(UroToday.com) The 2022 ASCO annual meeting featured a session on prostate cancer, including a presentation by Dr. Diogo Bastos discussing pathologic response and PSMA imaging correlates from a randomized phase II trial of neoadjuvant ADT plus abiraterone and apalutamide for patients with high-risk localized prostate cancer. Patients with high-risk localized prostate cancer have a significant risk of disease recurrence and metastasis after radical prostatectomy. Neoadjuvant therapy remains investigational but there may be a role for the next-generation androgen signaling inhibitors. Dr. Bastos and colleagues sought to evaluate pathologic and imaging responses after the intense neoadjuvant approach.
This is a phase II investigator-initiated randomized trial of 3-month neoadjuvant therapy with goserelin (ADT) + abiraterone acetate and prednisone (AAP arm) or abiraterone acetate and prednisone + apalutamide (A-APA arm) before radical prostatectomy for patients with high-risk localized prostate cancer (Gleason ≥ 8 and/or cT3N0-1 and/or PSA ≥ 20 ng/mL). The study design is as follows:
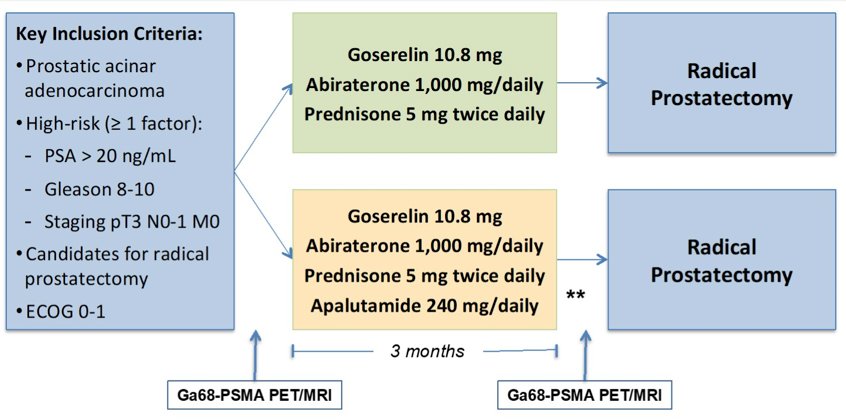
The primary endpoint was the rate of pathologic complete response or minimal residual disease (tumor ≤ 0.5 cm). The secondary endpoints were safety, rate of residual cancer burden ≤0.25 cm3 (tumor volume x cellularity), Gallium 68 PSMA-PET/MR correlates and rate of biochemical relapse.
There were 62 patients randomized to A-APA (n = 31) or AAP (n = 31), with a median age of 65 (range 47-77) years. NCCN risk groups included high-risk disease in 19%, very high-risk in 76%, and regional (N1) disease in 5% (79% cT3, 65% Gleason 8-10, 57% PSA ≥ 20 ng/mL). There was no statistically significant difference between study arms regarding pathologic complete response/minimal residual disease or residual cancer burden ≤ 0.25 cm3 rates:

Patients with complete PSMA-PET response demonstrated a residual cancer burden ≤ 0.25 cm3 rate of 50% compared to 7.5% in patients without a complete PSMA-PET response (p = 0.001). The rate of biochemical relapse was 14% for patients with residual cancer burden ≤ 0.25 cm3 versus 38% in patients with residual cancer burden > 0.25 cm3 (p = 0.118). At current median follow-up of 2.6 years, all patients with both complete PSMA-PET response and residual cancer burden ≤ 0.25cm3 (N = 11, 18%) are free of biochemical relapse. There were two grade 5 adverse events in the AAP arm (pulmonary embolism and sudden death, both after surgery), and 9 (14.5%) patients (6 in A-APA; 3 in AAP) experienced grade 3-4 treatment-related adverse events. The most common grade 3-4 adverse events were hypertension (11.3%), AST/ALT elevations (3.2%), and skin rash (1.6%).
Dr. Bastos concluded this presentation by discussing pathologic response and PSMA imaging correlates from a randomized phase II trial of neoadjuvant ADT plus abiraterone and apalutamide for patients with high-risk localized prostate cancer with the following take-home messages:
- There was no difference in pathologic complete or minimal residual disease observed between arms
- Although pathologic complete or minimal residual disease after intense neoadjuvant ADT was infrequent, a significant proportion of patients achieved a favorable pathologic response with residual cancer burden ≤ 0.25 cm3
- PSMA-PET response is a potential surrogate for pathologic response
Presented by: Diogo A. Bastos, Instituto do Câncer do Estado de São Paulo, São Paulo, Brazil
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 3 – Mon, June 7, 2022.