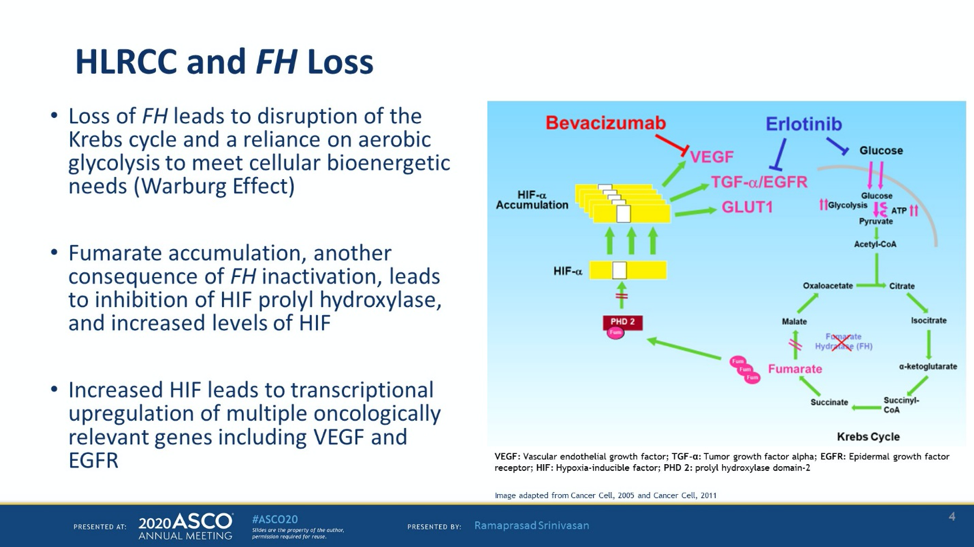
FH inactivation also results in VHL independent upregulation of hypoxia induced factor and activation of the NRF2 pathway. This study evaluates bevacizumab (a VEGF-A inhibitor) and erlotinib (an EGFR TKI).
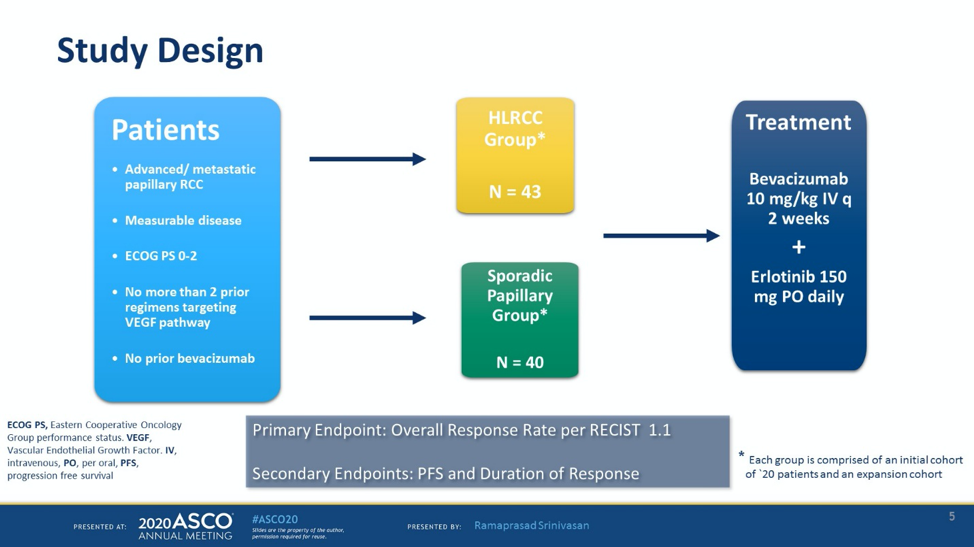
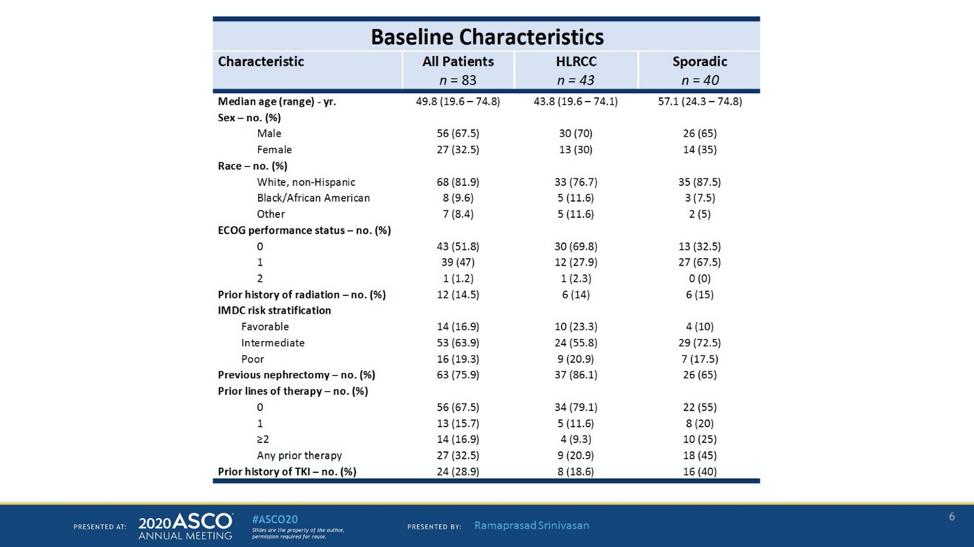
The study schema is shown above. This study enrolled a total of 83 patients with papillary RCC. About half of the patients were HLRCC and the other half had sporadic papillary RCC. Baseline characteristics are shown below. Most patients were IMDC intermediate risk or high risk and 67.5% were treatment naïve. About 2/3 of the patients were men and about 82% of patients were white. Of note, this is a young population of patients – the median age was 43.8 in HLRCC cohort and 57.1 in the sporadic cohort.
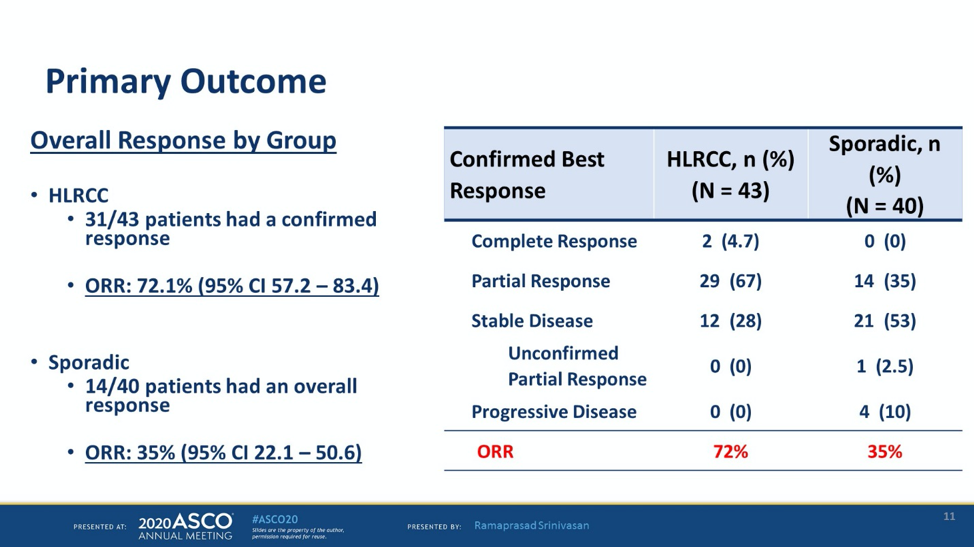
The primary endpoint of the study was the objective response rate. The objective response rate was 54% in all patients. For patients with HLRCC, the ORR was 72% and for patients with sporadic papillary RCC, the ORR was 35%. The objective response rates were independent of IMDC risk group or prior therapy.
The waterfall plot below shows that almost all patients with HLRCC had a decrease in tumor burden. 80% of patients with sporadic pRCC had tumor shrinkage as well.

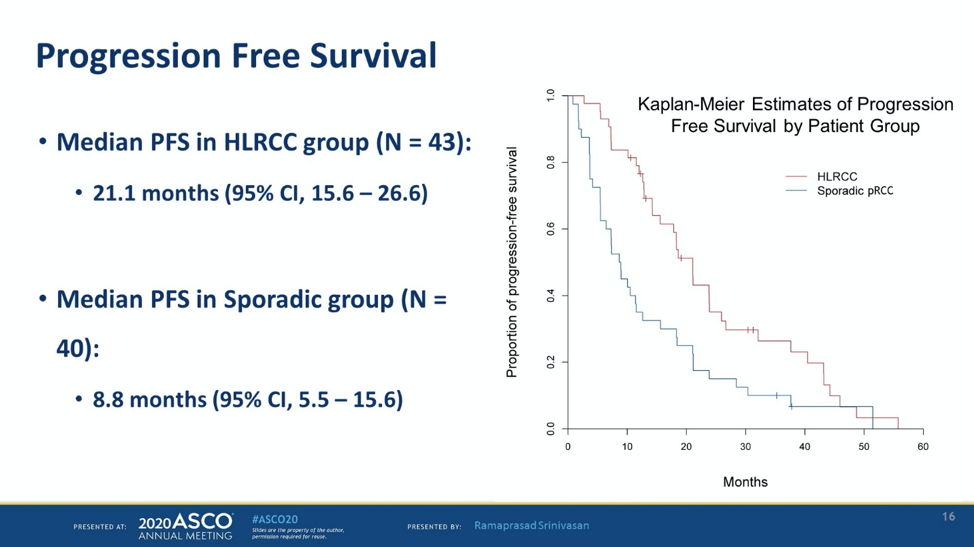
The responses were rapid and durable. The median time to response was 1.8 months and the median duration of response was 19.3 months for HLRCC and 17.5 months for sporadic PRCC. The median PFS for HLRCC was 21.1 months and 8.8 months in the sporadic group.
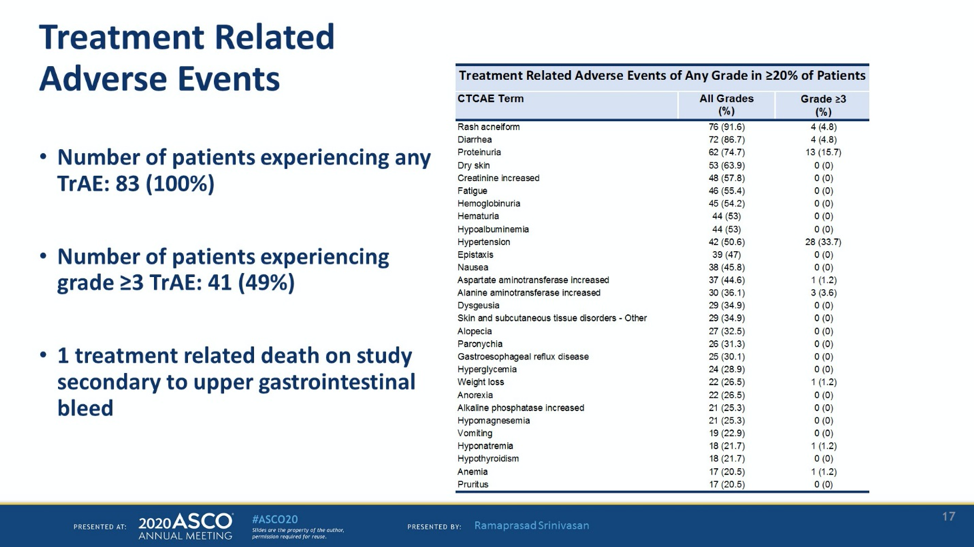
In terms of toxicity, the most common treatment related adverse events were rash (92%), diarrhea (77%), proteinuria (71%), and dry skin (61%). One patient had a grade 5 GI bleeding, possibly secondary to bevacizumab.
This is the largest prospective study of patients with HLRCC, and shows that the combination of bevacizumab and erlotinib is very active for patients with papillary RCC, especially those with FH deficiency. For patients who respond, especially those with HLRCC, the responses are durable with a median PFS of 21.1 months.
Presented by: Ramaprasad Srinivasan, MD, PhD, Center for Cancer Research, National Cancer Institute, Bethesda, MD
Written by: Jason Zhu, MD. Medical Oncologist, Division of Genitourinary Cancers, Levine Cancer Institute Twitter: @TheRealJasonZhu at the 2020 ASCO Annual Meeting, Virtual Scientific Program #ASCO20, May 29-31, 2020.
References:
- Menko FH, Maher ER, Schmidt LS, et al. Hereditary leiomyomatosis and renal cell cancer (HLRCC): renal cancer risk, surveillance and treatment. Familial cancer 2014;13:637-44.
Clinical Trial Information: NCT01130519