertise in cellular therapies. they have had significant success in hematologic malignancies.
CAR-T clinical experience in prostate cancer is relatively new. There are a few sites that are actively working on this and have published on it. You highlighted some of these groups in the slide below:

He then focused on Dr. Dorff’s work, in which they chose PSCA as the target neoantigen. Prostate Stem Cell Antigen (PSCA) is highly expressed on the surface membrane in mCRPC but has limited expression on normal tissues, making it an ideal target for therapy.
Eligible patients include adult patients with metastatic castration resistant prostate cancer whose cancer has progressed after at least one androgen receptor targeted agent. Prior taxane chemotherapy was allowed but not required; there was no limit on prior lines of therapy. CAR T cells were manufactured at City of Hope’s cGMP facility. In this first in human phase one trial they treated 14 patients. It had different stages associated with dose escalation. The primary endpoints were both safety as well as persistence of car T cells through day 28 and disease response.
The 3 stages of the study are summarized nicely below:
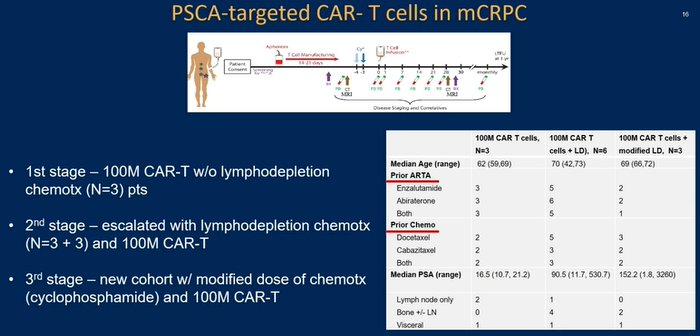
Unfortunately, no objective responses were noted. But two patients did have clinical improvement, including a reduction in size and number of liver mets. Cystitis was identified as the dose limiting toxicity (as there is some PSCA expression in the bladder). Finally, the use of lymphodepletion chemo was associated with better expansion and persistence of the CAR-T cells.
His lessons learned from CAR-T in prostate cancer are the following:
- PSCA appears to be a good target for metastatic castration resistant prostate cancer
- Lymphodepletion chemotherapy process allows expansion and persistence of CAR-T cells but it can contribute to dose limiting toxicities such as cystitis.
- safety is still a concern for CAR-T technology. it is not enough to have a good target and likely success depends on multiple factors.
He does not feel that CAR-T therapy for prostate cancer is ready for prime time, but it may have promising anti cancer effect which justifies efforts to overcome these obstacles.
Presented by: Pedro C. Barata, MD, MSc | University Hospitals Seidman Cancer Center, Cleveland, OH
Written by: Thenappan (Thenu) Chandrasekar, MD – Urologic Oncologist, Associate Professor of Urology, University of California, Davis, @tchandra_uromd @UCDavisUrology on Twitter during the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 2 – Tues, June 6, 2023.