(UroToday.com)The 2025 APCCC Diagnostics annual meeting featured a session on what we should know for PSMA radioligand therapy and a presentation by Dr. Louise Emmett discussing what to do in non-responding PSMA radioligand patients. Dr. Emmett emphasized that it is important to identify those patients that are unlikely to respond to PSMA radioligand therapy, which can be assessed using PSMA and FDG-PET, as well as ctDNA.
A post-hoc analysis from the TheraP trial assessed PSMA and FDG-PET as predictive and prognostic biomarkers in patients given 177Lu-PSMA-617 versus cabazitaxel for metastatic castration resistant prostate cancer (mCRPC).1 The odds of PSA response to 177Lu-PSMA-617 versus cabazitaxel were significantly higher for men with SUVmean of 10 or higher compared with those with SUVmean of less than 10 (OR 12.19, 95% CI 3.42-58.76 versus OR 2.22, 95% CI 1.11-4.51). Among the SUVmean >= 10 patients, 177Lu-PSMA-617 had significantly improved PSA progression free survival compared to cabazitaxel (HR 0.45, 95% CI 0.25-0.80), which was not the case for SUVmean <10 (HR 0.77, 95% CI 0.53-1.12):
At ASCO 2024, Kwon and colleagues presented results of ctDNA fraction as a predictor of treatment efficacy in the TheraP trial of 177Lu-PSMA-617 versus cabazitaxel. The odds of a PSA50 response to 177Lu-PSMA-617 versus cabazitaxel were significantly higher for men with ctDNA <2% (p = 0.0067), with no significant difference at ctDNA >30% (OR 1.1, 95% CI 0.42 - 2.8). The PSA50 and PSA90 response stratified by ctDNA% categories are depicted below:
With regards to intensifying treatment up front, how high can we go? Presented at ASCO 2019, Tagawa and colleagues assessed 56 men with mCRPC (no PSMA PET criteria for inclusion) in a dose escalation study, with a fractionated single dose of 177Lu-PSMA-617 at days 1 and 15, of which 27 of these 56 men received a maximum of 22 Gbq. Overall, 54% had a PSA50 response, the median PSA progression free survival was 5.6 months (95% CI 3.9 – 8.0 months), median radiographic progression free survival was 9.6 months (95% CI 5.6 – 14.9), and median overall survival was 15.2 months (95% CI 10.8 – 27). For adverse events, grade 1-2 thrombocytopenia was noted in 34% of patients and anemia in 20% (grade 3 anemia was 8%). On multivariable analysis, CALGB risk, prior chemotherapy, higher PSMA uptake, and dose were associated with overall survival.
As part of intensifying treatment up front, Dr. Emmett also highlighted biomarker-modulated PSMA theranostics (NCT0656299,) whereby low PSMA mCRPC patients are treatment intensified with 177Lu-PSMA-617: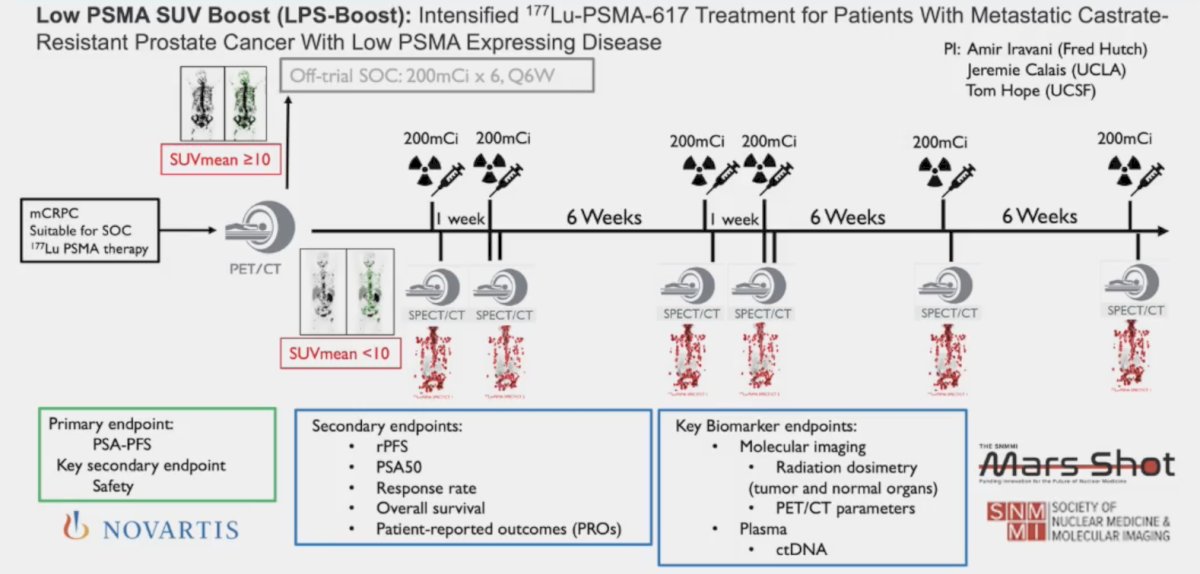
The ENZA-p trial included mCRPC patients not previously treated with chemotherapy or androgen receptor pathway inhibitors (prior abiraterone and/or docetaxel for hormone-sensitive disease were allowed), 68Ga-PSMA-positive disease on PET, and at least 2 risk factors associated with early progression on enzalutamide.2,3 In the enzalutamide + 177Lu-PSMA-617 arm, 81% of patients received four doses of 177Lu-PSMA-617. PSA50 and PSA90 improved with 177Lu-PSMA-617 + enzalutamide:![The ENZA-p trial included mCRPC patients not previously treated with chemotherapy or androgen receptor pathway inhibitors (prior abiraterone and/or docetaxel for hormone-sensitive disease were allowed), 68Ga-PSMA-positive disease on PET, and at least 2 risk factors associated with early progression on enzalutamide [2-3]. In the enzalutamide + 177Lu-PSMA-617 arm, 81% of patients received four doses of 177Lu-PSMA-617. PSA50 and PSA90 improved with 177Lu-PSMA-617 + enzalutamide](/images/com-doc-importer/194-apccc-diagnostics-2025/apccc-diagnostics-2025-what-to-do-in-non-responding-psma-rlt-patients/image-3.jpg)
Additionally, median overall survival was 34 versus 26 months for 177Lu-PSMA-617 + enzalutamide versus enzalutamide alone, with a 45% reduction in mortality (HR 0.55, 95% CI 0.36-0.84):3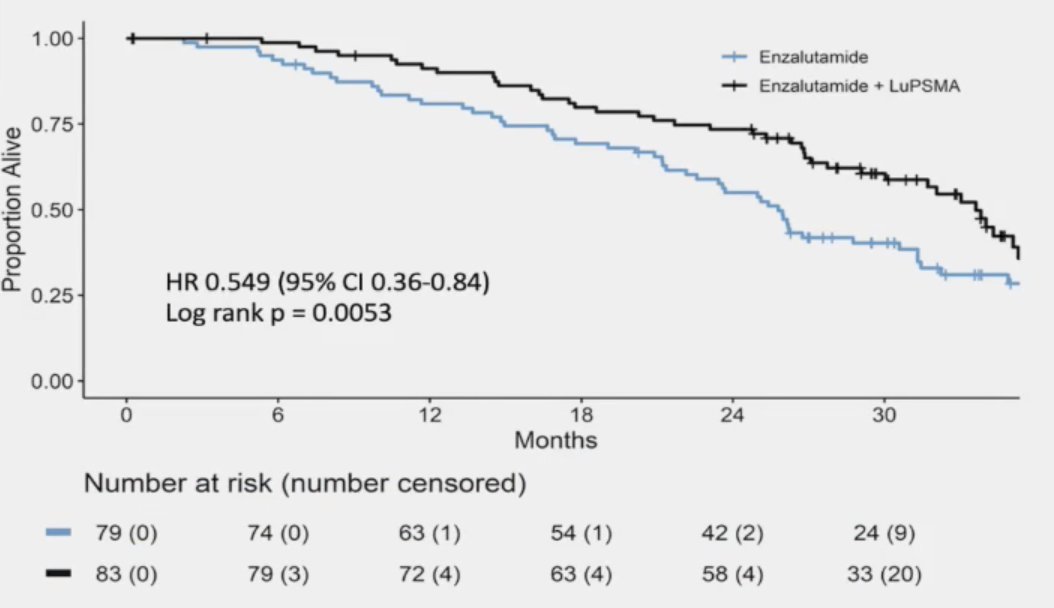
Recently presented at GU ASCO 2025, Yazdanpanah and colleagues presented a secondary analysis of the VISION trial4 assessing the efficacy of 177Lu-PSMA-617 with or without androgen receptor pathway inhibitors for the treatment of mCRPC. They found a statistically significant difference in median overall survival was observed in patients treated with concomitant androgen receptor pathway inhibitors versus those without (17.8 versus 12.4 months; HR 0.72; 95% CI 0.58–0.89; nominal p = 0.001): 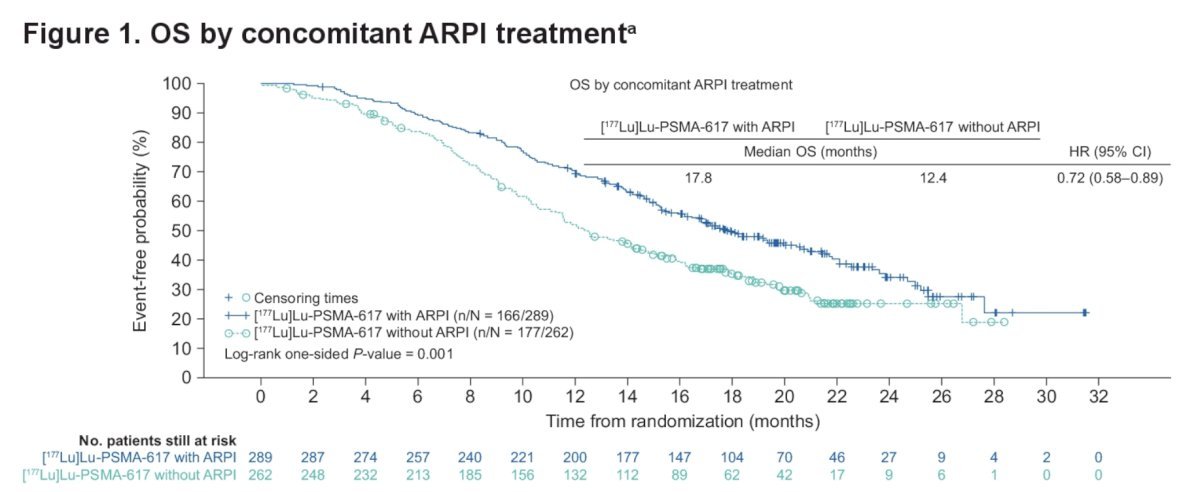
Intensification of upfront therapy may also include radium-223 + an androgen receptor pathway inhibitor, as noted in the PEACE III trial. The combination of enzalutamide + radium-223 (with 80% of overall survival events) showed an overall survival benefit for the combination therapy versus enzalutamide alone (median 42.3 months versus 35.0 months; HR 0.69, 95% CI 0.52-0.90):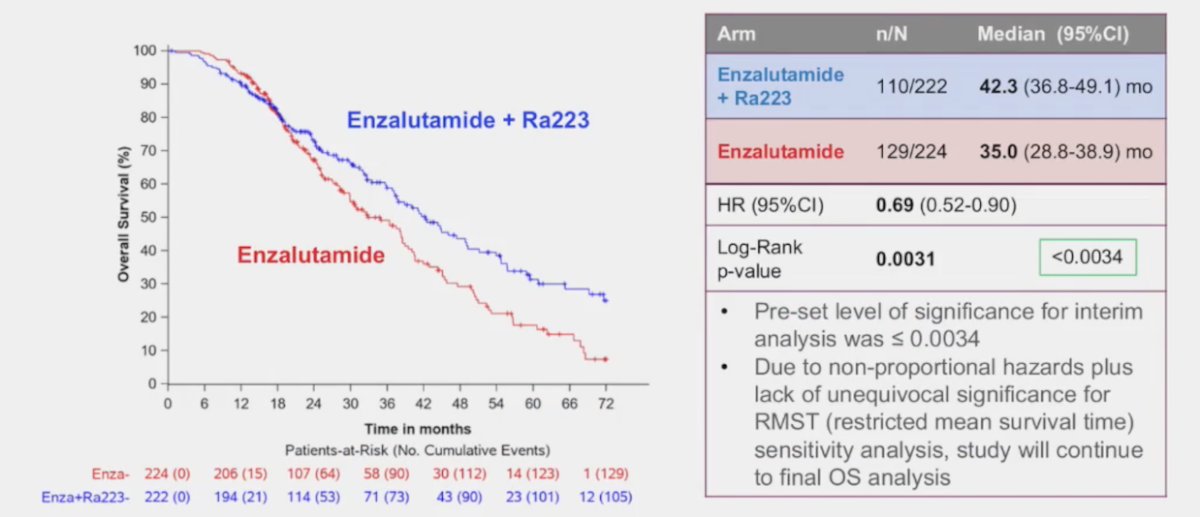
Although identifying radiation resistant disease is important, Dr. Emmett notes that Dr. Tom Hope suggests that everyone deserves 2 doses of 177Lu-PSMA-617. SPECT quantification offers a modality for more rapid assessment of radiation resistant disease. In an effort to assess response rates and adjust treatment appropriately John et al. [5] sought to evaluate change in 177Lu-PSMA SPECT quantitative parameters to monitor treatment response. Among 127 men with progressive mCRPC, at baseline and week 6, 76% had analyzable serial 177Lu-PSMA SPECT/CT imaging. SPECT total tumor volume was reduced between baseline and week 6 in 74% of patients. Any increase in SPECT total tumor volume between baseline and week 6 was associated with significantly shorter PSA progression free survival (HR 2.5, 95% CI, 1.5-4.2) but not overall survival. Thus, increasing PSMA SPECT total tumor volume on quantitative 177Lu-PSMA SPECT/CT predicted short progression-free survival and may play a future role as an imaging response biomarker, identifying when to cease or intensify 177Lu-PSMA therapy.
Demirci et al.6 have also assessed SPECT/CT in early response assessment of 66 patients with mCRPC receiving 177Lu-PSMA therapy. They found that changes in total tumor volume measured at the start of cycles 2 and 3 relative to baseline correlated significantly with corresponding changes in PSA level (r = 0.55 and 0.56), but absolute total tumor volumes did not correlate significantly (r = 0.00 and 0.18). Patients with a higher absolute total tumor volume at the start of cycle 2 had worse PSA progression-free survival and overall survival (HR 1.4, 95% CI, 1.1-1.8 and HR 2.1, 95% CI, 1.5-2.9; respectively), with consistent results at the start of cycle 3 (HR 2, 95% CI, 1.4-2.9 and HR 2, 95% CI, 1.2-3.2; respectively). New lesions were identified in 13 of 66 and 11 of 51 patients at the start of cycles 2 and 3, respectively. Moreover, new lesions at the start of cycle 2 were associated with worse overall survival (HR 5.8, 95% CI, 1.9-17.5), with consistent results at the start of cycle 3 (HR 4.9, 95% CI, 1.3-18.6):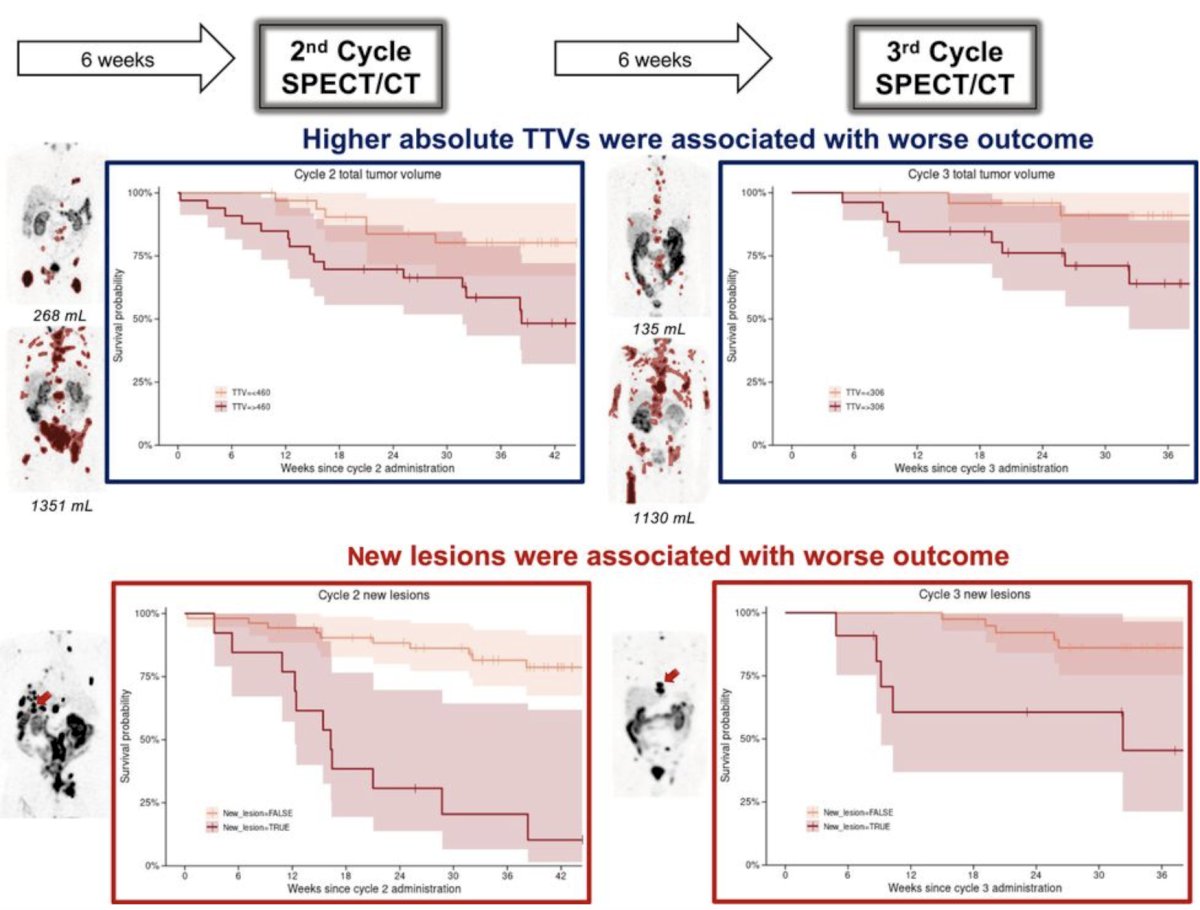
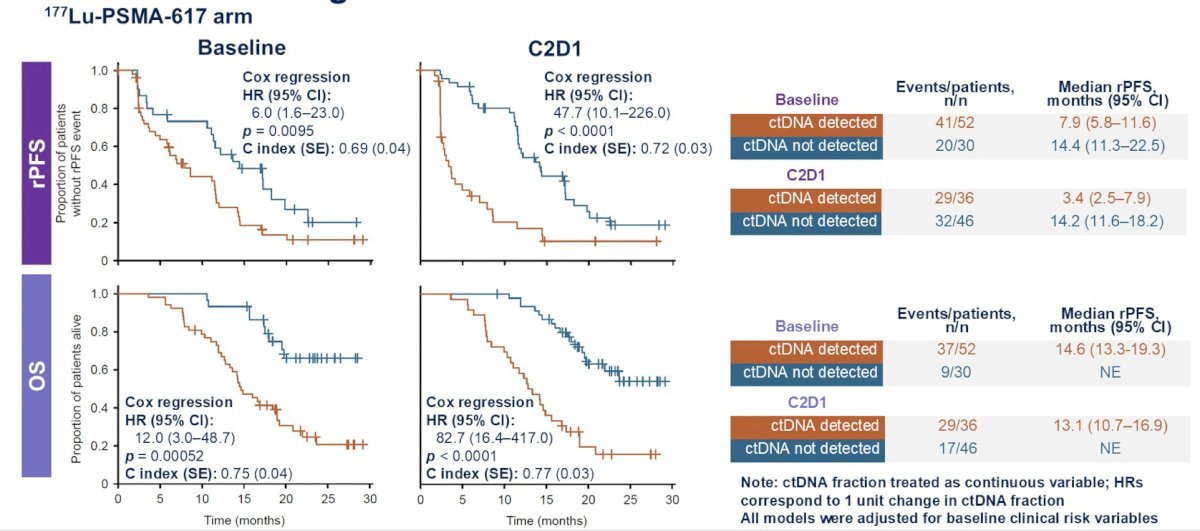
Presented recently at GU ASCO 2025, Dr. de Bono reported results assessing the association of baseline and on-treatment ctDNA fraction with clinical outcomes in patients with mCRPC in the PSMAfore trial.7 Patients with plasma samples at baseline and cycle 2 day 1 were included (177Lu-PSMA-617, 82/234; androgen receptor pathway inhibitor change, 91/234). Cox regression models adjusted for clinical features in the 177Lu-PSMA-617 arm showed that higher ctDNA fraction was associated with shorter radiographic progression free survival and overall survival. These associations were stronger for cycle 2 day 1 than baseline, both when comparing individual models and within a model including both time points:
Dr. Emmett notes that treatment intensification options for patients with (i) increasing PSMA volume or (ii) new lesions or (iii) a rise in PSA or (iv) PSMA negative expression currently include adding cabazitaxel, changing to an alpha therapy, or changing to radium-223: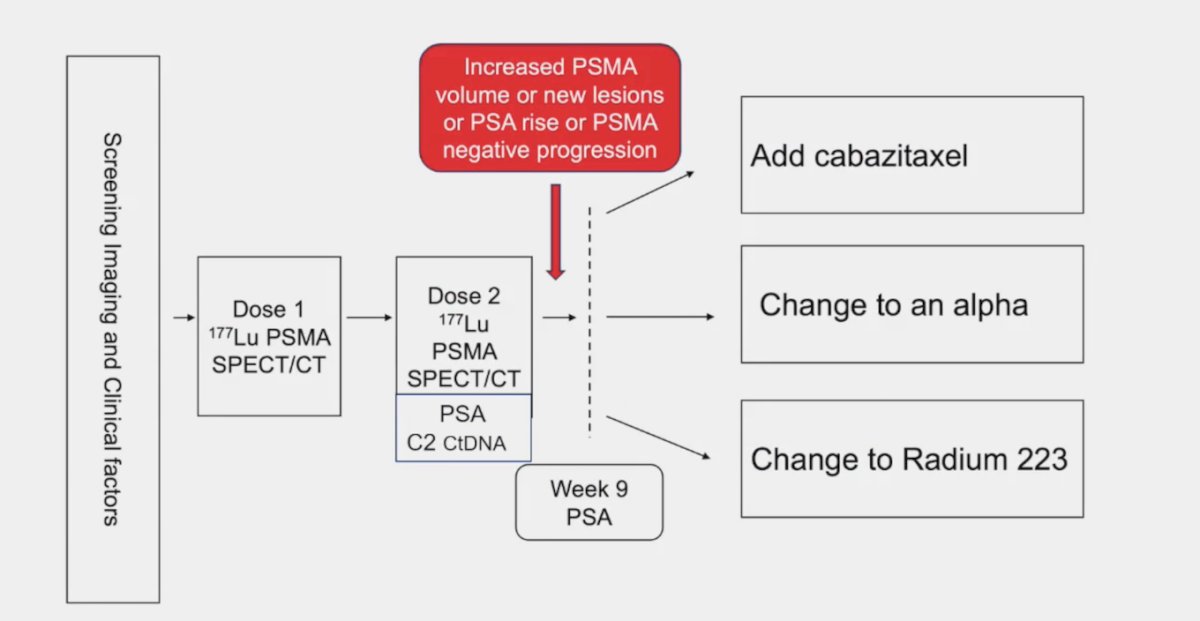
A trial assessing treatment intensification is the phase I/II LuCAB trial assessing the combination of cabazitaxel + 177Lu-PSMA-617 in mCRPC with a primary endpoint of maximum tolerated dose and recommended phase 2 dose: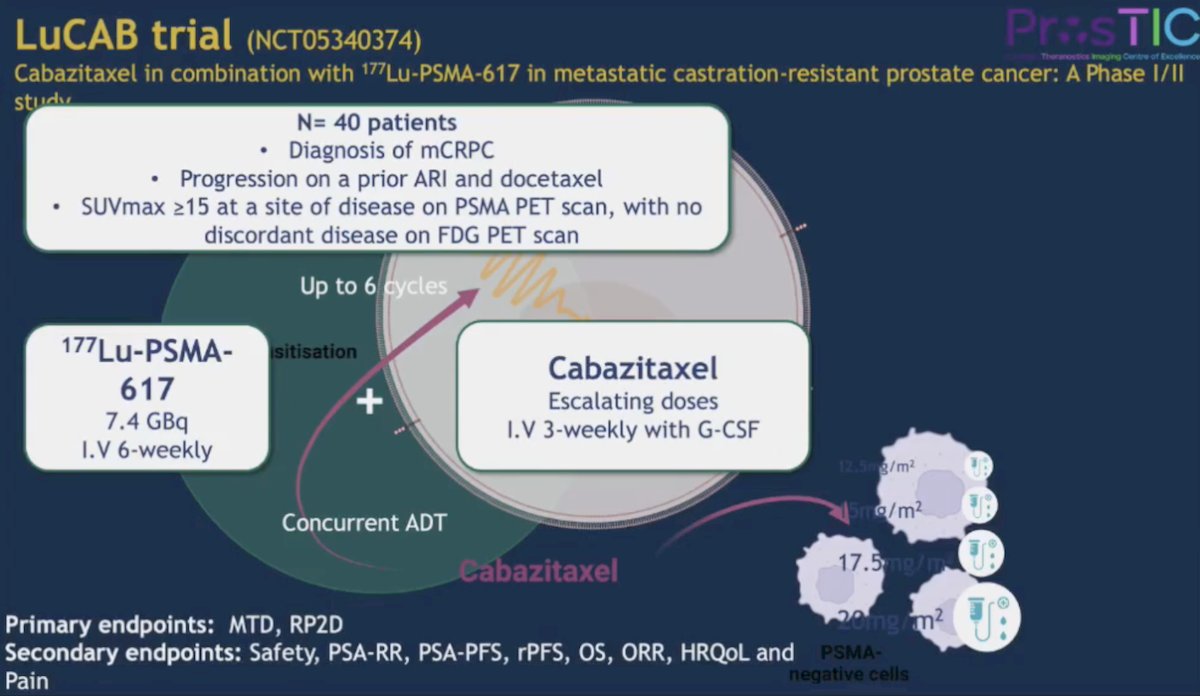
Other treatment intensification trials include the AcTION trial, which is a phase I trial of 225Ac PSMA-617: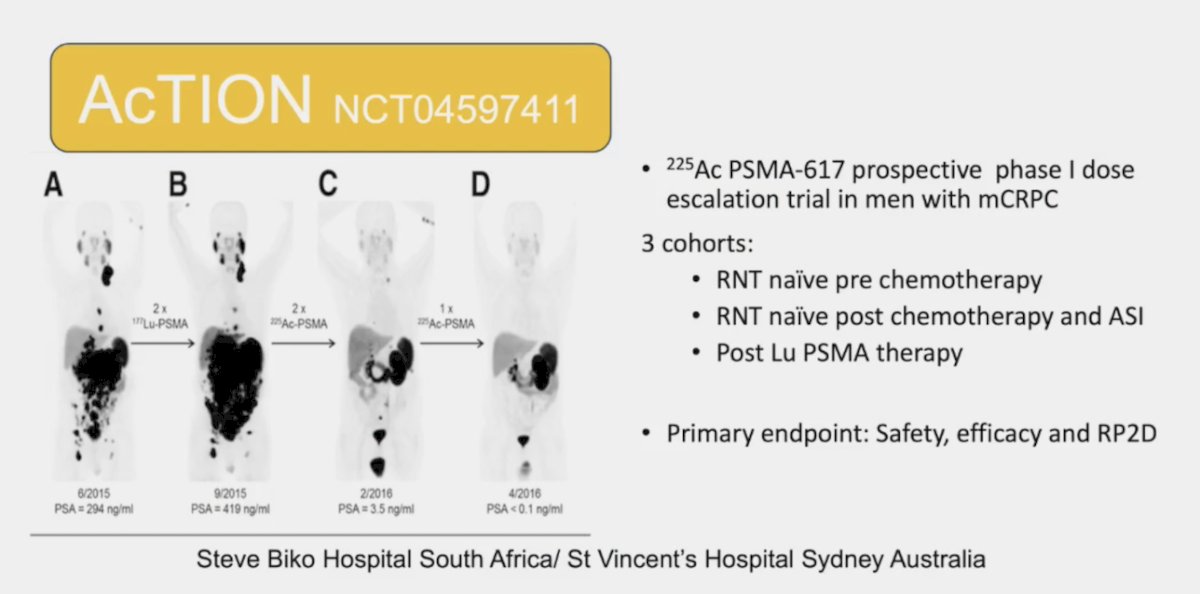
Additionally, PSMAcTION is a phase III trial of 225Ac PSMA-617 versus standard of care after 177Lu-PSMA-617.
Dr. Emmett concluded her presentation discussing what to do in non-responding PSMA radioligand patients with the following take-home points:
- Screening biomarkers and nomograms identify patients likely to have exceptional response to treatment, but are less effective at identifying those who will not respond
- Dose intensification, addition of androgen receptor pathway inhibitors, and/or alpha therapy are all potential options for improving treatment response and limiting non-responders
- Response to the first dose using SPECT and/or PSA and/or ctDNA can help identify radiation resistant disease
- Personalized intensification options based on biomarker patterns of progression may improve individual outcomes in non-responders
Presented by: Louise Emmett, MD, MBChB, FRACP, FAANMS, Department of Theranostics and Nuclear Medicine, St. Vincent’s Hospital, Sydney, New South Wales, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Buteau JP, Martin AJ, Emmett L, et al. PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): A biomarker analysis from a randomized, open-label, phase 2 trial. Lancet Oncol. 2022 Nov;23(11):1389-1397.
- Emmett L, Subramaniam S, Crumbaker M, et a. [177Lu]Lu-PSMA-617 plus enzalutamide in patients with metastatic castration-resistant prostate cancer (ENZA-p): An open-label, multicentre, randomized, phase 2 trial. Lancet Oncol. 2024 May;25(5):563-571.
- Emmett L, Subramaniam S, Crumbaker M, et al. Overall survival and quality of life with [177Lu]Lu-PSMA-617 plus enzalutamide versus enzalutamide alone in metastatic castration-resistant prostate cancer (ENZA-p): Secondary outcomes from a multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2025 Feb 12 [online ahead of print].
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- John N, Pathmanandavel S, Crumbaker M, et al. 177Lu-PSMA SPECT quantification at 6 weeks (dose 2) predicts short progression-free survival for patients undergoing 177Lu-PSMA-I&T therapy. J Nucl Med. 2023 Mar;64(3):410-415.
- Demirci RA, Gulati R, Hawley JE, et al. SPECT/CT in early response assessment of patients with metastatic castration-resistant prostate cancer receiving 177Lu-PSMA-617. J Nucl Med. 2024 Dec 3;65(12):1945-1951.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.