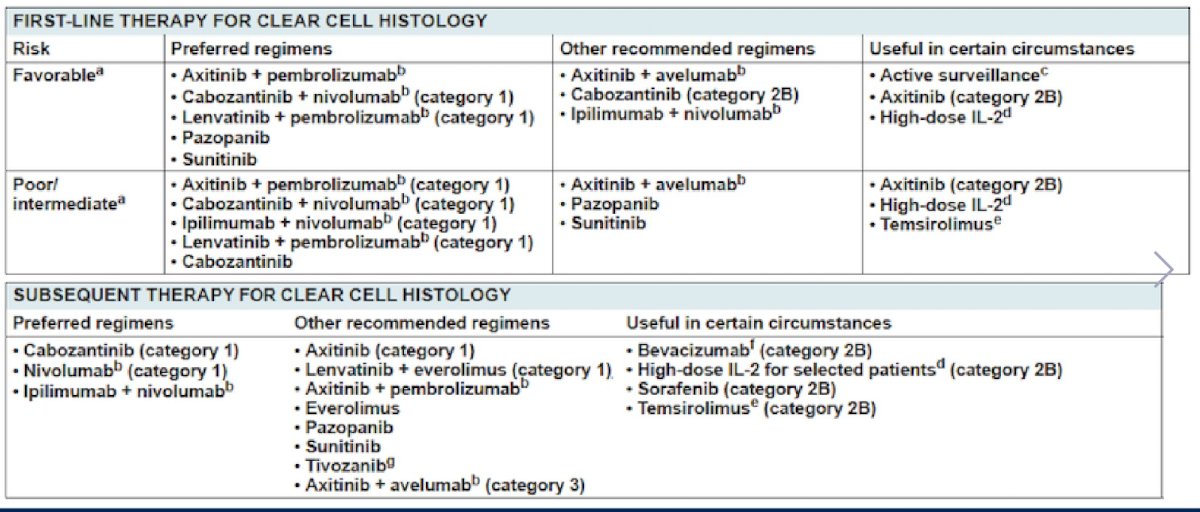
(UroToday.com) The 2022 ASCO annual meeting included a poster discussion session for kidney and bladder cancer, including a discussant presentation from Dr. Anil Kapoor discussing moving beyond TKI and immune-oncology in renal cell carcinoma (RCC). Dr. Kapoor started by highlighting the latest (2021) NCCN kidney cancer guidelines:
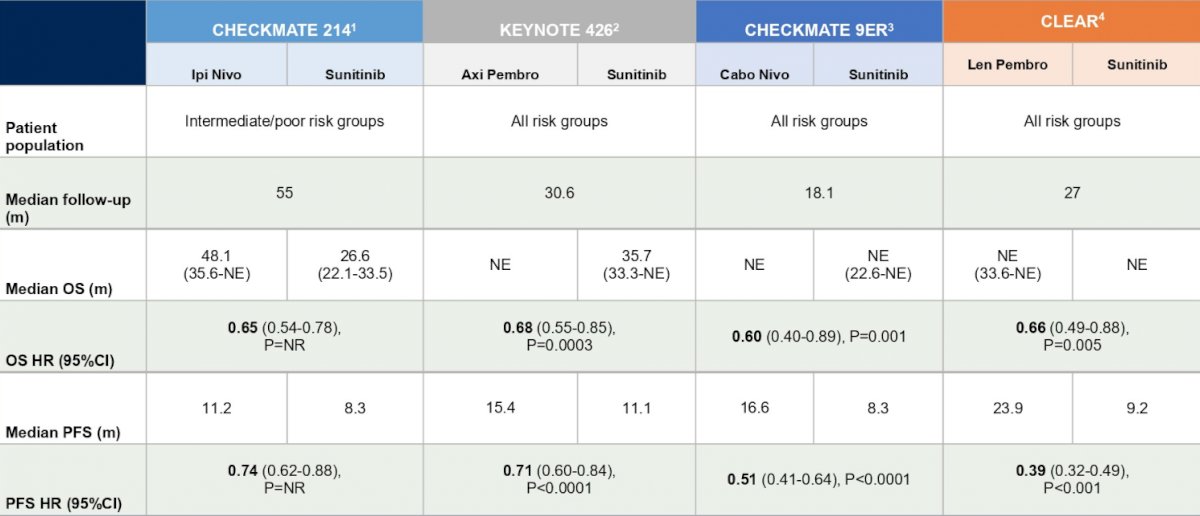
Currently, we have four IO/TKI trials that have showed PFS and OS benefit versus sunitinib, including CheckMate-214 [1], KEYNOTE-426 [2], CheckMate 9ER [3], and CLEAR [4]. A summary of the PFS and OS results is as follows:
Dr. Kapoor asks: How much further can we go with TKI, mTOR, and IO therapies? Triplet therapy (PD1 inhibitors, CTL4 inhibitor, TKI)? What about novel new mechanism of action therapies? In this presentation Dr. Kapoor discussed the following abstracts “Phase 1 LITESPARK-001 (MK-6482-001) study of belzutifan in advanced solid tumors: Update of the clear cell RCC cohort with more than 3 years of total follow-up” presented by Dr. Eric Jonasch, “A phase 1b/2 study of batiraxcept (AVB-S6-500) in combination with cabozantinib in patients with advanced or metastatic clear cell RCC who have received front-line treatment (NCT04300140)” presented by Dr. Neil Shah, and “Characterization of the microbial resistome in a prospective trial of CBM588 in metastatic RCC offers mechanism for interplay between antibiotic use and ICI activity” presented by Dr. Nazli Dizman.
VHL disease is associated with malignant or benign tumors, including renal cell carcinoma (RCC), pancreatic neuroendocrine tumors (pNETs), and hemangioblastomas. Alterations in the VHL gene cause aberrant stabilization and accumulation of HIF-2α, leading to activation of genes associated with tumor growth. Belzutifan is a selective small molecule HIF-2alpha inhibitor, showing favorable safety and antitumor activity in previous studies. At ASCO 2021, Ramaprasad Srinivasan presented data of an ongoing open-label phase 2 study (NCT03401788) of belzutifan in patients with VHL disease, noting over a median follow-up of 21.8 months (range 20.2-30.1), the objective response rate was 49.2% (95% CI 36.1-62.3%). Additionally, there were 40 confirmed partial responses (ORR, 49.2%), 4 (6.6%) unconfirmed responses, and no patients had progressive disease. The authors concluded at that time that belzutifan demonstrates clinical benefit and has a favorable safety profile in patients with VHL disease and associated tumors.
The phase 1 LITESPARK-001 trial presented at ASCO 2022 reported an update of the clear cell RCC cohort with more than 3 years of follow-up. Patients received oral belzutifan 120 mg once daily, and this analysis included median follow-up of 41 months (range: 38.2-47.7). Among 55 patients enrolled in the clear cell RCC cohort, 9 (16%) remain on treatment at the time of the data cutoff (July 15, 2021). Patients received a median of 3 prior therapies (range 1-9), and 39 (71%) received prior VEGF and immunotherapy. Twenty-two patients (40%) experienced grade 3 treatment related adverse events, with the most common (≥10%) grade 3 events being anemia (n = 13; 24%) and hypoxia (n = 7; 13%). ORR was 25%, with 1 confirmed complete response (2%) and 13 partial responses (24%). Per IMDC risk, 4 of 13 patients with favorable risk achieved response (ORR = 31%; all partial responses) and 10 of 42 patients with intermediate/poor risk achieved response (ORR = 24%; 1 complete response, 9 partial responses). For patients who received prior VEGF and immunotherapy, 8 of 39 patients achieved response (ORR = 21%; 1 complete response; 7 partial responses). For the 16 patients who did not receive prior VEGF/immunotherapy, 6 achieved response (ORR = 38%; all partial responses). Median PFS for the total cohort was 14.5 months (95% CI, 7.3-22.1) and PFS rate at 156 weeks (~36 months) was 34%.
Dr. Kapoor’s conclusions from the LITESPARK presentation are as follows:
- With extended follow-up of 41 months, belzutifan continued to demonstrate durable antitumor activity and manageable safety in heavily pretreated patients with sporadic advanced clear cell RCC
- The ORR of 25% has been maintained since the primary analysis, with responses observed across subgroups, including in patients who had previously received IO and VEGF therapy
- Median duration of response was not reached (range: 3.1+ to 38.0+ months)
- Belzutifan is an effective treatment option for VHL patients, and decreases the need for surgical interventions
Dr. Kapoor poses the following questions/comments with regards to belzutifan moving forward:
- How long should we continue therapy? For non-metastatic disease, should we stop after 1-2 years and reintroduce at the time of progression?
- LITESPARK was pre-treated mRCC, with impressive 3 year responses
- Belzutifan is a promising therapeutic target for mRCC in single agent, with combination agent trials ongoing
Dr. Kapoor then discussed the phase 1b/2 study of batiraxcept (AVB-S6-500) in combination with cabozantinib clear cell RCC who received front-line therapy. The AXL receptor and its activating ligand GAS6 drives metastasis and therapeutic resistance in cancer. AXL is up-regulated by HIF-1 signaling in VHL-deficient and hypoxic tumor cells, and overexpression is strongly correlated with clear cell RCC patient prognosis and survival. Batiraxcept is a recombinant fusion protein containing an extracellular region of human AXL combined with the human immunoglobulin G1 heavy chain (Fc). This is highly specific and potent for AXL inhibition:
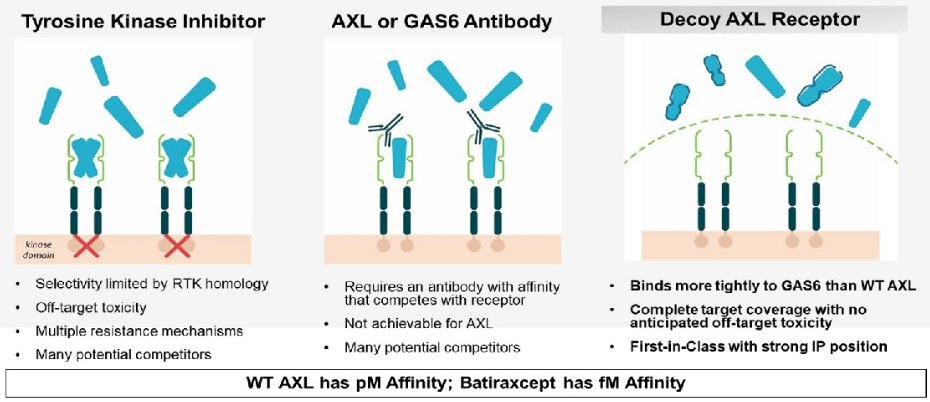
Furthermore, batiraxcept binds GAS6, thus inhibiting interaction with AXL and reducing invasion and migration of human cancers. It has been well tolerated in prior trials, with infusion related reaction and fatigue being the most common adverse events.
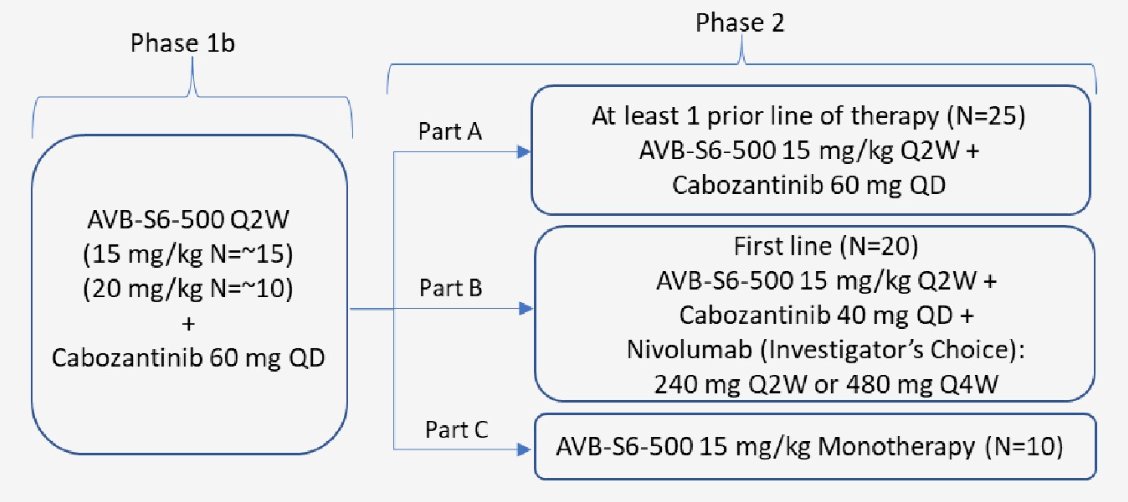
In this trial, batiraxcept at doses of 15 and 20 mg/kg, plus cabozantinib 60 mg daily, was evaluated using a 3+3 dose escalation study design. The primary objective was safety, and secondary and exploratory objectives included identification of the recommended phase 2 dose (RP2D), overall response rate (ORR), and duration of response (DOR). Additionally, correlation of serum soluble AXL/GAS6 with ORR was evaluated. Key eligibility criteria include previously treated (two or more lines of therapy) clear cell RCC patients, and prior treatment with cabozantinib was not allowed. The trial schema is as follows:
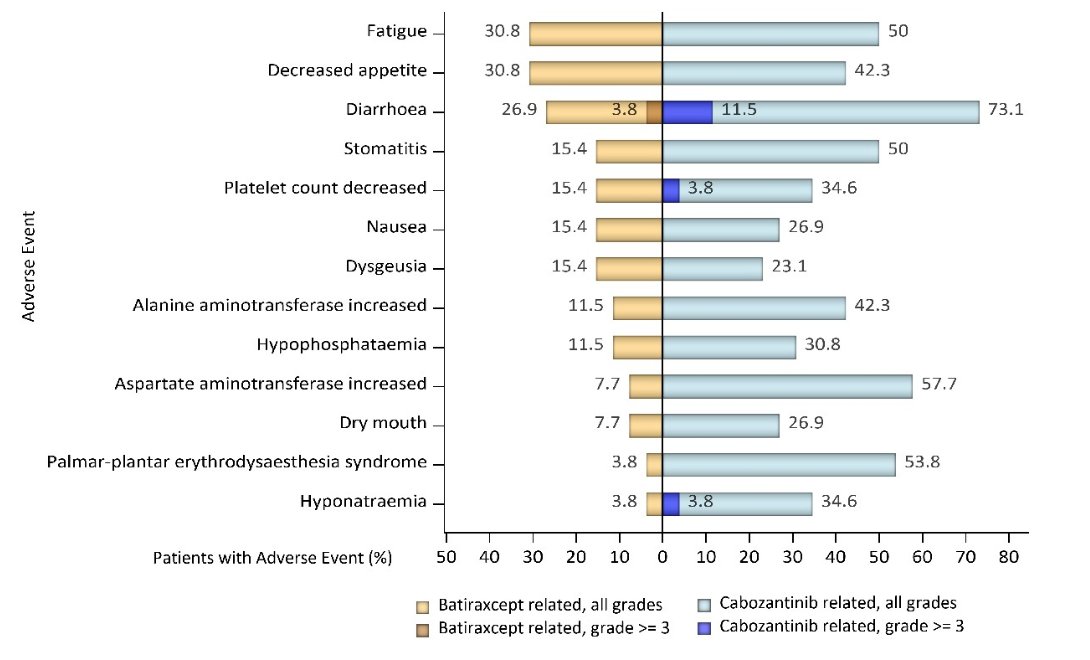
In this phase 1b trial, 26 patients have been enrolled, including 16 patients treated with 15 mg/kg and 10 patients with 20 mg/kg dose of batiraxcept. At median follow up of 4.9 months, 92% (n=24) patients remained on the study. No dose limiting toxicities were observed at either 15 mg/kg or 20 mg/kg dose, and batiraxcept/cabozantinib-related adverse events occurred in 17 subjects (65%). The most common related adverse events include decreased appetite 31% (n=8), diarrhea, and fatigue 23% (n=6). Grade 3 related adverse events occurred in 4 patients (15%) including diarrhea, thromboembolism, hypertension, small bowel obstruction, and thrombocytopenia (n=1, 4% each) being most common. No grade 4 or 5 related adverse events were observed. A summary of the safety data is as follows:
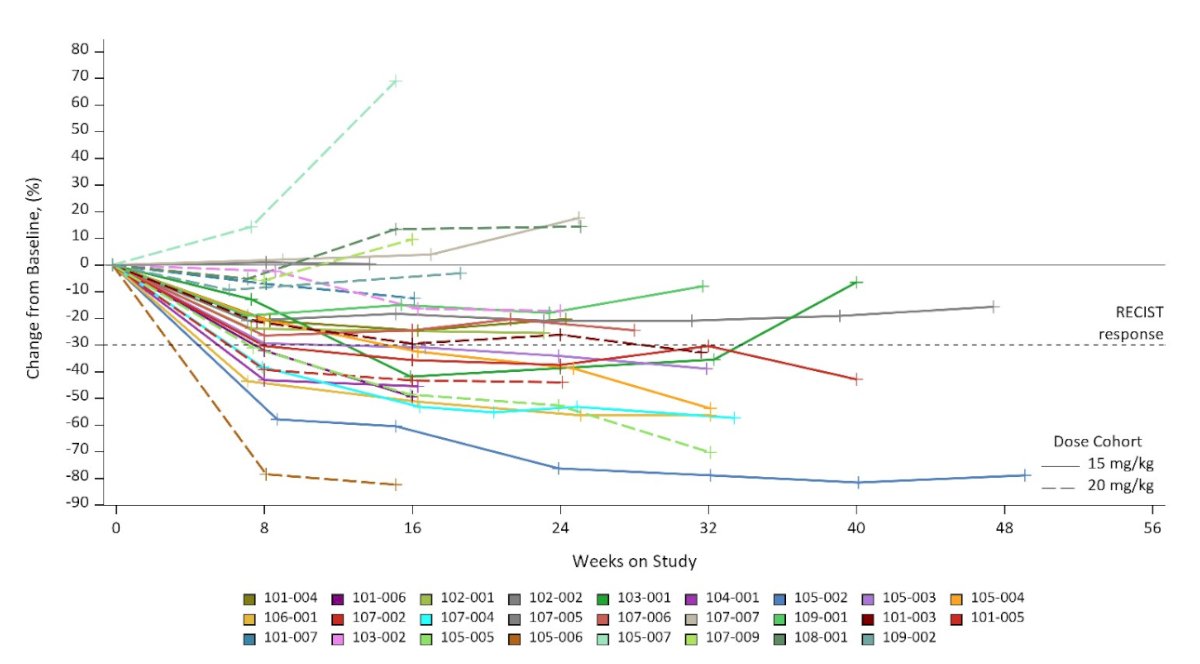
Among the patients who had baseline soluble AXL/GAS6 ratio of ≥ 2.3, the ORR was 67%. Regardless of baseline soluble AXL/GAS6 ratio, 3-month duration of response was 100%, and 6-month progression free survival was 79%. The ORR was 42% and no patients had primary progressive disease. There were 8 patients that experienced resolution of one or more target lesions, of which all responders were biomarker high:
Dr. Kapoor noted that Dr. Shah and colleagues concluded this presentation noting that batiraxcept plus cabozantinib is well tolerated, and the RP2D of batiraxcept was identified as 15 mg/kg. Early efficacy signals were observed including 100% duration of response at 3 months, and baseline soluble AXL/GAS6 may serve as a potential biomarker to enrich the population.
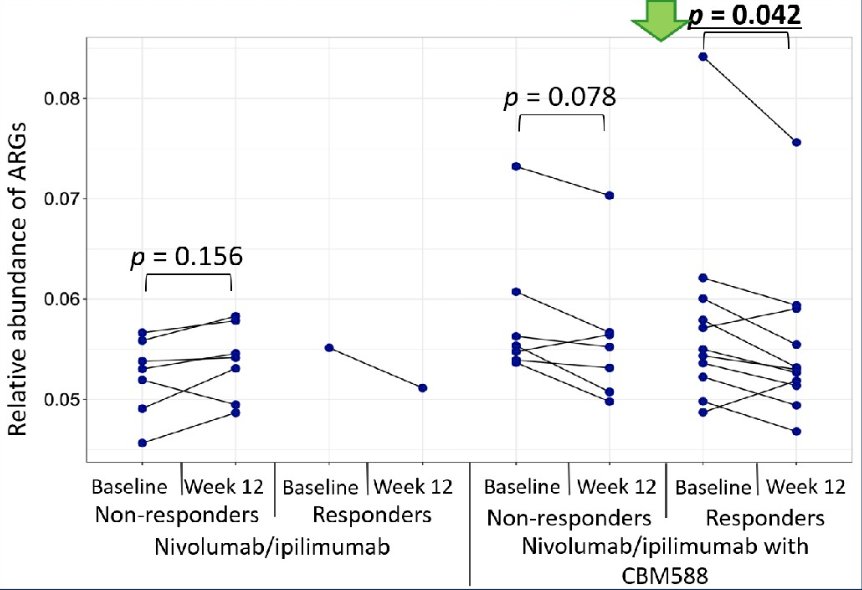
To conclude his presentation, Dr. Kapoor discussed the prospective trial of CBM588 in metastatic RCC. Dr. Kapoor notes that the negative association between immune checkpoint inhibitor response and antibiotic therapy is well defined. Paradoxically, retrospective data of the live bacterial product CBM588 in patients with advanced small cell lung cancer showed improved outcomes with immune checkpoint inhibitors when the combination of CBM588 and antibiotics were employed. Dr. Dizman and colleagues postulated that the microbial resistome (genes encoding antimicrobial resistance) could shift in a manner with CBM588 therapy that facilitated ICI response. Patients with newly diagnosed mRCC were randomized to nivolumab + ipilimumab or nivolumab + ipilimumab + CBM588 in a 1:2 ratio. Stool samples were collected at baseline and week 12, and whole-metagenome sequencing was performed to analyze stool microbiome composition. Antibiotic resistance genes were inferred using publicly available database, and groups of antibiotic resistance genes for various classes of antibiotics were characterized. The trial schema is as follows:

This study enrolled 30 patients, with the final analysis including 29 eligible patients. The objective response was 20% for nivolumab + ipilimumab and 58% in the nivolumab + ipilimumab + CBM588 arm. The overall abundance of antibiotic resistance genes remained unchanged between baseline and week 12 in patients receiving nivolumab + ipilimumab alone. In contrast, a decrease in antibiotic resistance genes was observed in patients receiving nivolumab + ipilimumab + CBM588 arm from baseline to week 12 (p = 0.042 in responders; p = 0.078 in non-responders):
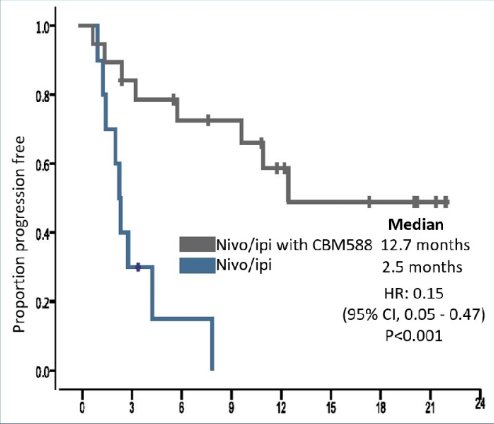
Median PFS was 12.7 months for nivolumab + ipilimumab + CBM588 versus 2.5 months for nivolumab + ipilimumab (HR 0.15, 95% CI 0.05-0.47):
Dr. Kapoor’s conclusions of the CBM588 trial are as follows:
- CBM588 decreases antibiotic resistance genes associated with multiple commonly used classes of antibiotics, facilitating the ability of antibiotics to clear resistant (potentially pathogenic) bacteria
- CBM588 enhances efficacy of immune checkpoint inhibitors to an even greater extent in patients receiving antibiotics
- Clinical studies of antibiotic priming for CBM588 + immune checkpoint inhibitors may be warranted
- Dr. Dizman and colleagues have tried to clarify this paradox by examining the antibiotic resistant genes
Presented by: Anil Kapoor, BSc, BEngr, MD, FRCS, Juravinski Cancer Centre, McMaster University, Hamilton, Ontario, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 3 – Mon, June 7, 2022.
References:
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carinoma. N Engl J Med 2018;378(14):1277-1290.
- Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med 2019;380(12):1116-1127.
- Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021 Mar 4;384(9):829-841.
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. 2021 Apr 8;384(14):1289-1300.