(UroToday.com) At the 2022 American Society of Clinical Oncology Annual Meeting held in Chicago and virtually, the poster session focused on Kidney and Bladder cancers on Saturday afternoon included a presentation from Dr. Sergio Vazquez-Estevez discussing interim results from the ATEZOBLADDERPRESERVE trial of atezolizumab in combination with radiotherapy as a bladder preserving treatment for patients with muscle invasive bladder cancer (MIBC).
Nearly one-quarter of patients newly diagnosed with bladder cancer present with muscle invasive disease. Currently, for those who are eligible, cisplatin-based neoadjuvant chemotherapy prior to radical cystectomy (RC+PLND) is the standard of care for patients with localized MIBC. An alternative is bladder-preserving therapy for patients who are not candidates for radical cystectomy by medical reasons, refusal, or patient´s choice. These approaches typically combine transurethral resection of bladder tumor (TURBT), radiosensitizing chemotherapy, and radiotherapy. However, immune therapies seem to potentiate tumor-specific immune response induced by radiotherapy (RT). Thus, combining RT with anti-PD-1/PD-L1 therapy appears safe with promising activity. As a result, the authors designed this study to assess the efficacy and safety of atezolizumab concurrent with external beam radiotherapy (EBRT) for the treatment of muscle-invasive bladder cancer (MIBC).
In this abstract, the authors present interim results of this open-label, multicenter, phase II trial, sponsored by SOGUG (NCT04186013). They enrolled patients with a confirmed diagnosis of (cT2-T4a N0 M0) who were deemed not candidates for radical cystectomy. Patients received 6 doses of atezolizumab 1200 mg IV every 3 weeks, starting on day 1 of EBRT, and 60 Gy of RT in 30 fractions over 6 weeks at 2 Gy/day. The primary endpoint of the study was to assess pathological complete response (pCR) defined as a response of grade 5 according to Miller and Payne criteria, 1 to 2 months after the last dose of atezolizumab.
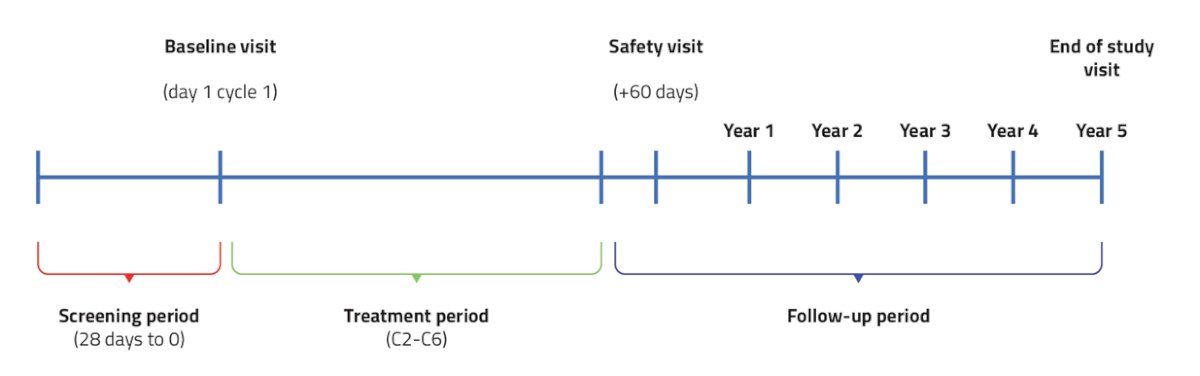
A planned interim analysis has been performed with a data cut-off of November 2021 on the primary endpoint to avoid exposure to ineffective treatment according to the minimax two-stages Simon’s design. They used a stopping rule in which it was assumed that 9 out of the first 13 evaluable patients should achieve pCR. As secondary outcomes, they assessed the incidence of adverse events (AE) and serious AE (SAE).
Between September 2019 and November 2021, 39 patients were screened, 13 were excluded due to non-compliance with eligibility criteria, and 26 were included in the evaluable population. Among these 26 patients, 22 received at least one dose of atezolizumab and formed the safety cohort. 14 patients were evaluable for pathologic response and formed the interim efficacy analysis population. Among the 14 patients in the efficacy population, the median age was 78.6 years and most (71.4%) had clinical stage T2a disease while 14.3% had T2b, 7.1% had T3a, and 7.1% had T3b disease.
As of the data cut-off, all 14 patients had achieved pCR.
In the safety population, 20/22 (91%) patients experienced at least one AE, with asthenia (11), diarrhea (9), and urinary tract infection (4) being the most common.
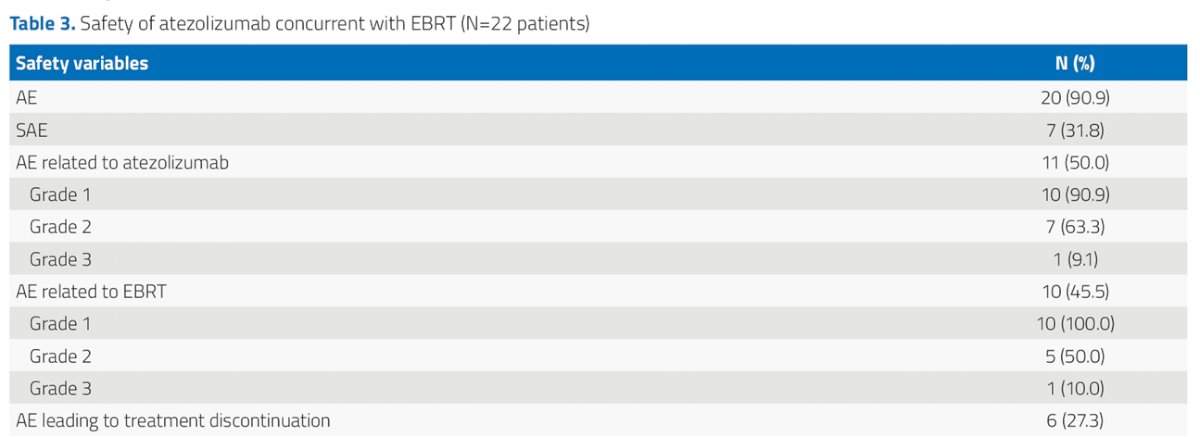
Nine unique SAEs were reported in 7 (32%) patients including bacteriemia, COVID-19 infection, depressed LVEF, unknown origin fever, hepatic toxicity, kidney failure, rectorrhagia, respiratory infection, and urinary sepsis. AEs leading to treatment discontinuation were noted in 6 (27%) patients. However, no AEs leading to death occurred.
The authors conclude that these interim results suggest that the combination of atezolizumab and concurrent radiotherapy is a feasible and effective treatment for MIBC with favourable pathologic complete response rates and a manageable safety profile.
Presented by: Sergio Vazquez-Estevez, Hospital Universitario Lucus Augusti, Lugo, Spain