(UroToday.com) In this presentation, Elizabeth Plimack, MD, discussed the findings from LBA1, a phase 3 randomized study of maintenance avelumab in advanced urothelial cancer patients who have not progressed with first-line platinum-based chemotherapy.
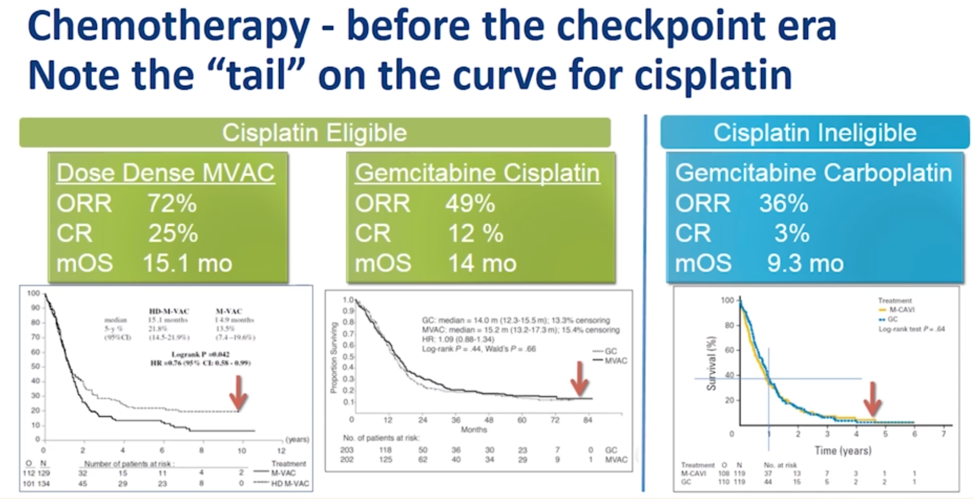
First, Dr. Plimack described the landscape of therapies for metastatic urothelial cancers. After the emergence of cisplatin in the late 1970s, there was a paucity of new therapies until 2008 when the efficacy of gemcitabine was demonstrated in this disease. Since 2016, multiple new therapies have been approved including immune checkpoint blockade (ICB), erdafitinib, and enfortumab vedotin. Cisplatin, however, remains the first-line standard of care for patients who can tolerate it, and can result in a durable response for a small subset of patients with advanced disease, as illustrated below.
As described in LBA1, the JAVELIN Bladder 100 trial recruited 700 patients treated with induction gemcitabine + platinum (cisplatin or carboplatin) who had either stable disease, partial response, or complete response and tolerated at least 4 cycles of induction therapy. Within 4-10 weeks of completion of chemotherapy, patients were randomized to either q2w maintenance avelumab or best supportive care. There was no placebo treatment, and no crossover was allowed.
Dr. Plimack first noted that the avelumab maintenance arm patients demonstrated the longest median overall survival (21.4 months) of any metastatic urothelial cancer trial population.
Dr. Plimack noted that in this trial, approximately half of the patients were PD-L1 positive, which is a higher positivity rate than prior avelumab or other immune-checkpoint trials in urothelial cancer. PD-L1+ patients in both arms had numerically longer overall survival compared to PD-L1 negative patients. 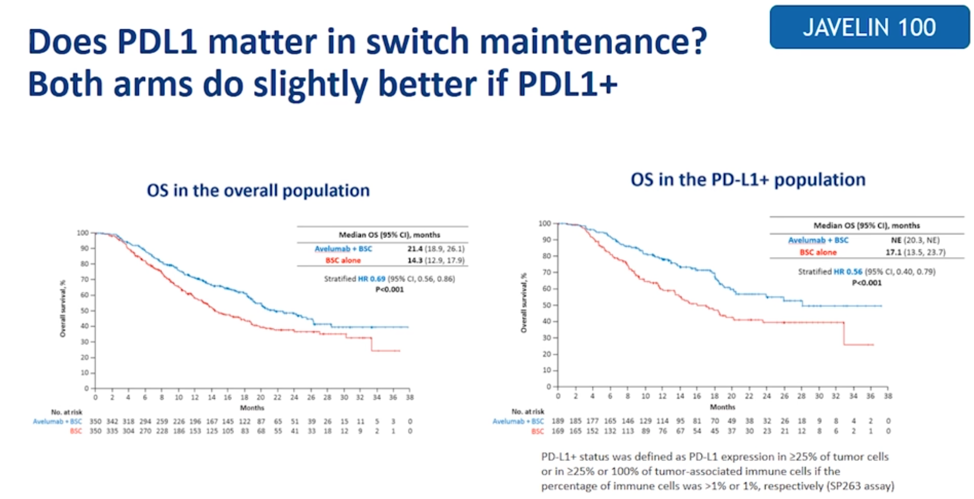
Dr. Plimack argued that the presented confirmed objective response rate data is difficult to interpret as most patients on trial already responded to chemotherapy and the benefit of this trial is focused on the maintenance of that response.
To further frame the data from this trial, Dr. Plimack compared the JAVELIN data to another trial of ICB maintenance therapy, the HCRN GU14-182 trial, the schema of which is shown below.
This phase 2 trial enrolled patients who had stable disease after 1-8 cycles of platinum-based induction therapy to either placebo or maintenance pembrolizumab. Crossover was allowed, and 52% of patients crossed over to receive pembrolizumab as essentially second-line post-chemotherapy ICB treatment. In essence, the control arm of this trial could be viewed as a “treatment break” study arm. This trial demonstrated a progression-free survival advantage, but no overall survival advantage to maintenance pembrolizumab. Dr. Plimack noted that approximately the same number of patients in the best supportive care arm on JAVELIN Bladder 100 received second-line ICB therapy.
So, what are the factors that may explain the different overall survival results between the HCRN trial and JAVELIN Bladder 100? Dr. Plimack noted that crossover was not allowed in JAVELIN Bladder 100, and indeed the control arm in JAVELIN Bladder had a lower numerical median OS compared to the HCRN trial. JAVELIN Bladder also included patients treated internationally, which could lead to differences in how second-line therapy was administered and handled. 
Dr. Plimack then asked the question of, post-platinum, is switch maintenance ICB preferred over a treatment break then second line therapy? Putting the JAVELIN Bladder 100 trial in context, Dr. Plimack showed the following slide suggesting that most patients who respond to chemotherapy should receive maintenance avelumab. She also mentioned that other data do suggest that the same patients that derive benefit from platinum chemotherapy generally derive benefit from ICB.

She stated that avelumab maintenance has a longer overall survival, confers a progression-free survival that is meaningful if progression is symptomatic, and may help patients that otherwise might not receive or respond to ICB as second-line therapy. However, maintenance therapy may over-treat patients who have durable responses to induction platinum chemotherapy, so it will be important moving forward to work to identify which patients are either likely to have a durable response to platinum induction therapy or respond well to second-line ICB.
In summary, Dr. Plimack stated that the JAVELIN Bladder 100 trial confirms that to date, platinum-based chemotherapy remains the most effective first-line treatment option for advanced urothelial cancers, and that offers the paradigm shift that switch maintenance with avelumab is preferred for patients who did not progress on initial chemotherapy. This maintenance therapy is associated with improved survival, delays progression of disease, and ensures that patients who are likely to have a response to ICB therapy are more likely to actually receive it.
Presented by: Elizabeth Plimack, MD, Chief of Genitourinary Oncology and Professor, Fox Chase Cancer Center, Philadelphia, PA
Written by: Alok Tewari, MD, Ph.D., Medical Oncology Fellow at the Dana-Farber Cancer Institute, at the 2020 ASCO Annual Meeting, Virtual Scientific Program #ASCO20, May 29-31, 2020.
Related Content:
Read: ASCO 2020: JAVELIN Bladder 100 Phase III Results: Maintenance Avelumab + Best Supportive Case vs BSC Alone After Platinum-Based First-Line Chemotherapy in Advanced Urothelial Carcinoma
View: JAVELIN Bladder 100: Avelumab for Previously Untreated Locally Advanced or Metastatic Urothelial Carcinoma - Thomas Powles