(UroToday.com) The 2022 ASCO annual meeting featured a session on prostate cancer, including a presentation by Dr. Claire Vale discussing a meta-analysis of individual participant data (IPD) from randomized trials to more precisely define the effects of docetaxel plus ADT for men with mHSPC. Adding docetaxel to ADT improves survival in mHSPC, but uncertainty remains about who benefits most. To investigate this thoroughly and reliably, the STOPCAP M1 collaboration conducted a meta-analysis of IPD from relevant trials.
The methods were included in a registered protocol (CRD42019140591). Updated IPD from the GETUG-15,1 CHAARTED,2 and STAMPEDE3 trials were harmonized and checked:
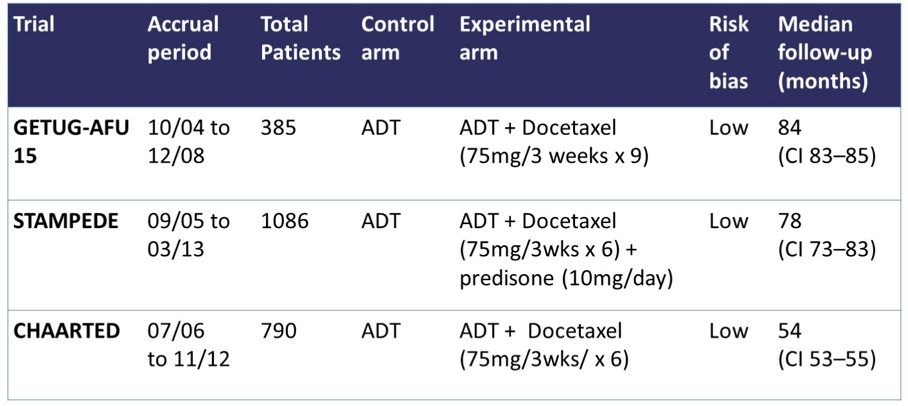
The main outcomes were overall survival (OS), progression-free survival (PFS) and failure-free survival (FFS). Overall pooled effects were estimated using intention-to-treat, 2-stage, fixed-effect meta-analysis, adjusted for age, PSA, Gleason sum score, performance status, and timing of metastatic disease (missing covariate values imputed), with 1-stage and random-effects sensitivity analyses. Dr. Vale and colleagues assessed subgroup effects using 2-stage, fixed-effect meta-analysis of within-trial interactions, adjusted for the same covariates. They based these on PFS to maximize power, and OS whenever interactions were found. To explore multiple subgroup interactions, and to derive subgroup-specific absolute treatment effects, they used 1-stage, flexible parametric modelling and standardization.
For this study, Dr. Vale and colleagues obtained IPD for all 2,261 men randomised, with median follow-up of 6 years (all patients). The mean age was 64 years, and most men had synchronous disease (83%), WHO performance status of 0 (75%), and Gleason >= 8 (63%). There were clear relative benefits of docetaxel on OS (HR 0.79, 95% CI 0.70 to 0.88, p<0.0001), PFS (HR 0.70, 95% CI 0.63 to 0.77, p<0.0001) and FFS (HR 0.64, 95% CI 0.58 to 0.71, p<0.0001). With evidence of non-proportional hazards, the estimated 5-year absolute differences were: OS 11% (95% CI 6 to 15%), PFS 9% (95% CI 5 to 13%) and FFS 9% (95% CI 6 to 12%). The relative effect of docetaxel on PFS differed by volume of metastases (interaction p=0.027; high volume HR = 0.60, 95% CI 0.52 to 0.68; low volume HR = 0.78, 95% CI 0.64 to 0.94) and timing of metastatic disease (interaction p=0.077; synchronous HR = 0.67, 95% CI 0.60 to 0.75; metachronous HR = 0.89, 95% CI 0.67 to 1.18). OS results were similar. When metastatic disease volume and timing were combined, docetaxel appeared to improve PFS and OS for all men, except those with low volume, metachronous disease:

Additionally, the benefits of docetaxel on PFS were greatest in men with high volume disease, particularly those with clinical T4 disease:

Dr. Vale concluded her presentation discussing a meta-analysis of IPD from randomized trials to more precisely define the effects of docetaxel plus ADT for men with mHSPC emphasizing that this IPD meta-analysis provides the most detailed assessment of the effects of docetaxel for mHSPC, and suggests that men with low volume, metachronous disease should be managed differently to those with other types of metastatic disease.
Presented by: Claire L. Vale, MRC Clinical Trials Unit at UCL, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 3 – Mon, June 7, 2022.
References:
- Gravis G, Boher JM, Joly F, et al. Androgen Deprivation Therapy (ADT) Plus Docetaxel Versus ADT Alone in Metastatic Non castrate Prostate Cancer: Impact of Metastatic Burden and Long-term Survival Analysis of the Randomized Phase 3 GETUG-AFU15 Trial. Eur Urol. 2016;70(2):256-262.
- Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015;373(8):737-746.
- James ND, Sydes MR, Clarke NW, et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet. 2016;387(10024):1163-1177.