(UroToday.com) The 2023 ASCO annual meeting included a bladder cancer session, featuring a presentation by Dr. Andrea Necchi discussing the biology and performance of pre- and post-pembrolizumab VI-RADS to predict the pathological response in MIBC. VI-RADS is a standardized reporting system that uses multiparametric magnetic resonance imaging (mpMRI) parameters to predict the probability of MIBC.1,2 Additionally, it has also been used in studies using standard neoadjuvant chemotherapy. However, no studies have analyzed the performance of VI-RADS to predict the ypT0 or ypT≤1 response post-immunotherapy in MIBC.
In the PURE-01 study, patients were staged with mpMRI before and after treatment (3 cycles of pembrolizumab) prior to radical cystectomy, and all mpMRI scans were centrally reviewed. Logistic regression models analyzed pre- and post-pembrolizumab VI-RADS against pT≤1 (primary endpoint) and pT0 (secondary endpoint). VI-RADS scores were dichotomized between 0-3 (0=no evidence of disease) and 4-5. Covariates included cT-stage, age, gender, PD-L1 combined positive score, and tumor mutational burden. Model performance was also tested in the ongoing NureCombo (nivolumab + nab-paclitaxel; NCT04876313) and SURE-01 (sacituzumab govitecan; NCT05226117) trials. Additionally, transcriptome-wide expression profiling was matched with VI-RADS scores.
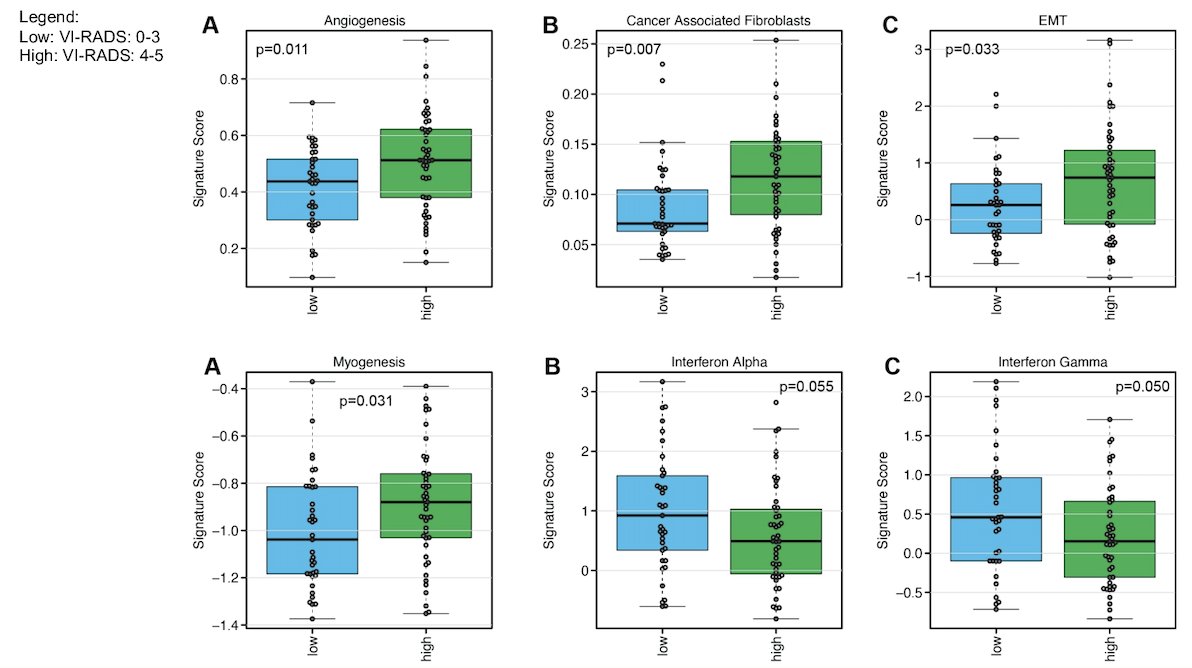
In PURE-01, 110 patients had centrally reviewed MRI scans (n=220 mpMRIs), treated between February 2017 and July 2020. In total, 30 (27.3%) patients had pure/predominant non-urothelial carcinoma histology, and 52 (47.3%) patients had cT3-4N0 MIBC. In the pre-pembrolizumab population, 21 patients (19.1%) had no measurable disease (VI-RADS=0), 34 (30.9%) a VI-RADS 1-3 score, and 55 (50.0%) had a VI-RADS 4-5 score. There were 20 patients (18.2%) that had downstaging from VI-RADS 4-5 to VIRADS 0-3 post-pembrolizumab. Pre-pembrolizumab VIRADS 4-5 was associated with higher angiogenesis and epithelial-mesenchymal transition activity vs VI-RADS 0-3 (p=0.011 and 0.033):
Both pre-pembrolizumab and post-pembrolizumab VI-RADS 0-3 scores were the only significant covariates against ypT≤1 endpoint on multivariable analyses: the strongest effect was seen with post-pembrolizumab VI-RADS 0-3 against pT≤1 response (OR: 21.58, 95% CI: 6.97-78.96, p<0.001), with an AUC of this model being 0.90:

Model-based decisions were supported in the range of threshold probabilities of 10-80%. Post-pembrolizumab VI-RADS 4-5 was characterized by higher stromal signature scores vs VI-RADS 0-3. As follows is the event free survival and OS using pre-pembrolizumab VI-RADS:

Similarly, as follows is the event free survival and OS using post-pembrolizumab VI-RADS, both of which were statistically significant:

When post-therapy VI-RADS were tested in evaluable patients from the combined NureCombo + SURE-01 cohort (n=17 patients, 34 mpMRI): 90% of post-VI-RADS 0-3 revealed a pT≤1 stage at radical cystectomy.
Dr. Necchi concluded his presentation by discussing the biology and performance of pre- and post-pembrolizumab VI-RADS to predict the pathological response in MIBC with the following take-home messages:
- MRI with VI-RADS for response assessment of pembrolizumab in MIBC revealed a way for the noninvasive prediction of the pathological response and outcome, opening new avenues for a better selection of candidates to bladder-sparing strategies within clinical trials
- Different VI-RADS scores not only mirrored the probability of residual MIBC after TURBT but also identified distinct biological features potentially associated with immunotherapy response
- Based on the existing evidence, MRI use should be offered to clinicians in clinical trials and routine practice to improve their ability to assess the response to treatment whenever neoadjuvant immunotherapy is envisioned, strengthen the decision making, enhance bladder-sparing strategies, and inform patients in the clinic
Presented by: Andrea Necchi, MD, Vita-Salute San Raffaele University, Milan, IT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 2 – Tues, June 6, 2023.
References:
- Panebianco V, Narumi Y, Altun E, et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting and Data System). Eur Urol 2018 Sep;74(3):294-306.
- Del Giudice F, Barchetti G, De Berardinis E, et al. Prospective assessment of Vesical Imaging Reporting and Data System (VI-RADS) and its Clinical Impact on the Management of High-risk non-muscle-invasive bladder cancer patients candidate for repeated transurethral resection. Eur Urol 2020 Jan;77(1):101-109.