Patients with metastatic urothelial carcinoma with no prior chemotherapy for metastatic disease and >12 months from prior (neo)adjuvant chemotherapy and ECOG PS 0-1 were randomized 1:1 to gemcitabine 1000 mg/m2 IV days 1 and 8 and cisplatin IV 70 mg/m2 day 1 with bevacizumab (GCB) 15 mg/kg IV or placebo (GCP) day 1 every 21 days. Randomization was stratified by the presence of visceral metastases and prior chemotherapy. The primary endpoint was OS defined as the time from randomization to death or last follow-up. Secondary endpoints included progression-free survival (PFS), objective response rate (ORR), and ≥ grade 3 toxicity. With 445 deaths, the log-rank test had an 87% power to detect a hazard ratio (HR) of 0.74 with a 2-sided α=0.05. A schema of the trial is as follows:

Dr. Rosenberg concluded his presentation of CALGB 90601 with several concluding statements:
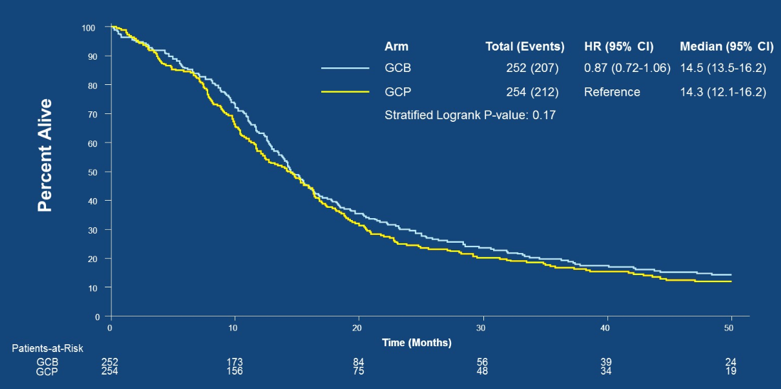
- The addition of bevacizumab did not improve overall survival when added to gemcitabine and cisplatin chemotherapy as first-line therapy for metastatic urothelial carcinoma
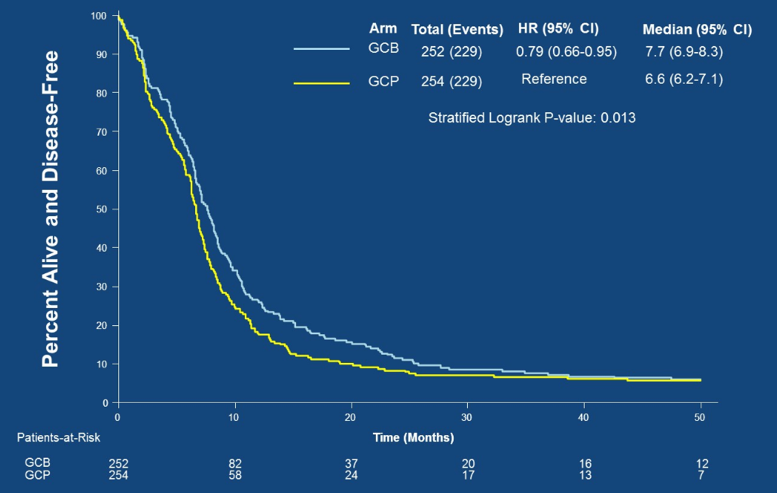
- However, the addition of bevacizumab did improve PFS although the improvement of 1.1 months was not clinically significant
- Toxicity of the GCB combination was comparable to historical data
- Currently, the standard of care remains cisplatin-based chemotherapy without the addition of biologic agents
- Ongoing correlative work may identify subsets of patients who may benefit from anti-angiogenic therapy
- This study shows the importance of confirming phase II results in phase III randomized trials – pretreatment prognostic factors can heavily influence outcomes in advanced urothelial carcinoma
- Although accrual took more than five years, it showed that the US could complete a large randomized phase III trial in mUC
Presented by: Jonathan E. Rosenberg, Memorial Sloan Kettering Cancer Center, New York, NY
Co-Authors: Karla V. Ballman, Susan Halabi, Colleen Watt, Olwen Mary Hahn, Preston D. Steen, Robert Dreicer, Thomas W. Flaig, Walter Michael Stadler, Christopher Sweeney, Amir Mortazavi, Michael J. Morris; Memorial Sloan Kettering Cancer Center, New York, NY; Weill Cornell Medicine, New York, NY; Duke University Medical Center, Durham, NC; University of Chicago, Chicago, IL; University of Chicago Medical Center, Chicago, IL; Roger Maris Cancer Center, Fargo, ND; Cleveland Clinic, Cleveland, OH; Division of Medical Oncology, School of Medicine, University of Colorado, Aurora, CO; Lank Center for Genitourinary Oncology, Dana-Farber Cancer Institute, Boston, MA; Arthur G. James Cancer Hospital, Ohio State University Wexner Medical Center, Columbus, OH
Written By: Zachary Klaassen, MD, MSc, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md at the 2019 ASCO Annual Meeting #ASCO19, May 31- June 4, 2019, Chicago, IL USA
References:
- Bellmunt J, Gonzalez-Larriba JL, Prior C, et al. Phase II study of sunitinib as first-line treatment of urothelial cancer patients ineligible to receive cisplatin-based chemotherapy: baseline interleukin-8 and tumor contrast enhancement as potential predictive factors of activity. Ann Oncol 2011;22(12):2646-2653.
- Hahn NM, Stadler WM, Zon RT, et al. Phase II trial of cisplatin, gemcitabine, and bevacizumab as first-line therapy for metastatic urothelial carcinoma: Hoosier Oncology Group GU 04-75. J Clin Oncol 2011;29(12):1525-1530.
- Balar AV, Apolo AB, Ostrovnaya, et al. Phase II study of gemcitabine, carboplatin, and bevacizumab in patients with advanced unresectable or metastatic urothelial cancer. J Clin Oncol 2013;31(6);724-730.