In this talk, Dr. Feldman reviewed some common and important principles and pitfalls in diagnosis and workup, early-stage disease, and advanced disease.
He began with the 1st principle stating that the main differential diagnosis for GCT is epididymo-orchitis. In this stage, it is appropriate to order an US or even attempt a trial of antibiotics/NSAIDS. However, it is critical to make sure that the patient comes back for follow-up within two weeks. Once the diagnosis of GCT is made, staging must be performed with serum tumor markers, and CT scans of the chest, abdomen, and pelvis. At this stage, there is no role for PET scans. Before any kind of active treatment, sperm banking must be offered, as all therapeutic options in post-orchiectomy patients carry a risk of infertility.
Another important principle mentioned is the usage of post-orchiectomy markers instead of using pre-orchiectomy markers. This can cause either over or under-treatment. It is important to know the half-life (t1/2) of HCG (1-3 days) and AFP (5-7 days). Furthermore, when HCG levels are extremely high at the time of diagnosis, normalization does not usually happen immediately and takes time after chemotherapy. There can be a slow terminal rate of decline. Therefore, it is prudent not to assume treatment failure for a slowly declining HCG level. Also, we should never forget that elevated serum tumor markers have false positive causes, potentially causing over treatment. However, most of these false positive causes result in serum tumor markers fluctuating or remaining constant. For HCG these include:
- Hypogonadism
- LH cross-reactivity with test for B-HCG
- Pituitary secretion of HCG in response to low testosterone levels
- Marijuana
- Heterophile antibodies
- Change in upper normal limit from 15 to 6-8 in many labs (for some patients a level of 6-15 is considered normal)
- Liver inflammation/injury (hepatitis, alcohol, steatohepatitis)
- Hereditary persistence of AFP
Dr. Feldman continued to discuss the management of neutropenia caused by every cycle of BEP chemotherapy. An important pitfall is omitting week 3 bleomycin or delaying chemotherapy for mid/recovering neutropenia. According to the MSKCC approach, only if WBC<2500 and ANC <500, should chemotherapy be delayed by 1 week. Otherwise, treatment should continue without any delays or dose reductions. Additionally, G-CSF can be used for support in future cycles.
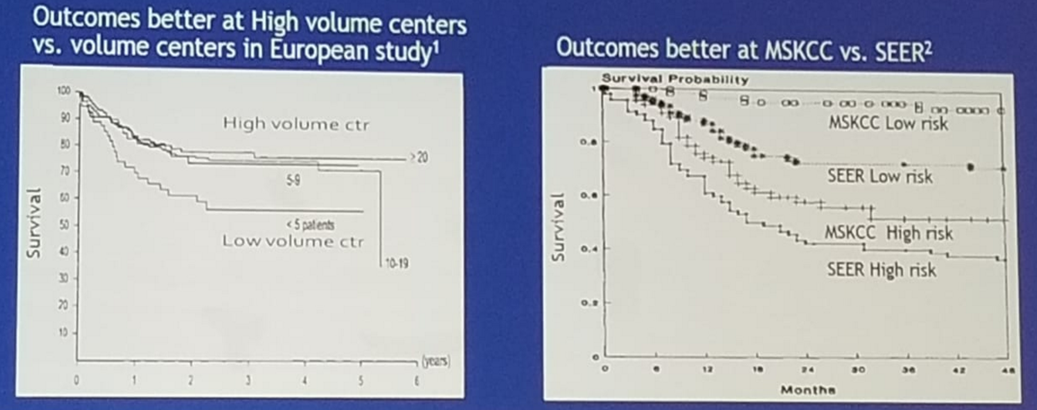
Lastly, Dr. Feldman mentioned the importance of referral of complicated GCT cases to centers of excellence. These cases usually require experience and expertise. There is data demonstrating outcomes at high volume centers being better when compared to lower volume centers (Figure 1).[1,2] Furthermore, the guidelines must be adhered to, as this adherence causes better relapse-free survival.
Figure 1 – Better outcomes of GCTs at centers of excellence:
In conclusion, avoiding common pitfalls will improve outcomes. Mildly enlarging retroperitoneal node may not be due to metastatic disease, and therefore imaging must be repeated before treatment. Post-orchiectomy markers are the ones that should be used, and not pre-orchiectomy markers. Elevated markers can have false positive causes that need to be considered. The half-life of markers must be considered before deciding on any treatment strategy. Dose reductions in neutropenia should be avoided, and lastly, referral of complex cases to centers of excellence is always the right move.
References:
1. Feuer et al. JCO 1983
2. Collete et al. JNCI 1999
Presented by: Darren Feldman, MD, Memorial Sloan Kettering Cancer Center, New York, USA
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter: @GoldbergHanan at the 2018 ASCO Annual Meeting - June 1-5, 2018 – Chicago, IL USA