(UroToday.com) The 2025 APCCC Diagnostics annual meeting featured a session on how to monitor metastatic prostate cancer and a presentation by Dr. Bertrand Tombal discussing what we can expect from monitoring metastatic disease. Dr. Tombal started with a case presentation of a 68 year old with urinary symptoms (IPSS 15) and screening PSA of 245 ng/mL. A biopsy showed extensive Gleason 8 prostate cancer, staging CT scan was normal, and a bone scan showed multifocal bone metastases with mild to moderate hyper fixation. He was started on degarelix + enzalutamide, with moderate side effects (grade 2 fatigue, sexual dysfunction, and difficulty concentrating on daily activities). His PSA subsequently decreased to 0.2 ng/mL on treatment, however, his bone scan showed no change in expression. Does this indicate response to treatment?
Dr. Tombal notes that from the ENZAMET trial,1 we have made significant progress in survival among men with newly diagnosed mHSPC, but there are still 30-40% of men that die at 5 years, and many will be exposed to a very long duration of treatment:

Thus, the crux of the matter is whether we should do more (escalation) or do less (de-escalation) therapy. Looking back at the SWOG 9346 trial,2 absolute PSA value after ADT is in itself a strong independent predictive of survival in newly diagnosed metastatic prostate cancer:

Moreover, deep and durable PSA response to darolutamide + ADT + docetaxel is also associated with improved overall survival in the phase 3 ARASENS trial:3

The importance of deep, rapid, and durable PSA response has also been corroborated in the TITAN phase 3 study of ADT + apalutamide in mHSPC patients.4 However, 20% of men still die at 3 years:

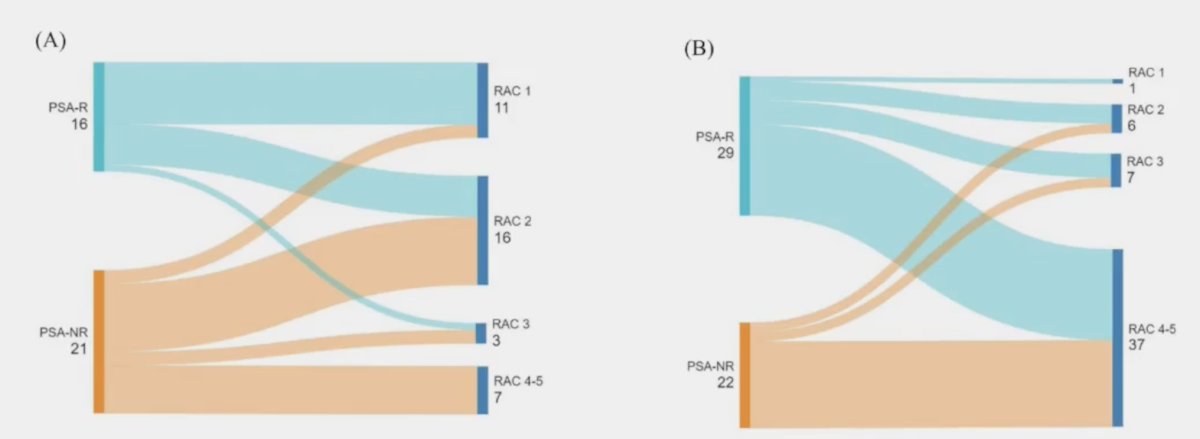
What is the role of whole body MRI? In 2024, Van Damme et al.5 sought to explore the potential prognostic value of PSA and whole body MRI responses in 37 mHSPC and 51 mCRPC patients before and after 6-12 months of ADT and an androgen receptor pathway inhibitor therapy. They found that agreement between PSA and whole body MRI responses was fair in mHSPC (κ = 0.30) but quite poor in mCRPC (κ = 0.15). However, whole body MRI progression in mHSPC patients was associated with a significantly higher risk of death (HR 8.59; p = 0.002). The following figure highlights the concordance and discordance between response assessment via PSA and via whole body MRI use MET-RADS-P response assessment categories:
Dr. Tombal then highlighted two questions from the APCCC Diagnostic 2025 consensus panel:
Q: What are your imaging evaluation criteria for defining progression of bone metastases on bone scintigraphy in mHSPC or mCRPC patients on systemic therapy?
- Appearance of a new lesion or increased activity in existing lesions: 17%
- Appearance of at least two lesions (PCWG3): 64%
- Appearance of at least two lesions and repetition of a confirmatory bone scan at 8 weeks: 19%
Q: What is your imaging evaluation to confirm an equivocal progression on a bone scintigraphy?
- Plain X-rays: 0%
- Computed tomography: 18%
- Whole body MRI: 19%
- PSMA PET/CT: 44%
- Wait for the next bone scintigraphy: 19%
Dr. Tombal concluded his presentation by discussing what we can expect from monitoring metastatic prostate cancer with the following take-home points:
- We need to be able to better define minimal residual disease – how much, where, and what phenotype
- We need to be better at identifying progression – when, where, and what phenotype
Presented by: Bertrand F. Tombal, MD, PhD, Institut de Recherche Clinique, Universite Catholique de Louvain, Louvain, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Sweeney CJ, Martin AJ, Stockler MR, et al. Testosterone suppression plus enzalutamide versus testosterone suppression plus standard antiandrogen therapy for metastatic hormone-sensitive prostate cancer (ENZAMET): An international, open-label, randomized, phase 3 trial. Lancet Oncol. 2023 Apr;24(4):323-334.
- Hussain M, Tangen CM, Higano C, et al. Absolute prostate-specific antigen value after androgen deprivation is a strong independent predictor of survival in new metastatic prostate cancer: Data form Southwest Oncology Group Trial 9346 (INT-0162). J Clin Oncol. 2006 Aug 20;24(24):3984-3990.
- Saad F, Hussain MHA, Tombal B, et al. Deep and Durable Prostate-specific Antigen Response to Darolutamide with Androgen Deprivation Therapy and Docetaxel, and Association with Clinical Outcomes for Patients with High- or Low-volume Metastatic Hormone-sensitive Prostate Cancer: Analyses of the Randomized Phase 3 ARASENS study. Eur Urol. 2024 Oct;86(4):329-339.
- Chowdhury S, Bjartell A, Agarwal N, et al. Deep, rapid, and durable prostate-specific antigen decline with apalutamide plus androgen deprivation therapy is associated with longer survival and improved clinical outcomes in TITAN patients with metastatic castration-sensitive prostate cancer. Ann Oncol. 2023 May;34(5):477-485.
- Van Damme J, Tombal B, Michoux N, et al. Value of whole-body magnetic resonance imaging using the MET-RADS-P criteria for assessing the response to intensified androgen deprivation therapy in metastatic hormone-naïve and castration-resistant prostate cancer. Eur Urol Oncol. 2024 Nov 5:S2588-9311(24)00238-4.