(UroToday.com) Dr. Benjamin Garmezy presents a review of 3 abstracts and puts it in the context of the power of patients’ experiences to inform therapeutic decisions.
The abstracts he reviews are the following:
- Abstract 4515: Estimated net benefit of avelumab (AVE) + best supportive care (BSC) vs BSC alone for patients (pts) with advanced urothelial carcinoma (aUC) using a quality-adjusted time without cancer symptoms or toxicity (Q-TWiST) analysis
- Presented by: Thomas Powles, MD | Barts Cancer Institute, Experimental Cancer Medicine Centre, Queen Mary University of London, St. Bartholomew's Hospital
- Abstract 4516: Long-term safety of avelumab first-line (1L) maintenance for advanced urothelial carcinoma (aUC) in the JAVELIN Bladder 100 trial
- Presented by: Joaquim Bellmunt, MD, PhD | Dana-Farber Cancer Institute, Harvard Medical School
- Abstract 4517, “The impact of surgery on patients with VHL-associated tumors: An international patient survey”
- Presented by Othon Iliopoulos, MD, Associate Professor, Medicine, Harvard Medical School
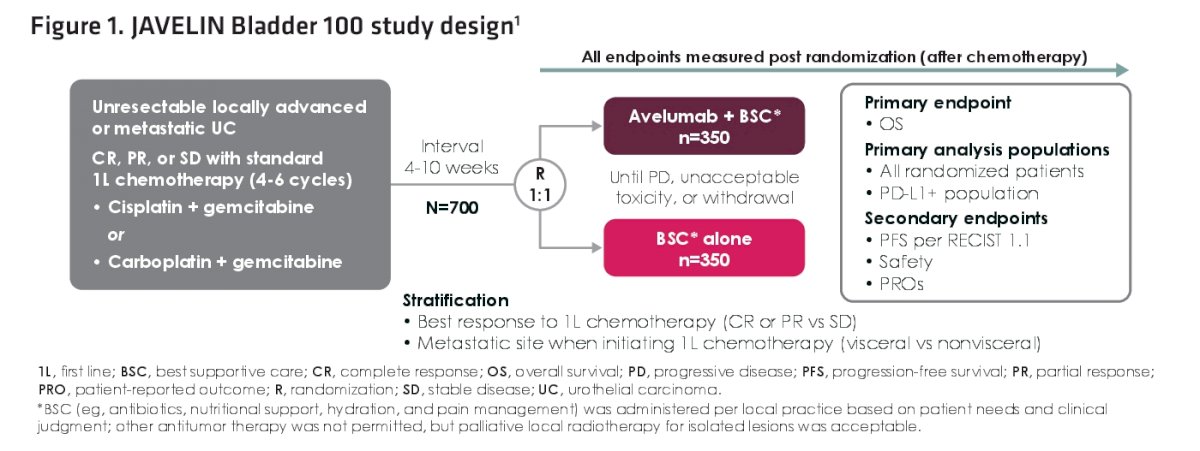
Both the first two abstracts focus on the JAVELIN Bladder 100 trial1 was a landmark study that demonstrated that treatment with Avelumab (AVE) maintenance therapy in the first line on top of best supportive care (BSC) significantly prolonged overall survival (OS) and progression free survival (PFS) in patients with against your filial carcinoma that had not progressed after first line chemotherapy. Summary of the presentations related to this landmark study can be found here: https://www.urotoday.com/tags/javelin-bladder-100-trial-te.html
As a reminder, here is the study design for the original trial:
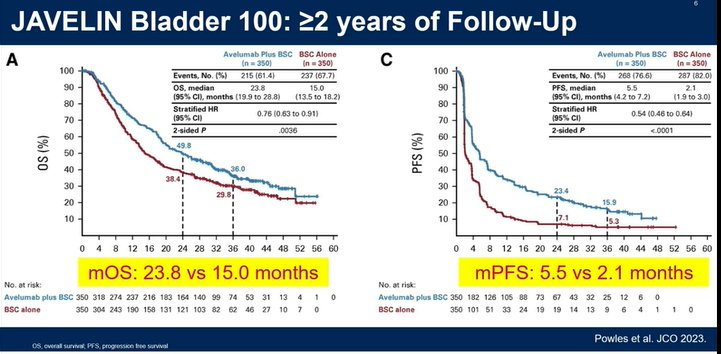
With now two years worth of data, Avelumab continues to demonstrate overall and progression free survival benefit over best supportive care. The toxicity profile remained unchanged. He notes that Dr. Grivas recently published patient-reported outcomes from the trial, demonstrating similar QOL outcomes amongst both arms.
He then jumped into Dr. Powles abstract. This particular study (post-hoc) assesses between-treatment differences using Q-TWiST analysis, Which is an integrated measure that incorporates efficacy safety and patient reported outcomes into a single value. It helps to contextualize the clinical benefit of extended life and delay in progression by accounting for the impact of quality of life due to toxicity and disease progression. when comparing an intervention with the control arm, a positive between treatment difference in Q-TWiST represents a net benefit for the intervention.
This is conceptually seen below:

There are 3 key clinical states: TOX, TWIST and REL. This that is further modified by multiplying these times by utility scores which he will get into it a little bit later in the talk.
The curves specific to this study for each arm is seen below:

Key take-home points:
- TWIST time is larger for avelumab treated patients
- TOX time was slightly longer for avelumab than for BSC
- REL time for avelumab was shorted because these patients spent more time in a progression free state
Regardless of the extremes of different hypothetical utility weight combinations for each of the disease states, the difference in Q-TWiST scores always favored avelumab over BSC alone. Using PRO data utility weights, the data was a little more narrow and potentially more accurate. It still favored avelumab over BSC alone.
He then highlighted some of the limitations of this analysis. specifically this analysis only takes into account grade three or higher toxicities, but in reality and in clinical practice certain grade one or two toxicities can be limiting to patients. In addition the estimation of weighted utility scores based on pro data can have challenges in capturing the full patient experience.
His main take home points where that the addition of avelumab maintenance resulted in delayed disease progression, longer overall survival and relatively safe toxicity profile. Since the Q-TWiST also supports its use, it should not change our clinical decision making. it only further supports our use of Avelumab maintenance as a standard of care.
He then went on to talk to Dr. Bellmunt’s study. He reviewed the baseline characteristic differences between the groups which are relatively evenly balanced. He did note slight enrichment for better performance status in the BSC alone arm and slightly higher rates of visceral metastases in the avelumab arm at the start of therapy.
In all avelumab treated patients (N=344):
- Any grade TRAE occurred in 269 patients (78.2%); Grade 3+ was 67 (19.5%)
- 11.6% had a TRAE that led to discontinuation
- Most patients just had a single irTRAE
Among patients treated for at least 12 months (N=118):
- Any grade TRAE occurred in 59 patients (50%); Grade 3+ was 14 (11.9%)
- 10.2% had a TRAE that led to discontinuation
- Most patients just had a single irTRAE

When looking at the nature of immune related TRAEs, these are summarized below:

He concluded with the following:
- There are no new safety signals identified with longer treatment
- Grade 3+ TRAEs and irTRAEs Occurred in less than 5% of patients after 12 months of treatment
- most patients with any grade irTRAES only had a single irTRAE
- limitations of the study is that there's no long term analysis for the VSC alone arm to compare
This data further supports the use of Avelumab maintenance as a standard of care.
He did question how this data compare to EV+Pembro for patients ineligible for cisplatin chemotherapy – and will there be a new future SOC?
He finally talked about the final abstract. This was an international patient survey focus on the impact of surgery on patients with VHL associated tumors.
He briefly reviewed VHL syndrome, its presentation and its indications for surgery (when the largest tumor reaches approximately 3 cm to prevent metastases). 30-70% of patients with VHL will get RCC.
In this abstract, they reported on an international cross-sectional survey of patients in the US, Canada, UK, France and Germany. Recruited via the VHL alliance. it was one survey and was completed in one setting.
Of the 220 patients that participated, 2/3 were from North America.
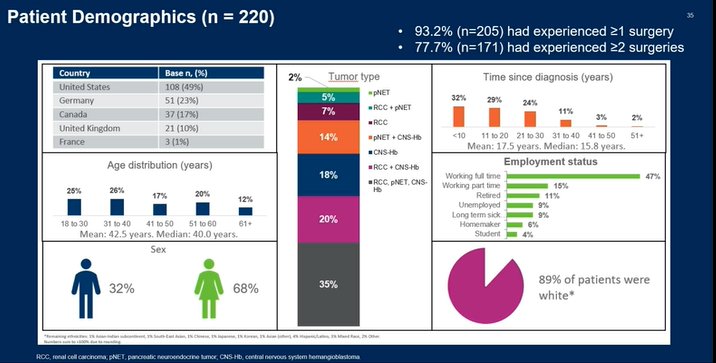
Many had multiple VHL related tumors – 86% had CNS hemangioblastoma, 66% RCC, 55% pNET.
93% had 1+ surgeries and 77% had 2+ surgeries.
Median was 3. Most common was CNS surgery.
When asked about impact of their surgery on the functional status/symptoms, here is the breakdown of responses:

Most patients do not think the surgeries helped with symptoms. Nearly half felt the surgeries contributed to worsening fatigue and mental health.
Many patients actually, when given a choice between watch and wait vs. taking a pill for their VHL, most opted to take a medication despite its associated side effects.

The key takeaways from this last abstract are as follows:
- surgery has significant impact on our patients lives including worsening fatigue mental health and ability to participate in activities of daily life
- most patients would prefer to take a pill to possibly delay surgery
The limitations of this study is that it is a survey at a single point in time and the full safety profile available on medication was not made aware to the participants.
Therefore he concludes that treatments such as Beltizufan should be offered and discussed with patients.
Presented by: Benjamin Garmezy, MD | Sarah Cannon Research Institute at Tennessee Oncology
Written by: Thenappan (Thenu) Chandrasekar, MD – Urologic Oncologist, Associate Professor of Urology, University of California, Davis, @tchandra_uromd @UCDavisUrology on Twitter during the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 2 – Tues, June 6, 2023.