Patients with metastatic castration-resistant prostate cancer (mCRPC) who have homologous recombination repair mutation (HRRm) have been previously shown to have improved response to the PARP inhibitor olaparib (Lynparza) as monotherapy when compared to men without a HRRm.2 Based on this, the authors of this study initiated an assessment of olaparib in combination with abiraterone (an androgen axis targeted therapy approved in this setting already) in men with mCRPC already previously treated with chemotherapy. The biologic rationale was that they would work synergistically – PARP inhibitors would affect AR dependent transcription while abiraterone would work on androgen synthesis.
This was a Phase II, placebo-controlled trial. Men with mCRPC previously treated with chemotherapy (docetaxel) were eligible regardless of HRRm status. Standard of care would be treatment with ARAT, specifically abiraterone.
Patients were randomized 1:1 to either arm A - olaparib 300 mg bid (tablets; combination with abiraterone) or arm B- placebo (comparator). All patients received abiraterone (1000 mg od). Patients were treated until disease progression.
Schema below:

The primary endpoint was investigator-assessed radiologic progression-free survival (rPFS; RECIST 1.1, PCWG-2). HRRm status was assessed using optional tumor (n = 68), whole-blood and plasma samples.
HRRm status was assessed in different ways for different patients, depending on availability of tissue:

They recruited 142 pts to the study and they were randomized 1:1 to each arm (both arms, n = 71). Baseline patient demographics are below:
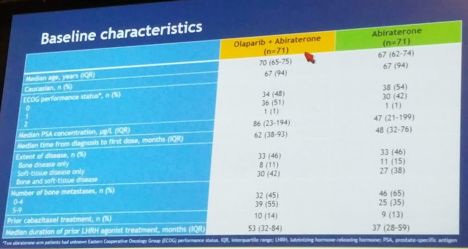
Despite randomization, the olaparib arm was older, had a higher median PSA (86 vs. 47) and higher volume bony metastatic disease (55% had 5-9 bone mets vs. 35%).
In terms of oncologic outcomes, there was a statistically significant increase in rPFS seen with the combination (13.8 months) vs abiraterone alone (8.2 month), a 5.5 month PFS beneifit (HR 0.65, P= 0.03). As seen below, HRRm status did not seem to impact this benefit:

Median overall survival was 22.7 vs 20.9 months in the combination vs AA alone arms, respectively (HR 0.91, p=0.66).
When looking at objective response, most of the benefit seemed to come from shifting patients from progressive disease to stable disease. There were no complete responses in either arm. Partial responses were similar in both arms (~27-32%).
In terms of tolerability, adding olaparib increased the AE profile: 54% vs 28% of pts, respectively, had grade ≥3 AEs; 34% vs 18% reported serious AEs, including more cardiovascular AEs with the combination. Treatment related deaths was seen in 6% vs. 1% of each arm. Anemia, which is a known effect of PARP inhibitors, was significantly higher in the olaparib arm. 30% vs 10% of pts, respectively, discontinued treatment due to an AE. Based on AE, median time to deterioration in quality of life (QoL; FACT-P) was 5.7 vs 6.0 months, respectively (HR 0.97, not significantly different).
As the authors note, while the safety data was not as favorable for the combination, there was a significant PFS and survival benefit with adding a PARP inhibitor to SOC abiraterone therapy. This is the first study to show efficacy of PARP inhibitors independent of HRRm status.
A phase III study is already underway.
Presented by: Earle Frederick Burgess, MD
Written by: Thenappan Chandrasekar, MD, Clinical Fellow, University of Toronto, Twitter: @tchandra_uromd at the 2018 ASCO Annual Meeting - June 1-5, 2018 – Chicago, IL USA
References:
1. Pritchard CC, Mateo J, Walsh MF, De Sarkar N, Abida W, Beltran H, Garofalo A, Gulati R, Carreira S, Eeles R, Elemento O, Rubin MA, Robinson D, Lonigro R, Hussain M, Chinnaiyan A, Vinson J, Filipenko J, Garraway L, Taplin ME, AlDubayan S, Han GC, Beightol M, Morrissey C, Nghiem B, Cheng HH, Montgomery B, Walsh T, Casadei S, Berger M, Zhang L, Zehir A, Vijai J, Scher HI, Sawyers C, Schultz N, Kantoff PW, Solit D, Robson M, Van Allen EM, Offit K, de Bono J, Nelson PS. Inherited DNA-Repair Gene Mutations in Men with Metastatic Prostate Cancer. N Engl J Med. 2016 Aug 4;375(5):443-53. doi: 10.1056/NEJMoa1603144. Epub 2016 Jul 6.
2. Mateo J, Carreira S, Sandhu S, Miranda S, Mossop H, Perez-Lopez R, Nava Rodrigues D, Robinson D, Omlin A, Tunariu N, Boysen G, Porta N, Flohr P, Gillman A, Figueiredo I, Paulding C, Seed G, Jain S, Ralph C, Protheroe A, Hussain S, Jones R, Elliott T, McGovern U, Bianchini D, Goodall J, Zafeiriou Z, Williamson CT, Ferraldeschi R, Riisnaes R, Ebbs B, Fowler G, Roda D, Yuan W, Wu YM, Cao X, Brough R, Pemberton H, A'Hern R, Swain A, Kunju LP, Eeles R, Attard G, Lord CJ, Ashworth A, Rubin MA, Knudsen KE, Feng FY, Chinnaiyan AM, Hall E, de Bono JS. DNA-Repair Defects and Olaparib in Metastatic Prostate Cancer. N Engl J Med. 2015 Oct 29;373(18):1697-708. doi: 10.1056/NEJMoa1506859.