Dr. Lorch continued to give an extended overview of 1st line salvage therapy in patients with refractory GCTs. The conventional dose regimen includes either VIP (cisplatin, Ifosfamide, etoposide), VeIP (cisplatin, Ifosfamide, vinblastine), or TIP (cisplatin, Ifosfamide, paclitaxel) chemotherapy, repeated every 21 days for 4 cycles. TIP as 1st line salvage therapy has been shown to have a 63% durable complete response with 2 years progression-free survival (PFS) of 65% (95% CI 51-79%).[1]
High-dose regimens include the combination of Carboplatin and etoposide, at varying dosages according to the protocol used (Indiana, German germ cell cancer group [GTCSG], and Memorial [MSKCC]). The Indiana protocol demonstrated 63% of the patients being disease free at a median follow-up of 48 months, with 90% of the patients being disease free at 2 years.[2] The GTCSG protocol demonstrated a 5 years PFS of 47%.[3] Lastly, the MSKCC protocol demonstrated 5-year disease-free survival of 47% and 5-year overall survival of 52%.[4]
Dr. Lorch continued to discuss the problems with prognostic factor analyses in refractory GCTs. These included the fact the studies published on these patients usually have small number of patients, usually from a single center. Not all patients received standard 1st line treatment, and some had inaccurate staging with outdated regimens. Many times, the cohorts are mixed with 1st and 2nd line salvage therapies. Moreover, many times the salvage treatment that patients received is inadequate.
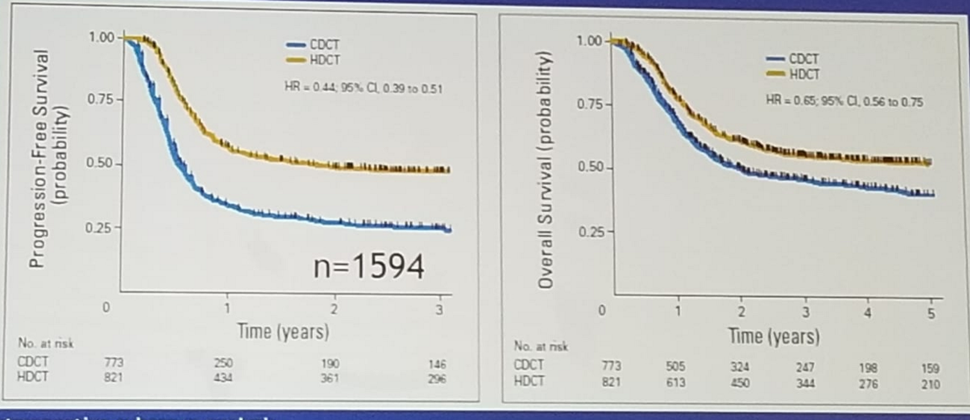
In 2010 a multicenter study with multinational participation from Europe, USA, and Canada that analyzed 1594 patients treated between 1990-2007 with 1st line salvage therapy, was published in the Journal of Clinical Oncology. [5] This was a retrospective study analyzing patients that received 1st line salvage therapy, both conventional and high dose. This study demonstrated a clear advantage in PFS and overall survival for high dose chemotherapy over conventional dose (Figure 1).
Figure 1 – Advantage in PFS and overall survival of high dose over conventional dose chemotherapy:
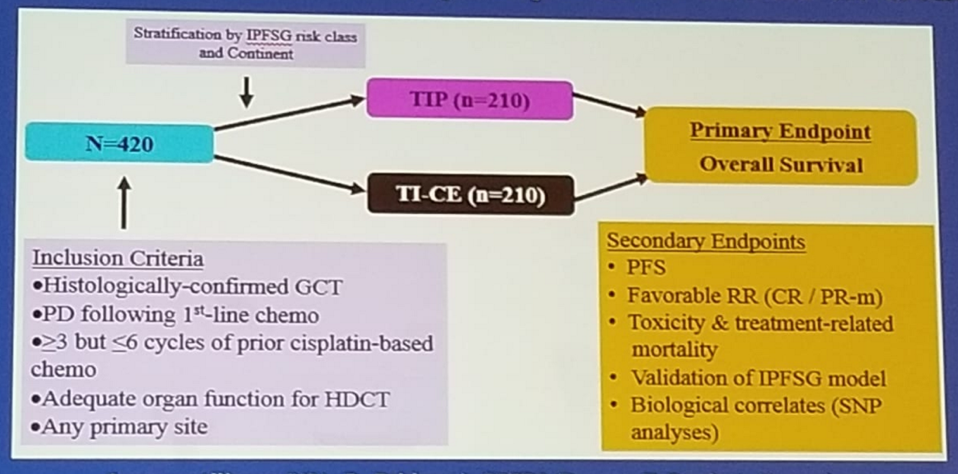
Dr. Lorch moved on with her presentation to present the new and relevant TIGER study (Figure 2). This is a randomized phase 3 trial comparing conventional-dose chemotherapy using TIP with high-dose chemotherapy using TI-CE (paclitaxel plus ifosfamide followed by high-dose carboplatin plus etoposide with stem-cell support), as first salvage treatment in relapsed or refractory GCTs.
Figure 2 -The TIGER study design:
Dr. Lorch discussed briefly the role of surgery in these patients. Salvage surgery rather than salvage chemotherapy is warranted in patients with growing teratoma syndrome, resectable late relapse GCT, and as desperation surgery. Resection of all residual detectable tumor in nonseminoma tumors is mandatory for treatment and long-term survival. The proportion of viable cancer in the specimen of these patients in this specific setting is approximately 70%.
Dr. Lorch concluded her informative talk by stating that future directions include focusing on targeted therapies, including tyrosine kinase inhibitors, checkpoint inhibitors, and others. Most published studies assessing these targeted agents have been negative.
In conclusion, when dealing with patients with refractory GCTs, it is critical that we first identify patients who will not need salvage chemotherapy (growing teratoma syndrome, resectable “late” relapses). Sequential high dose carboplatin and etoposide is the most frequently used regimen outside of clinical trials with acceptable toxicity. The TIGER trial will be the 1st prospective study assessing whether conventional dose chemotherapy or high dose chemotherapy, as 1st line therapy, is superior. Importantly high dose chemotherapy can cure refractory resistant GCTs, even when given as 2nd line salvage therapy. Achieving a state of complete resection of all residual tumor is paramount for treatment success. So far, there has been no proven role for targeted therapies, such as immune checkpoint inhibitors for these patients. However, there are currently several phase 1/2 trials that are underway. Lastly, relapsing/refractory patients should be referred to experts at clinical centers of excellence.
References:
1. Kondagunta et al. JCO 2005
2. Einhorn et al. NEJM 2007
3. Lorch et al. JCO 2007, and 2012
4. Feldman et al. JCO 2010
5. The international prognostic factor study group. JCO 2010
Presented by: Anja Lorch, MD, Dusseldorf, Germany
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter: @GoldbergHanan at the 2018 ASCO Annual Meeting - June 1-5, 2018 – Chicago, IL USA