(UroToday.com) At the 2022 American Society of Clinical Oncology Annual Meeting held in Chicago and virtually, the poster session focused on Prostate, Testicular, and Penile cancers on Monday afternoon included a presentation from Dr. Tamim Niazi describing the rationale, design, and protocol of the DASL-HiCaP trial of darolutamide, along with androgen deprivation therapy, for patients undergoing definitive or salvage radiotherapy.
Radiation therapy (RT), plus androgen deprivation therapy (ADT) with a luteinizing hormone-releasing hormone analog (LHRHA), is the standard of care for men with very high-risk localized prostate cancer (PC), or with very high-risk features and persistent PSA after radical prostatectomy (RP). Despite this, incurable distant metastases develop within 5 years in 15% of men with very high-risk features. Thus, there is an unmet need to improve care for these patients through treatment intensification.
Darolutamide is a structurally distinct and highly potent androgen receptor inhibitor. Like apalutamide and enzalutamide, a randomized clinical trial of darolutamide (ARAMIS, NCT02200614) demonstrated significantly increased median metastasis-free survival by ̃2 years and improved overall survival in men with non-metastatic castration-resistant prostate cancer (nmCRPC), with a favorable tolerability profile. Further, in the ARASENS trial, triplet therapy with darolutamide, docetaxel, and ADT improved overall survival compared to docetaxel and ADT.
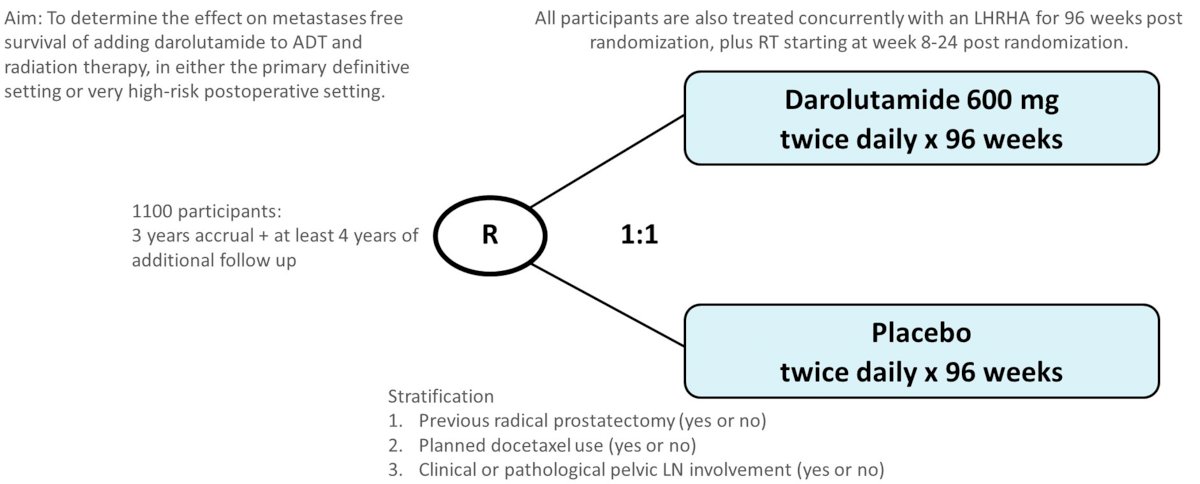
Thus, the authors aim is to determine the efficacy of adding darolutamide to ADT and RT in the setting of either primary definitive therapy or salvage therapy for very high-risk PC.
DASL-HiCaP is a randomized (1:1), phase 3, placebo-controlled, double-blind trial for men planned for RT who have very high-risk localized PC on conventional imaging; or very high-risk features with PSA persistence or rise within one year following RP (NCT04136353). Given the somewhat broad inclusion criteria, the trial is stratified by prior radical prostatectomy, the use of adjuvant docetaxel, and pelvic nodal involvement.
1100 participants will be randomized to darolutamide 600 mg or placebo twice daily for 96 weeks. All included participants will receive LHRH agonist for 96 weeks, plus RT starting week 8-24 from randomization.
Participants are allowed nonsteroidal antiandrogen in addition to LHRH agonist for up to 90 days prior to randomization at the discretion of the treating physician. Additionally, early treatment with up to 6 cycles of docetaxel completed at least 4 weeks prior to RT is permitted.
The primary endpoint of this trial is metastasis-free survival (ICECaP-validated), with numerous secondary endpoints including overall survival, prostate cancer-specific survival, PSA-progression-free survival, time to subsequent hormonal therapy, time to castration-resistance, frequency and severity of adverse events, health-related quality of life, fear of recurrence. Tertiary endpoints include incremental cost-effectiveness, and identification of prognostic and/or predictive biomarkers of treatment response, safety, and resistance to study treatment.
Currently, with enrollment having open March 31, 2020, 56 sites have been activated and 530 patients have been randomized.
Presented by: Tamim Niazi, MD, Jewish General Hospital, McGill University, Montréal, QC, Canada