(UroToday.com) The 2025 APCCC Diagnostics annual meeting featured a session on how to monitor metastatic prostate cancer and a presentation by Dr. Andrei Iagaru discussing monitoring of patients on PSMA-radioligand therapy. Dr. Iagaru started his presentation stating that the balance in imaging should not be that all possible imaging is performed, and should not mean that no imaging is performed, but rather the goal is to find the appropriate imaging for monitoring patients on radioligand therapy.
The following arguments could be made for no PSMA imaging being needed:
- In VISION,1 85.1% of participants had a 68Ga-PSMA-11 PET/CT scan meeting the study eligibility definition
- Complexity
- Cost
- It may limit access to care even more than it already does
- Unproven as to whether there are better outcomes
Conversely, the following arguments could be made for PSMA imaging being needed:
- One of the undisputed principles of treatment among patients with cancer is knowing the extent of disease to the best of one’s ability
- By excluding patients unlikely to response, PSMA PET will save health-care costs in the long run
- The additional resources and cost to obtain the useful information from PSMA PET are a small fraction of what a prostate cancer patient and the health care system will spend.
Dr. Iagaru provided the following cost analysis, emphasizing that FDG PET/CT costs $2,545, PSMA PET/CT costs $6,445, and six cycles of 177Lu-PSMA-617 costs $300,000:
The International Atomic Energy Agency can record the number of PET scanners and SPECT scanners (per 1 million), highlighting the geographical variation across the globe: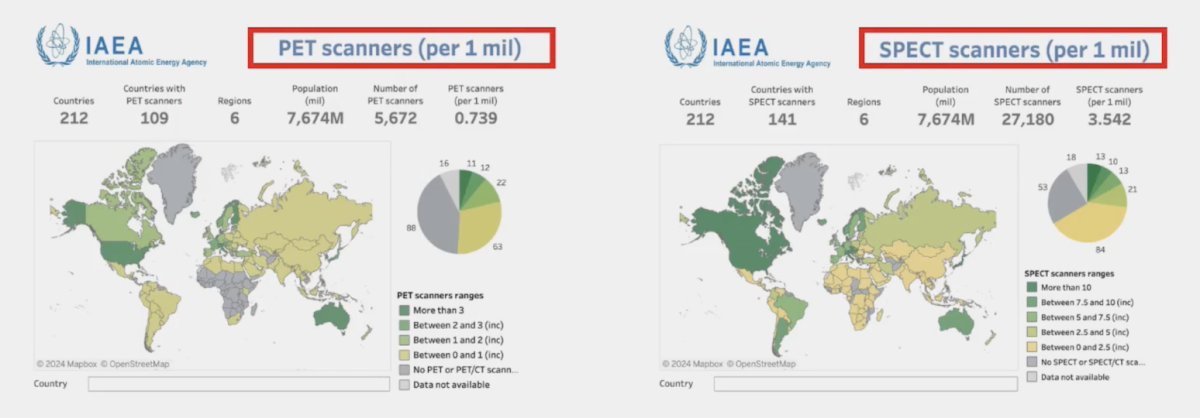
To try and improve speed and accessibility for monitoring therapy, Dr. Iagaru’s team evaluated the feasibility of using the StarGuide, a new generation multi-detector cadmium-zinc-telluride (CZT)-based SPECT/CT, for whole-body imaging in the setting of post-therapy imaging of 177Lu-labeled radiopharmaceuticals.2 Among 31 patients, the StarGuide system acquired vertex to mid-thighs post-therapy SPECT/CT scans with 4 bed positions, 3 min/bed and a total scan time of 12 min. In comparison, the standard GE Discovery 670 Pro SPECT/CT system typically acquires images in 2 bed positions covering the chest, abdomen, and pelvis with a total scan time of 32 min. The post-therapy scans acquired with faster scanning time using StarGuide system had comparable detection/targeting rate compared to the Discovery 670 Pro SPECT/CT system, in addition to detecting larger lesions defined by RECIST criteria on the pre-therapy PET scans:
In an effort to assess response rates and adjust treatment appropriately John et al.3 sought to evaluate change in 177Lu-PSMA SPECT quantitative parameters to monitor treatment response. Among 127 men with progressive mCRPC, at baseline and week 6, 76% had analyzable serial 177Lu-PSMA SPECT/CT imaging. SPECT total tumor volume was reduced between baseline and week 6 in 74% of patients. Any increase in SPECT total tumor volume between baseline and week 6 was associated with significantly shorter PSA progression free survival (HR 2.5, 95% CI, 1.5-4.2) but not overall survival. Thus, increasing PSMA SPECT total tumor volume on quantitative 177Lu-PSMA SPECT/CT predicted short progression-free survival and may play a future role as an imaging response biomarker, identifying when to cease or intensify 177Lu-PSMA therapy. Dr. Iagaru provided the following workflow for incorporating SPECT/CT and allowing switching to other therapies among those patients not responding to 177Lu-PSMA therapy:2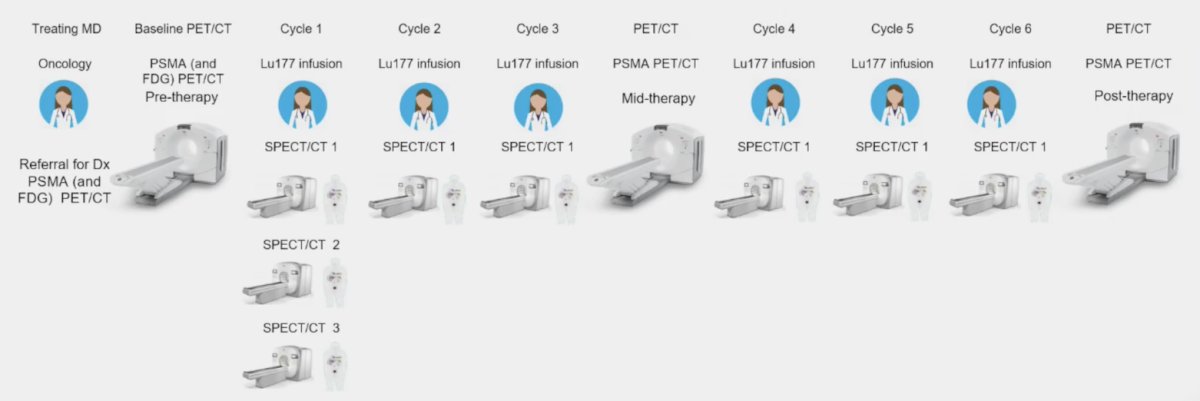
In 2024, Dr. Iagaru’s group published results of their utilization of the StarGuide CZT SPECT/CT system in same-day post-infusion assessment and early treatment response to 177Lu-PSMA-617.4 Among 56 patients who underwent at least 2 post-therapy SPECT/CTs, the whole-body SPECT/CT scans (~ 12 min per scan) were well tolerated, with 221 same-day scans performed (89%). Quantitative analysis of SPECT/CT images showed that 37 patients (66%) had > 30% reduction in Lutetium-total tumor volume, associated with significantly improved overall survival (median not reached versus 6 months, p = 0.008) and PSA progression free survival (median 6 months versus 1 months, p < 0.001).
When and why should we stop 177Lu-PSMA-617 radioligand therapy? Dr. Iagaru notes that this should include when there is FDG positive/PSMA negative disease progression or when there is complete response to treatment: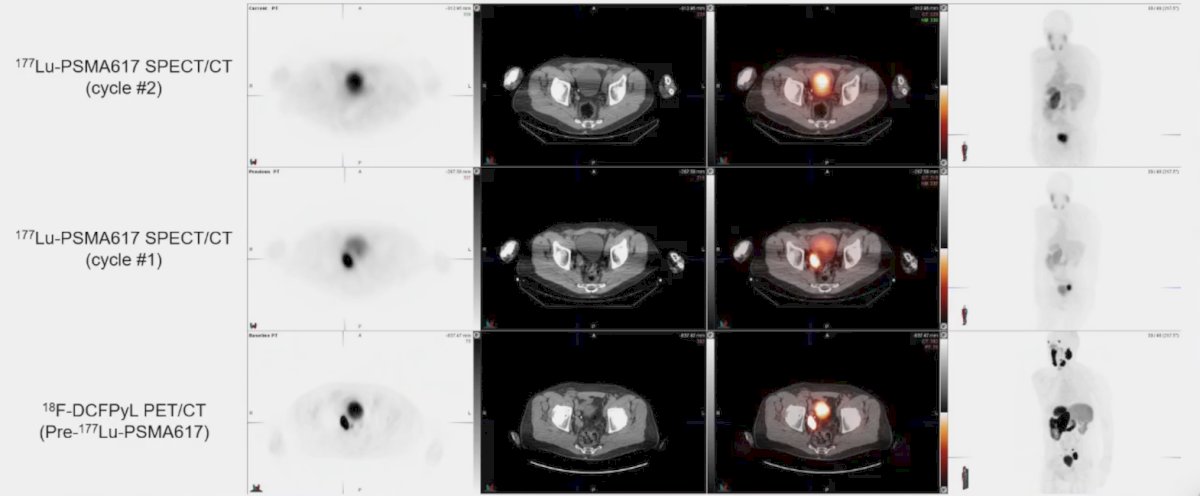
When should we extend 177Lu-PSMA-617 radioligand therapy. Dr. Iagaru notes that this approach has been evaluated in a German multicenter study of 111 patients,5 either as a continuous treatment (38.7%) or as a rechallenge (61.3%) treatment. Overall survival in the continuous group was 23.2 months (95% CI 20.4 – 25.9) versus 40.2 months (95% CI 31.8 – 48.7) in the rechallenge group:![When should we extend 177Lu-PSMA-617 radioligand therapy. Dr. Iagaru notes that this approach has been evaluated in a German multicenter study of 111 patients [5], either as a continuous treatment (38.7%) or as a rechallenge (61.3%) treatment. Overall survival in the continuous group was 23.2 months (95% CI 20.4 – 25.9) versus 40.2 months (95% CI 31.8 – 48.7) in the rechallenge group](/images/com-doc-importer/194-apccc-diagnostics-2025/apccc-diagnostics-2025-monitoring-of-patients-on-psma-radioligand-therapy/image-5.jpg)
Extended therapy with 177Lu-PSMA-617 was safe and was not associated with increased grades 3-4 toxicity.
Dr. Iagaru concluded his presentation discussing monitoring of patients on PSMA-radioligand therapy with the following take-home points:
- Both FDG and PSMA PET provide useful information
- PSMA SPECT is very valuable and can be done very fast with modern scanners
- Multiple biological targets may lead to improved outcomes secondary to better selection
- Require upfront cost but much less than the cost of treatment and toxicities
- The appropriate sequence of imaging is not fully understood or accepted
Presented by: Andrei Iagaru, MD, Division of Nuclear Medicine and Molecular Imaging, Department of Radiology, Stanford University, Stanford, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Song H, Ferri V, Duan H, et al. SPECT at the speed of PET: A feasibility study of CZT-based whole-body SPECT/CT in the post 177Lu-DOTATE and 177Lu-PSMA-617 setting. Eur J Nucl Med Mol Imaging. 2023 Jul;50(8):2250-2257.
- John N, Pathmanandavel S, Crumbaker M, et al. 177Lu-PSMA SPECT quantification at 6 weeks (dose 2) predicts short progression-free survival for patients undergoing 177Lu-PSMA-I&T therapy. J Nucl Med. 2023 Mar;64(3):410-415.
- Song H, Leonio MI, Ferri V, et al. Same-day post-therapy imaging with a new generation whole-body digital SPECT/CT in assessing treatment response to 177Lu-PSMA-617 in metastatic castration-resistant prostate cancer. Eur J Nucl Med Mol Imaging. 2024 Jul;51(9):2784-2793.
- Seifert R, Telli T, Lapa C, et al. Safety and efficacy of extended therapy with [177Lu]Lu-PSMA: A German multicenter study.