(UroToday.com) The 2023 American Society of Clinical Oncology (ASCO) annual meeting held in Chicago, IL between June 2nd and June 6th was host to a kidney and bladder cancers poster session. Dr. Shuchi Gulati, MD, MS, presented results of a subgroup analysis from the EVEREST trial (SWOG S0931) evaluating adjuvant everolimus in patients with localized non-clear cell renal cell carcinoma (nccRCC).
The EVEREST trial was a phase 3, double-blind, placebo-controlled trial that randomized 1,545 patients in a 1:1 fashion to 54 weeks of everolimus (10 mg daily), an mTOR inhibitor, or placebo within 12 weeks of radical or partial nephrectomy. This trial included patients with treatment-naïve, non-metastatic, fully-resected RCC at intermediate high- (pT1 G3-4 N0 to pT3a G1-2 N0) or very high-risk disease (pT3a G3-4 to pT4 G-any or N+). This trial failed to meet its primary endpoint with disease-free survival (DFS) and overall survival (OS) hazard ratios (HR) of 0.85 (95% CI: 0.71 – 1.00) and 0.90 (95% CI: 0.71 – 1.13), respectively.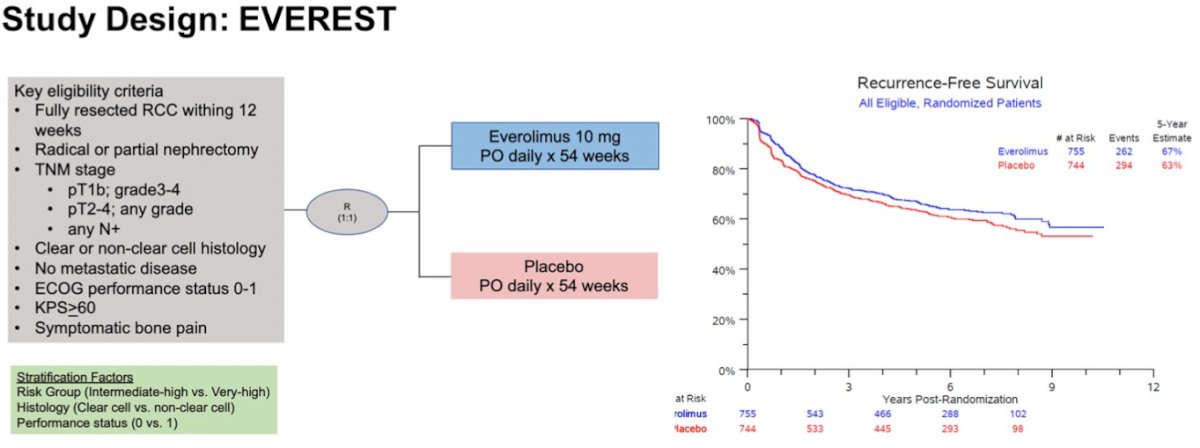
However, there is evidence that everolimus may have activity in patients with chromophobe and/or papillary RCC.1,2 As such, the authors sought to evaluate the efficacy of everolimus within these non-clear cell subsets of EVEREST.
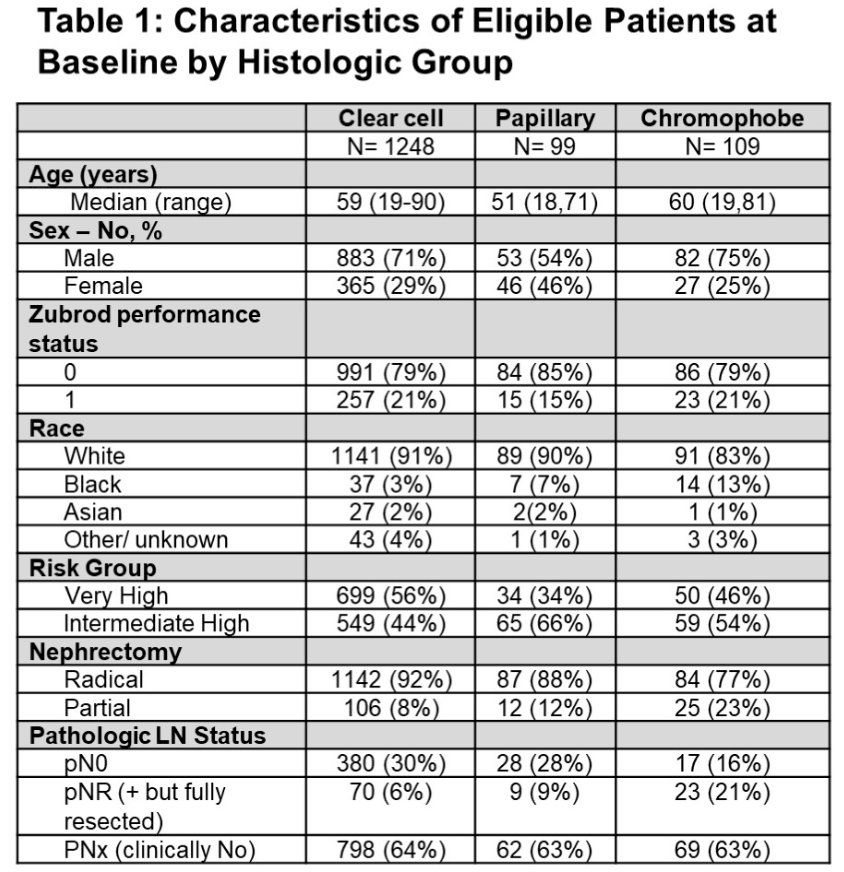
This analysis included a total of 99 patients with chromophobe RCC and 109 with papillary RCC (Type 1: 16; Type 2: 37; Not otherwise specified: 56). The median follow-up was 6.3 years. Baseline patient characteristics were well-balanced between the two groups, consistent with the randomization technique. 34% of patients in the chromophobe RCC subgroup and 46% of those in the papillary RCC subgroup had very high-risk disease.
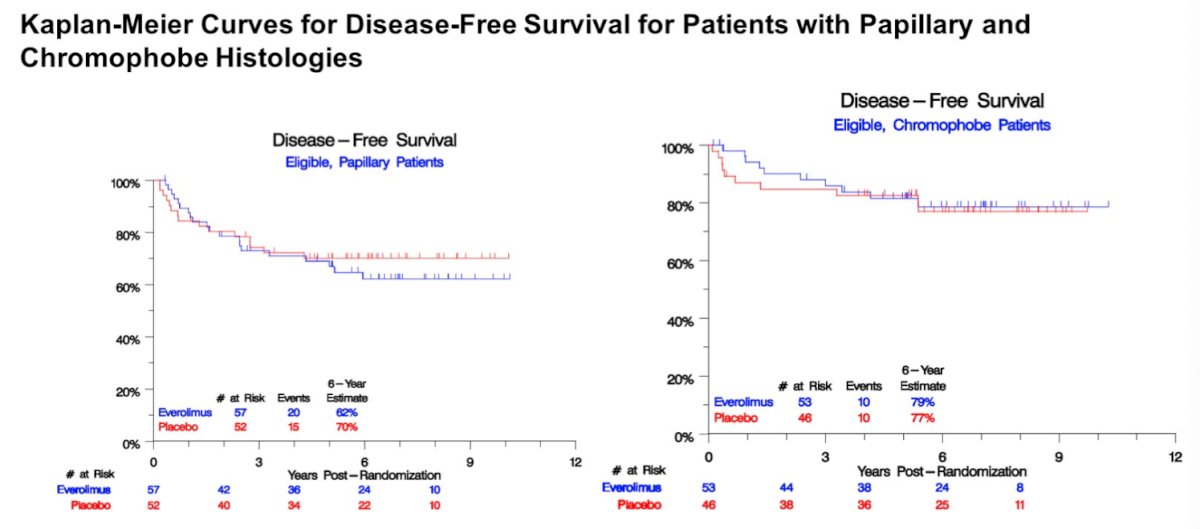
Fewer patients completed all 54 weeks of everolimus in each subgroup compared to placebo (49% versus 74% in the chromophobe subgroup and 46% versus 71% in the papillary subgroup). Efficacy analyses failed to demonstrate a DFS benefit to the use of everolimus in this setting in both the chromophobe (HR: 0.89, 95% CI: 0.37 – 2.13, p=0.79) and the papillary subgroups (HR: 1.19, 95% CI: 0.61 – 2.33, p=0.61). No OS benefits were seen with everolimus use in either subgroup (HRs: 0.93 and 1.47, respectively).
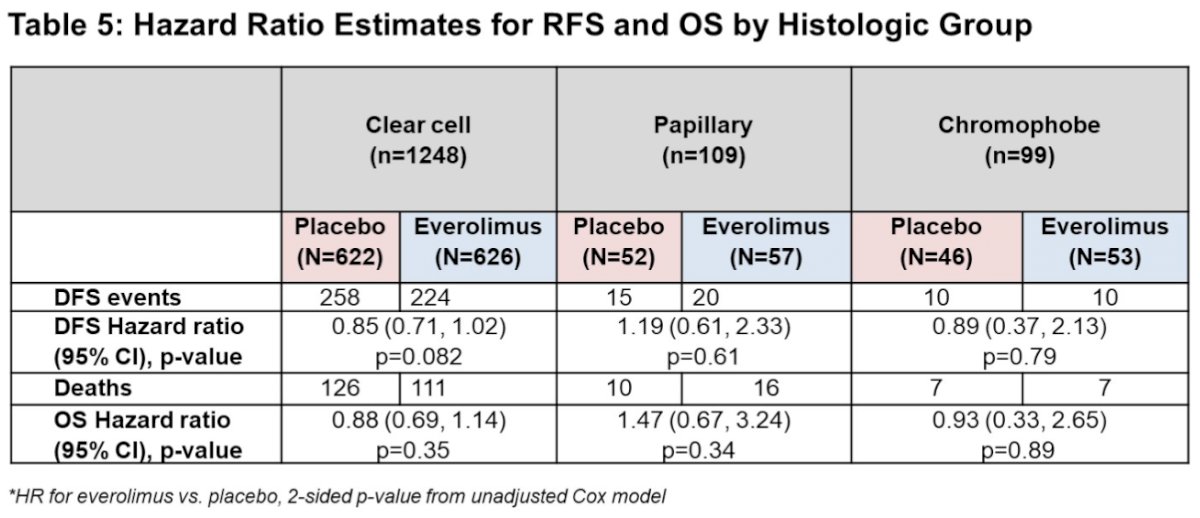
The investigators concluded that patients with non-clear cell histology accounted for a significant proportion (~13%) of the S0931 cohort. The everolimus estimated hazard ratios for DFS and OS in the chromophobe RCC subset were consistent with the overall trial results; however, those same modest HR benefits were not observed in the papillary RCC subgroup. These results are in contrast to prior reports of mTOR inhibitor activity in this subtype. Although inferences are limited by sample size and wide confidence intervals, this is the largest experience in chromophobe or papillary RCC subgroups among any adjuvant trials presented to date.
Presented by: Shuchi Gulati, MD, MS, Assistant Professor, Division of Hematology and Oncology, Department of Internal Medicine, University of California, Davis, CA
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 2 – Tues, June 6, 2023.
References:
- Tannir NM, Jonasch E, Albiges L, et al. Everolimus Versus Sunitinib Prospective Evaluation in Metastatic Non-Clear Cell Renal Cell Carcinoma (ESPN): A Randomized Multicenter Phase 2 Trial. Eur Urol 2016;69(5):866-74.
- Escudier B, Molinie V, Bracarda S, et al. Open-label phase 2 trial of first-line everolimus monotherapy in patients with papillary metastatic renal cell carcinoma: RAPTOR final analysis. Eur J Cancer 2016;69:226-235.