(UroToday.com) The 2025 APCCC Diagnostics annual meeting featured a session on how to monitor metastatic prostate cancer and a presentation by Dr. Himisha Beltran discussing when we should assess biology with a re-biopsy.
Castration resistant prostate cancer (CRPC) is a heterogeneous disease with different genomic subtypes (BRCA2, MSI-high, SPOPmut, PTEN loss, TP53, RB1, etc), different phenotypic variants (histologic – small cell carcinoma; gene expression, PSMA-negative/FDG avid), and different resistance mechanisms (most are androgen receptor driven; non-androgen receptor driven tumors include loss of androgen receptor expression/signaling). Androgen receptor (and PSMA) expression can be lost in late-stage disease, which has implications for androgen receptor and PSMA therapy: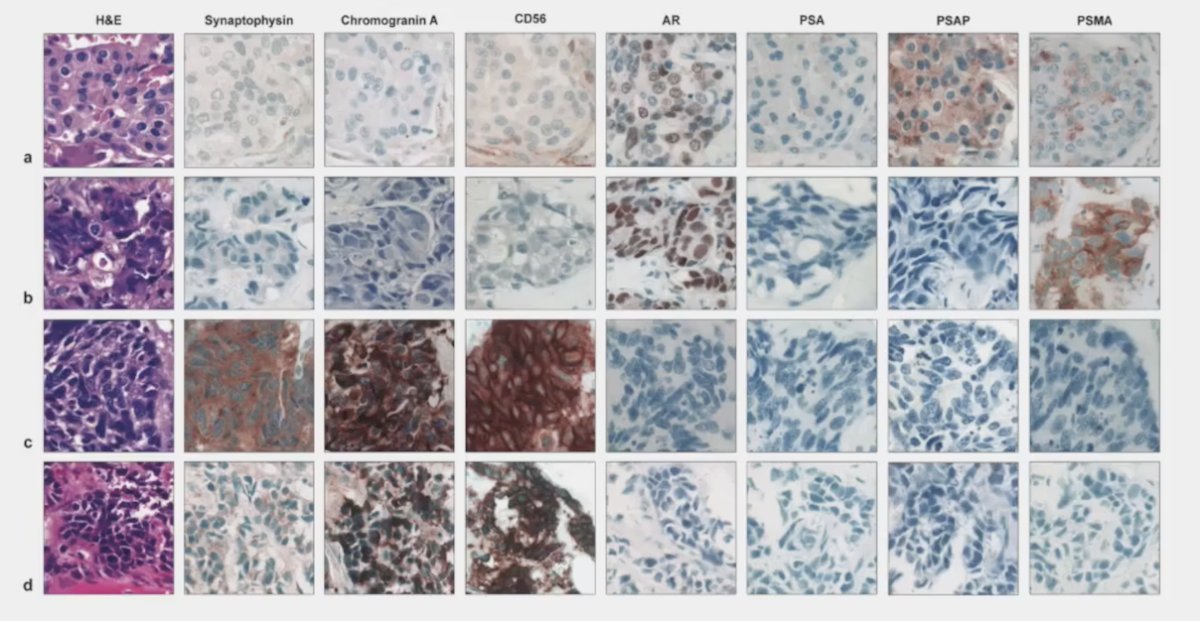
The reason it important to know about phenotype is that it (i) can impact expression of surface targets (PSMA, STEAP1, B7H3, DLL3, etc), (ii) is important for disease monitoring (PSA, PSMA, ctDNA), and (iii) is important for selection of lineage-directed therapy (ie. neuroendocrine prostate cancer directed therapies, such as the DLL3 T-cell engager tarlatamab).
Dr. Beltran then discussed when we should consider a new biopsy, with the following reasons:
- Ruling out other cancers, especially in the setting of low PSA/PSMA and atypical progression
- Consideration of small cell carcinoma/neuroendocrine prostate cancer therapies
- Enrollment in clinical trials using cell surface therapies (ie. B7H3 expression)
- Repeat genomic analysis
Reasons why we should not do a re-biopsy include the fact that (i) re-biopsying everyone is likely to have low yield, (ii) a re-biopsy is invasive, and (iii) we can consider platinum chemotherapy even in the absence of neuroendocrine histology, especially if there are AVPC clinical features or combined tumor suppressor loss (ie. PTEN, RB1, TP53).
In prostate cancer, therapeutic pressure may lead to small cell/neuroendocrine prostate cancer transformation, and although rare, it is important to recognize. The following patient developed new liver and lung metastases while on abiraterone in the absence of significant PSA progression (PSA 29 ng/mL):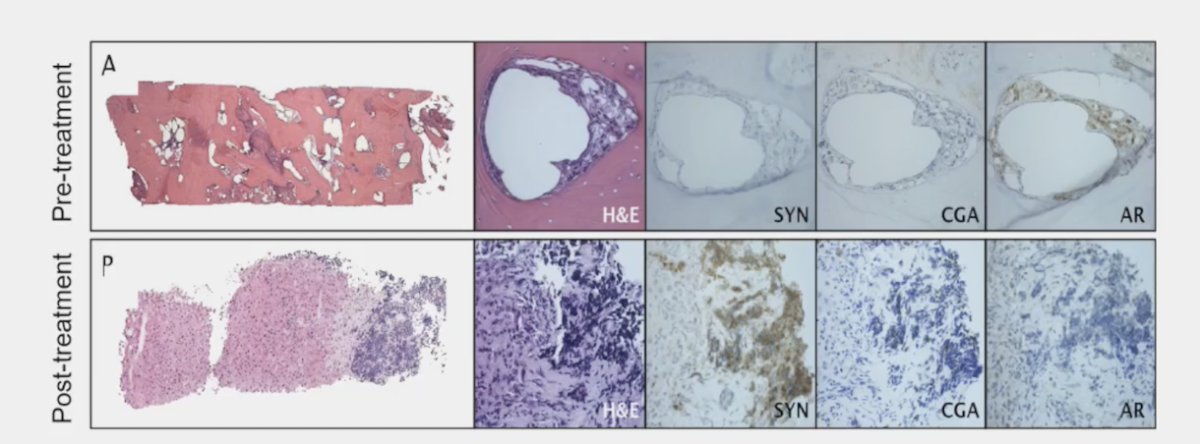
The reason neuroendocrine prostate cancer is so controversial is because some people never or rarely see a case of neuroendocrine prostate cancer, and others report up to 15-20% of CRPC tumors are neuroendocrine prostate cancer. Possible explanations for this discrepancy include (i) repeat biopsies are not standardly done in mCRPC, (ii) there is variability amongst pathologists and the evaluation and nomenclature are not standardized, and (iii) intra-patient heterogeneity exists. In 2024, Dr. Beltran notes that they gathered a group of pathologists and clinical experts to develop a framework for the pathology workup of mCRPC biopsies,1 with the goal of putting together a simple, standardized diagnostic framework: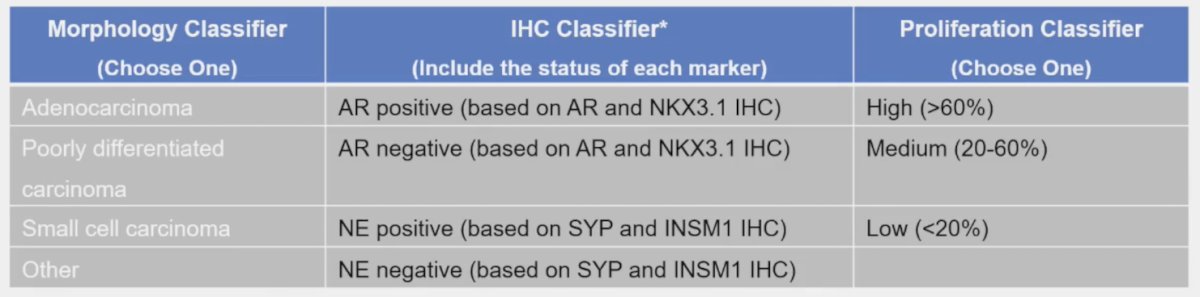
DLL3 is also important and has expression in many neuroendocrine carcinomas; however is not expressed in prostate adenocarcinoma:
Dr. Beltran noted that the DLL3 T-cell engager tarlatamab was FDA approved in May 2024 for the treatment of previously treated small cell lung cancer patients.
There are several limitations of tumor biopsies, including:
- Single site biopsy does not capture intra-patient heterogeneity, and variations can be seen across metastatic sites
- Liquid biopsies and molecular imaging may complement or potentially replace metastatic biopsies in the future, which may include:
- Cell free DNA (ctDNA tumor fraction, especially when PSA is not reliable)
- Circulating tumor cell expression of lineage markers, targets, and other gene programs
- PSMA PET imaging
- Other PET tracers (ie. FDG, fluciclovine, FAPI, DOTATATE, DLL3, etc)
In 2024, Franceschini et al.2 reported results of their targeted DNA methylation assay to detect castration-resistant neuroendocrine prostate cancer using plasma cell free DNA: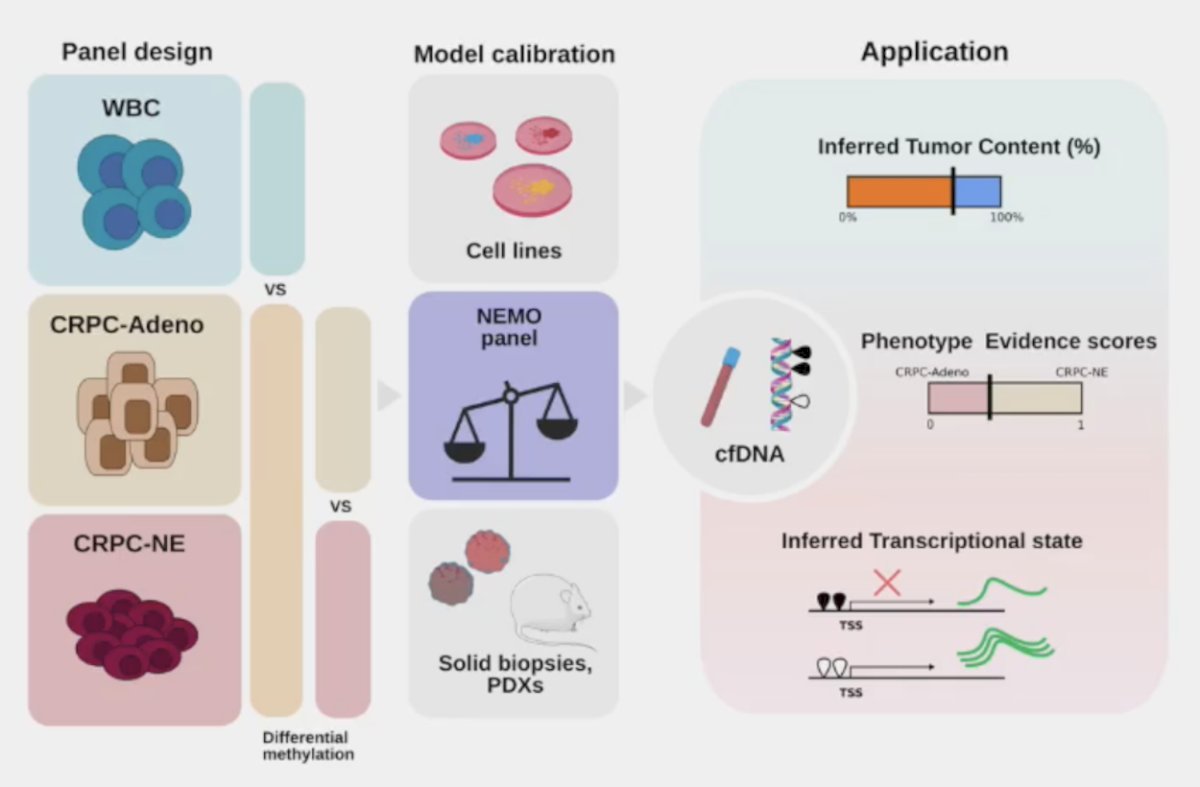
They found that in independent clinical cohorts (n = 222 plasma samples), the assay achieved an AUC > 0.93 for detecting pathology-confirmed castration-resistant neuroendocrine prostate cancer (n = 136):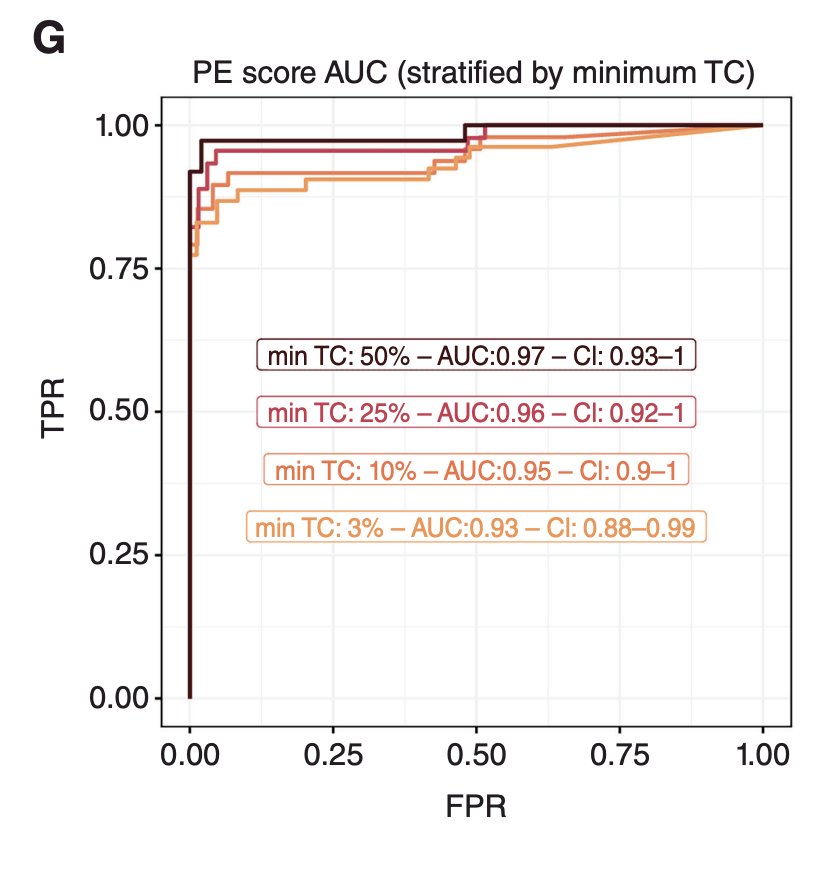
PSMA is “lost” in androgen receptor negative and neuroendocrine prostate cancer, marking a unique subset of CRPC. In fact, 12.6% of patients in VISION3 and 28% of patients in TheraP4 were not eligible for 177Lu-PSMA-617 secondary to PSMA negative disease:![PSMA is “lost” in androgen receptor negative and neuroendocrine prostate cancer, marking a unique subset of CRPC. In fact, 12.6% of patients in VISION [3] and 28% of patients in TheraP4 were not eligible for 177Lu-PSMA-617 secondary to PSMA negative disease](/images/com-doc-importer/194-apccc-diagnostics-2025/apccc-diagnostics-2025-when-to-assess-biology-with-a-re-biopsy/image-6.jpg)
Ultimately, it is important to refine PSMA as a biomarker in mCRPC, given the inter-patient, intra-patient, and temporal PSMA heterogeneity in patients recruited for PSMA radioligand therapy.
Can we use DLL3 imaging to diagnose neuroendocrine prostate cancer? 89Zr-Sc16 is the first PET scan tracer for detecting and quantifying in vivo tumor DLL3 expression:
However, there are still several questions surrounding DLL3 imaging:
- Does it complement PSMA PET and FDG?
- What is the patient selection criteria for DLL3-targeted treatment?
- What are the resistance patterns?
Finally, Dr. Beltran highlighted a pilot study for detection of PSMA-low castration resistant and neuroendocrine prostate cancer with 18F-fluciclovine PET/CT imaging that is being done at her institution, the Dana-Farber Cancer Institute: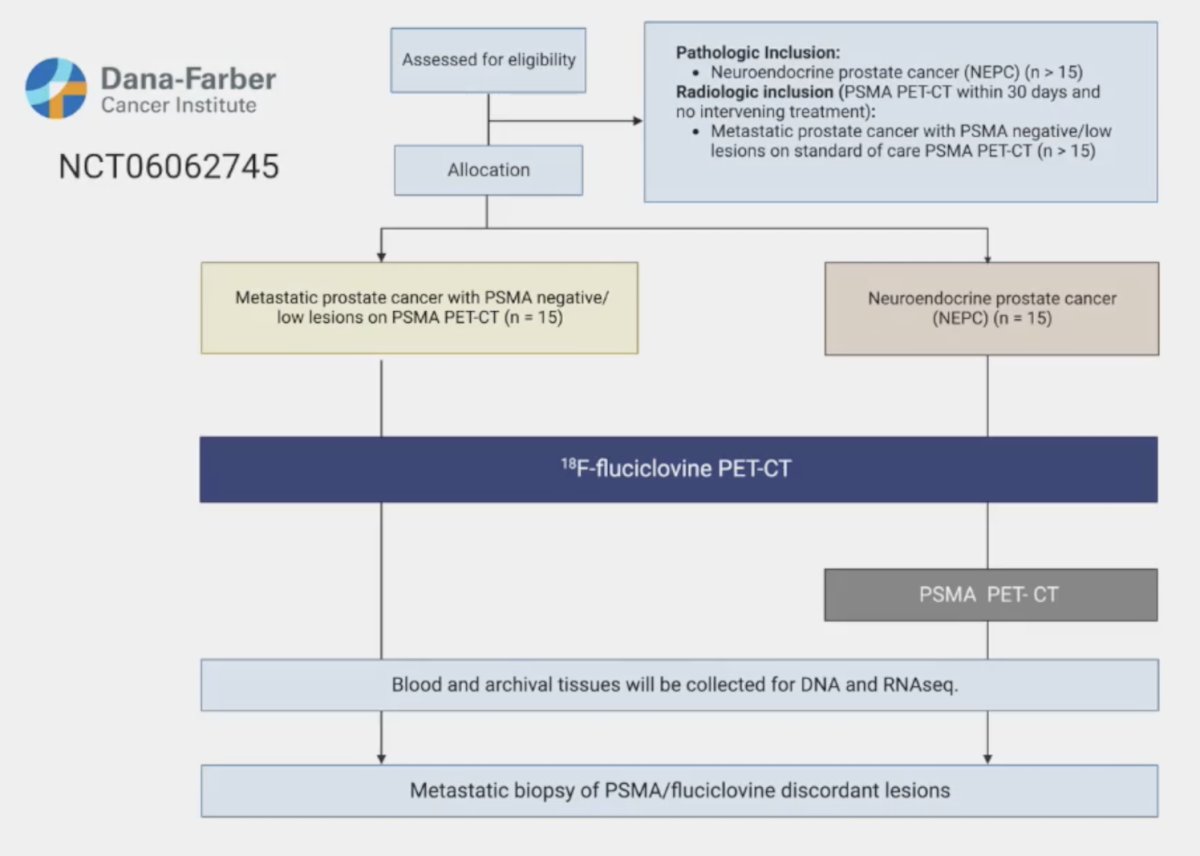
Dr. Beltran concluded her presentation discussing when we should assess biology with a re-biopsy with the following take-home points:
- mCRPC evolves during disease progression and can acquire phenotypic changes that impact response to therapy and outcomes
- Repeat biopsy could be considered for patients with atypical progression, low PSA, low PSMA, high FDG, or aggressive disease to evaluate for histologic changes (ie. neuroendocrine prostate cancer)
- Cell surface target expression can by dynamic (PSMA, DLL3, B7H3, STEAP1, etc), and understanding the biology of target dynamics could optimize patient selection and inform biomarkers and combinations
- Combined imaging + liquid biomarkers might complement or replace the need for repeat metastatic biopsies in the future to identify specific CRPC phenotypic subtypes for more precise therapy
Presented by: Himisha Beltran, MD, Department of Medical Oncology, Dana Farber Cancer Institute and Harvard Medical School, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Haffner MC, Morris MJ, Ding CKC, et al. Framework for the Pathology Workup of Metastatic Castration-Resistant Prostate Cancer Biopsies. Clin Cancer Res. 2025 Feb 3;31(3):466-78.
- Franceschini GM, Quaini O, Mizuno K, et al. Noninvasive detection of neuroendocrine prostate cancer through targeted cell-free DNA methylation. Cancer Discov. 2024 Mar 1;14(3):424-445.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.