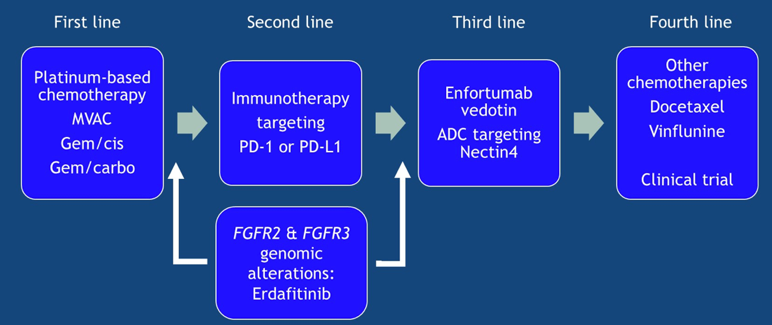
(UroToday.com) The kidney and bladder cancer poster discussion at the ASCO 2020 virtual annual meeting included a discussion presentation by Tian Zhang, MD, from the Duke Cancer Institute discussing single-agent targeted agents versus combinations with immunotherapy for patients with advanced urothelial cancer. The treatment landscape in metastatic urothelial carcinoma is rapidly evolving. In January 2019, first-line therapy included platinum-based chemotherapy, second-line therapy was immunotherapy, and third-line was other chemotherapies (ie. docetaxel or vinflunine) or a clinical trial. In April 2019, the second line therapy space expanded to include erdafitinib for patients with FGFR2 and FGFR3 genomic alterations. As of December 2019, enfortumab vedotin has taken over the third-line setting, as is shown in this schematic figure:
Dr. Zhang notes that the FGFR pathway is a powerful oncogenic driver in urothelial cancer, with FGFR mutations/translocations present in 15-20% of urothelial cancers. These alterations are more commonly seen in luminal-papillary subtypes of tumors, enriched in up to 50% of upper tract urothelial cancers, lack T-cell infiltration, and are less immunotherapy responsive. Erdafitinib gained accelerated approval by the US FDA in April 2019 for metastatic urothelial carcinoma with FGFR alterations,1 marking the first molecularly actionable target in metastatic urothelial carcinoma. Impressively, 76% of patients treated with 8 mg continuous erdafitinib had a reduction in the sum of target lesion diameters.
At this meeting, Alrene Siefker-Radtke, MD, presented long-term outcomes of the pivotal phase 2 BLC2001 trial testing erdafitinib in patients with metastatic urothelial carcinoma. The trial design for BLC2001 is as follows: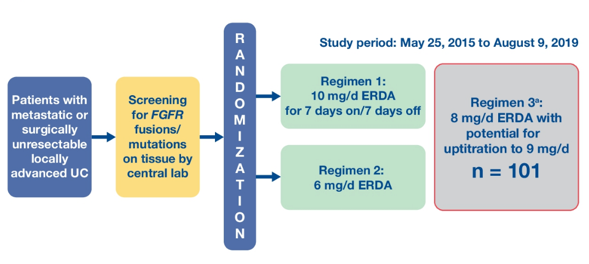
Of note, 88% of patients had progressed or relapsed on chemotherapy, 24% had received prior immunotherapy, and 43% of patients had received at least two or more lines of prior therapy. Furthermore, 77% of patients had visceral metastasis and 25% of patients had upper tract urothelial primary tumors. At a median follow-up of 24 months, the objective response rate in the entire cohort was 40% (95% CI 30-49%), for those with chemo-refractory disease was 39% (95% CI 29-50%), and the median duration of treatment was 6.0 months (95% CI 4.2-7.5 months). Additionally, in the overall cohort, the median PFS was 5.5 months (95% CI 4.0-6.0 months), and median OS was 11.3 months (95% CI 9.7-15.2 months):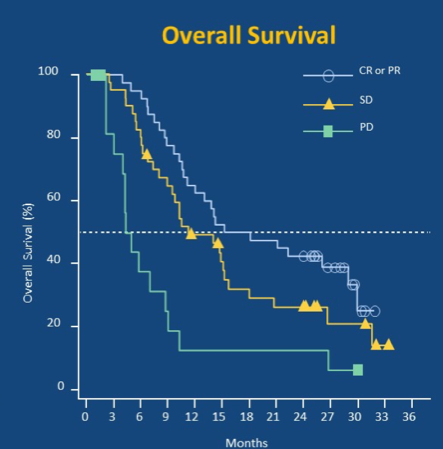
Regarding toxicity, 16% of patients had treatment discontinuation secondary to adverse events, with 27% of patients having serous retinopathy. Dr. Zhang notes that this trial does change the standard of care and has changed practice to routine genomic testing for patient selection. The strengths of this study are the significant responses in the chemo-refractory population with visceral disease, and 31% of patients with durable responses of more than one year, which is clinically meaningful. The caveat of this study, according to Dr. Zhang, is that this a single cohort phase 2 study, with several ongoing studies:
- THOR: phase 3 randomizing erdafitinib vs pembrolizumab vs chemotherapy
- NORSE: ongoing phase 2 randomizing erdafitinib vs erdafitinib + cetrelimab
- THOR2: phase 2 monotherapy vs intravesical chemotherapy in non-muscle invasive bladder cancer
Given that FGFR upregulated tumors have T-cell depletion through suppressed IFN-gamma signaling, Dr. Zhang suggests that this warrants combination approaches of FGFR and PD-1 inhibition.
The next abstract Dr. Zhang discussed was the FORT-2 phase Ib/II study assessing rogaratinib in combination with atezolizumab for first-line treatment in cisplatin-ineligible patients with metastatic urothelial carcinoma and FGFR mRNA overexpression. The trial schema for FORT-2 is as follows:
Dr. Zhang highlighted that treatment discontinuation secondary to adverse events was 55% for patients receiving rogaratinib 800 mg BID, but this decreased to only 15% of patients receiving 600 mg BID. As such, the recommended phase 2 dose is rogaratinib 600 mg PO BID and atezolizumab 1200 mg IV q3 weeks. In terms of efficacy, the objective response rate was 44%, the disease control rate was 68%, and three patients had a complete response. Importantly, among three patients with detectable resistance mutations in PI3K, there was no objective response. According to Dr. Zhang, this trial does not currently change the standard of care, however, the strengths are that it builds on strong pre-clinical data linking FGFR activation and T-cell depletion in the microenvironment. It also showed that objective response rates were higher than rogaratinib or atezolizumab monotherapy. This study is ongoing with the expansion cohort currently enrolling for FORT-2.
The final abstract discussed by Dr. Zhang is the COSMIC-021 study assessing cabozantinib in combination with atezolizumab for patients with urothelial carcinoma previously treated with platinum chemotherapy presented by Dr. Monty Pal and colleagues. The combinations of cabozantinib + atezolizumab, as well as cabozantinib + nivolumab, have previously shown early efficacy in other tumor types, including mCRPC, non-small cell lung cancer, and renal cell carcinoma. The trial design for cohort 2 of the COSMIC-021 trial is as follows: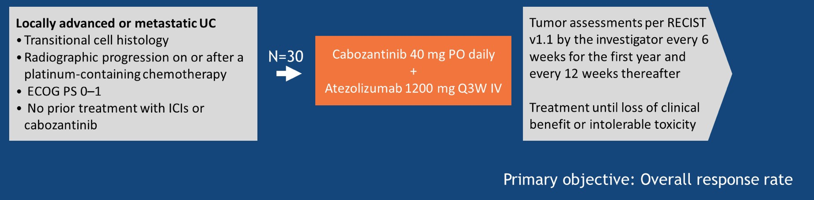
Among these 30 patients, 27% had liver metastasis, 40% had lung metastasis, and 27% had bone metastasis. Furthermore, 43% had received two or more prior systematic therapies. The objective response rate for these patients was 27%, with 2 complete responses and a disease control rate of 63%. The median duration of response was not reached, with the longest >15 months, and the median PFS was 5.4 months. The most common adverse events were asthenia (37% grade 3) and diarrhea (27% grade 1-2). There were 30% of patients that had dose reductions in cabozantinib, and there were no instances of discontinuation of both cabozantinib and atezolizumab. According to Dr. Zhang, this trial does not yet change the standard of care but notes that the cabozantinib-atezolizumab combination is active with an ORR of 27%, better than the 13% for atezolizumab in IMvigor 211 [2]. Looking ahead, three other metastatic urothelial carcinoma cohorts are enrolling in COSMIC-021, including first-line cisplatin-ineligible, first-line cisplatin eligible, and patients that have previously received immunotherapy. What we need in future trials is randomization against PD-1 monotherapy or chemotherapy to assess how much more benefit vs toxicity is associated with combination therapy.
Presented by: Tian Zhang, MD, Duke Cancer Institute, Durham, NC
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md, at the 2020 ASCO Annual Meeting, Virtual Scientific Program #ASCO20, May 29-31, 2020.
References:
- Loriot Y, Necchi A, Park SH, et al. Erdafitinib in Locally Advanced or Metastatic Urothelial Carcinoma. N Engl J Med 2019 Jul 25;381(4):338-348.
- Powles T, Duran I, van der Heijden MS, et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): A multicentre, open-label, phase 3 randomized controlled trial. Lancet 2018;391:748-757.