(UroToday.com) The Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025, held in Lugano, Switzerland, on February 27th and 28th, was host to a session addressing the contemporary management of biochemically recurrent prostate cancer patients. Dr. Jochen Walz discussed ‘when to act’ for a PSA relapse.
What are the definitions of biochemical recurrence?
- Following a radical prostatectomy: Rising PSA level to ≥0.2 ng/ml, with a subsequent confirmatory reading of >0.2 ng/ml
- Following radiotherapy (external beam or brachytherapy): PSA nadir + 2 ng/ml
Dr. Walz emphasized that biochemical failure is not a justification per se to initiate additional treatment. It, in itself, is not equivalent to clinical failure, and thus, do we need to treat all patients with biochemical failure? Historical data from the Johns Hopkins series provides important information regarding the natural history of biochemically recurrent prostate cancer patients. The median time from biochemical recurrence to the development of metastases in untreated patients is ~8 years, and then from metastases to death is ~5 years.1,2 As such, there is a median interval of ~13 years from biochemical recurrence to death. This highlights the fact that many such patients have a prolonged disease course, not requiring aggressive adjuvant/salvage therapy, and the importance of considering patients’ life expectancies when weighing treatment options.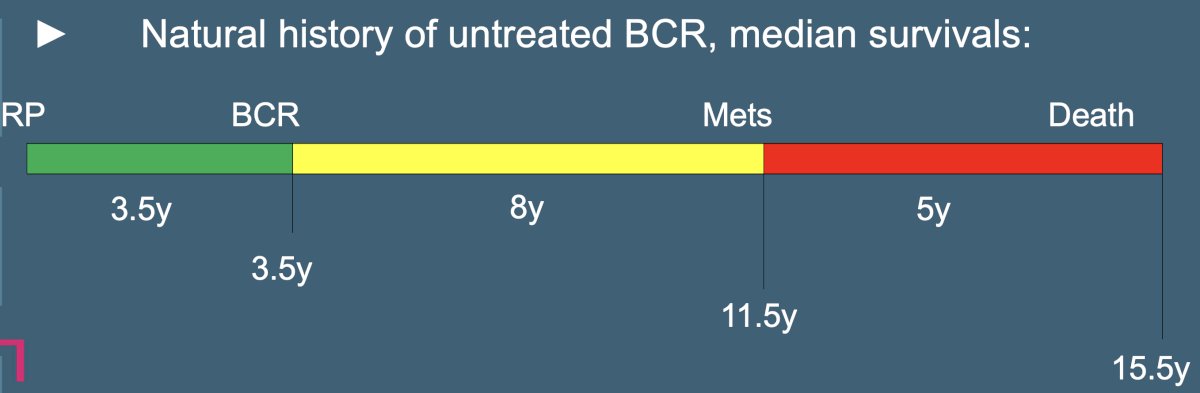
Classically, a serum PSA level of ≥0.2 ng/ml has been used to define biochemical recurrence following a radical prostatectomy. Given that many such patients have an indolent or prolonged disease course, can an alternate (i.e., higher) PSA cutoff with an improved prognostic utility be employed in this setting? Numerous studies have demonstrated that a PSA cutoff >0.4 ng/ml has a superior ability to predict subsequent disease progression in biochemically recurrent patients.
What about PSA cut-offs in the post-radiotherapy setting? Should a cut-off of nadir + 2 ng/ml be used, or should an alternate cut-off be employed in this setting? Seminal work by Roach et al. demonstrated that a cut-off of nadir +2 is associated with a sensitivity of 64% and specificity of 78% for detecting subsequent disease progression. A higher cut-off of nadir + 3 ng/ml is associated with superior specificity (82% versus 78%) but at the cost of a significantly lower sensitivity for subsequent disease progression (56% versus 64%). Conversely, a cut-off of nadir +1 has superior sensitivity (68%) but lower specificity (66%).6 Overall, the consensus is that a cut-off of nadir + 2 ng/ml offers the best ‘compromise’ in this setting.
Important factors to consider when contemplating the timing of imaging and subsequent treatment of biochemically recurrent patients include:
- Radical prostatectomy, presence/absence of:
- pT3 disease
- pN+ disease
- Pathologic Grade Group ≥4
- Radiotherapy patients
- Clinical stage
- Biopsy Grade Group
Another important predictor of the subsequent risk of progression is the time to PSA recurrence, with ‘high risk’ intervals defined as <2 years in post-radical prostatectomy patients and <1.5 to 2.5 years in radiotherapy-treated patients.
PSA velocity is another important consideration, with a PSA velocity at relapse of >0.75 ng/ml/year shown to be strongly correlated with the risk of subsequent disease progression.7 Additionally, various PSA doubling time cut-offs for predicting the subsequent risk of disease progression have been proposed:
It is clear, however, from the work published by Freedland et al. in JAMA in 2005, that the risk of subsequent disease progression is highest for patients with a PSA doubling time of <9 months, particularly those with a doubling time <3 Month (HRs: 8.8 – 27.5, p<0.001). These important findings have served as the foundation for subsequent studies, notably the EMBARK trial, which demonstrated important survival benefits for the addition of enzalutamide to leuprolide for high-risk biochemically recurrent patients with a PSA doubling time ≤9 months (5-year metastasis-free survival: 87% versus 71% for leuprolide alone; HR: 0.42, p<0.001).7
While patients with a PSA doubling time of <9 months have been clearly identified as being at high risk for the subsequent development of metastases, with the risk highest in those with a doubling time <3 Months; this represents a broad range of PSA doubling times. Can we further define a more specific PSA doubling time cutoff? In 2019, Markowski et al. demonstrated that the risk of subsequent progression to distant metastases sharply increases when the PSA doubling time decreases to ≤5 months.8
Another important factor to consider in the biochemically recurrent setting is the competing risk of death from other causes. For patients with a PSA doubling time ≤15 months, it appears that the risk of prostate cancer-specific mortality mirrors that of all-cause mortality (i.e., similar likelihood of dying from prostate cancer versus any other cause). Conversely, for patients with a PSA doubling time >15 months, patients are significantly more likely to die of other causes.9
Another obvious tool to incorporate in the risk stratification of biochemically recurrent patients is PSMA PET, with pelvic nodal PET-positive patients having worse failure-free survival outcomes, compared to both prostate bed-positive and PSMA PET-negative patients.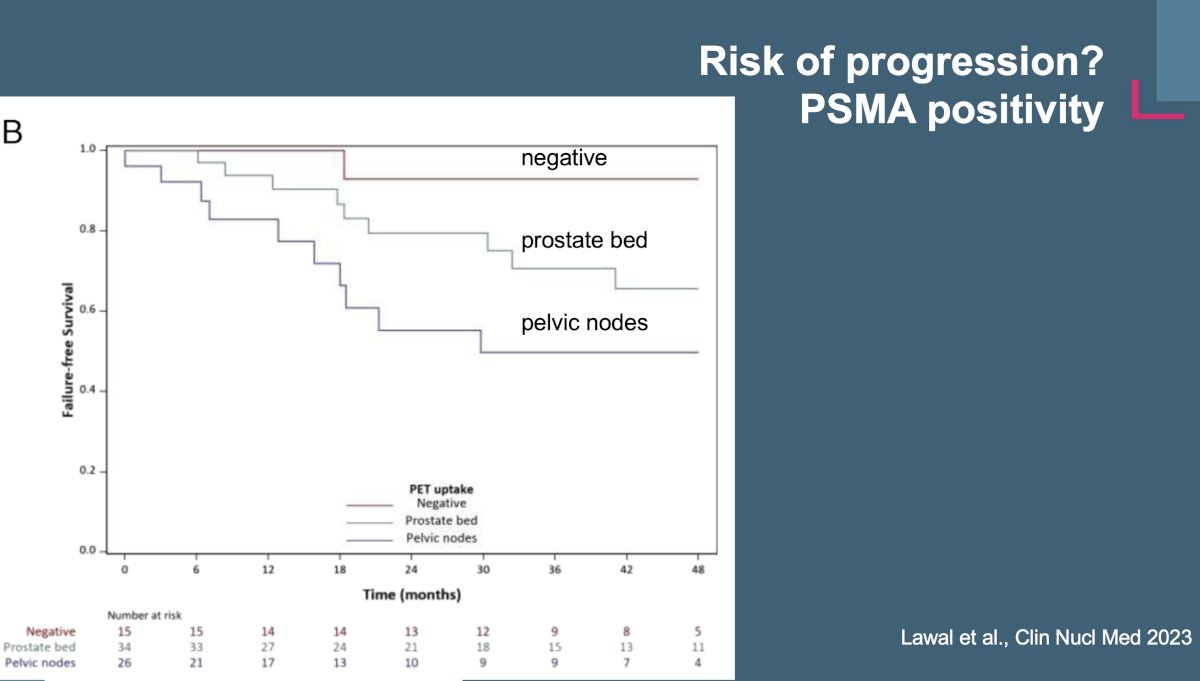
The EAU currently uses the following system to risk stratify patients into low- and high-risk groups for subsequent disease progression:
Following a radical prostatectomy, ‘high risk’ biochemically recurrent patients are those with a PSA doubling time ≤1 year and/or pathologic Grade Group 4–5 disease. Following radiotherapy, high-risk patients are those with a time to biochemical failure of ≤18 months and/or biopsy Grade Group 4–5 disease.
This risk stratification system helps guide the timing of imaging and subsequent treatment decision making. Currently, the EAU recommends offering monitoring, including interval PSA testing, to patients with EAU low-risk biochemical recurrences following either a radical prostatectomy or radiotherapy (weak recommendations).

When should biochemically recurrent patients in the post-radical prostatectomy setting receive salvage therapy? In 2016, Tendulkar et al. demonstrated that patients who receive salvage radiotherapy at lower PSA levels (i.e., <0.5 ng/ml) have superior freedom from biochemical failure survival outcomes, compared to those who receive salvage radiotherapy at higher PSA levels.10 These results solidified the role of early salvage, as opposed to late salvage, radiotherapy in this setting.

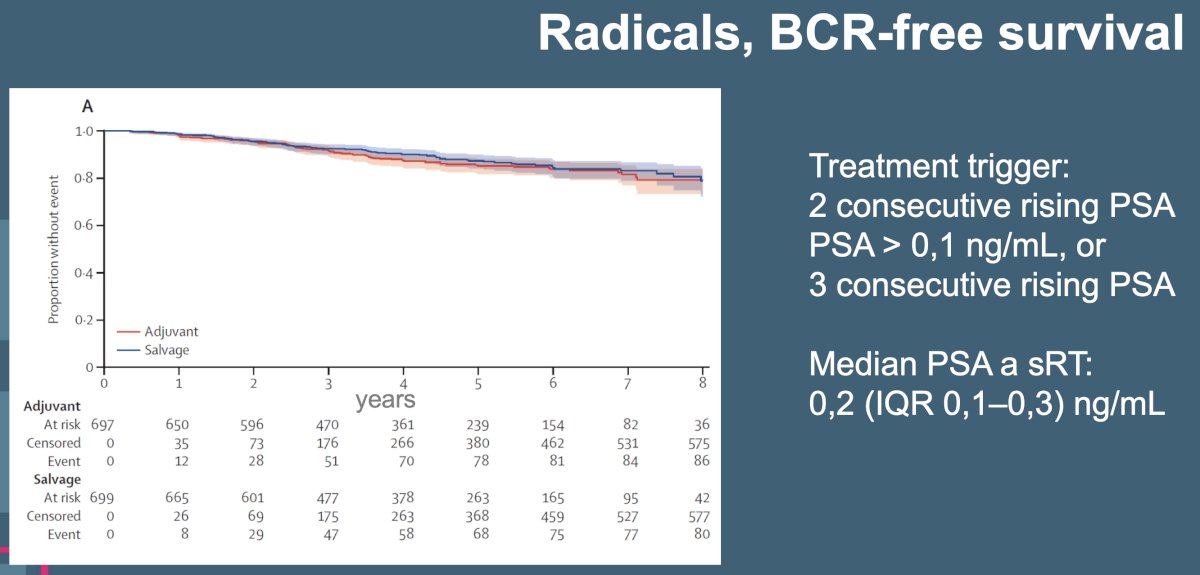
What about adjuvant versus early salvage radiotherapy? To date, three trials in this space have failed to demonstrate a relative survival benefit for adjuvant radiotherapy, compared to early salvage radiotherapy. The RADICALS-RT trial was a phase III trial that randomized 1,396 patients with evidence of biochemical progression following radical prostatectomy and ≥1 risk factor (pathologic T3-4, Gleason Score of 7-10, positive margins, or pre-operative PSA ≥10 ng/mL) 1:1 to either adjuvant radiotherapy or an observation policy with salvage radiotherapy for PSA biochemical progression (PSA ≥0.1 ng/mL or 3 consecutive rises). Notably, 24% of patients received concurrent androgen suppression. At a median follow-up of 4.9 years, no differences were seen in the 5-year biochemical progression-free survival rates: 85% for adjuvant and 99% for salvage radiotherapy (HR: 0.88, 95% CI: 0.58 – 1.33, p=0.53). Notably, self-reported urinary incontinence was worse at one year for those in the adjuvant radiotherapy group (mean score 4.8 vs 4.0; p=0·0023).11
Published at the same time, RAVES also evaluated the role of adjuvant versus early salvage radiotherapy. This non-inferiority phase III trial randomized 333 patients who had undergone a radical prostatectomy and had high-risk features (positive surgical margin, extraprostatic extension, or seminal vesicle invasion) who developed biochemical recurrence following a post-operative PSA level of 0.1 ng/ml or less. Patients were randomized 1:1 to either adjuvant radiotherapy (64 Gy in 32 fractions) within six months or early salvage radiotherapy for a PSA of 0.20 ng/ml or higher. No concurrent ADT was given. At a median follow-up of 6.1 years, the 5-year freedom from biochemical progression was non-significantly different (adjuvant: 86% versus salvage: 87%; HR: 1.12, 95% CI: 0.65 – 1.90). Only 50% of patients in the salvage arm actually received radiotherapy. The grade 2 or worse genitourinary toxicity rate was lower in the salvage radiotherapy group (54% versus 70%), with no difference in grade 2 or worse gastrointestinal toxicity rates (10% versus 14%).12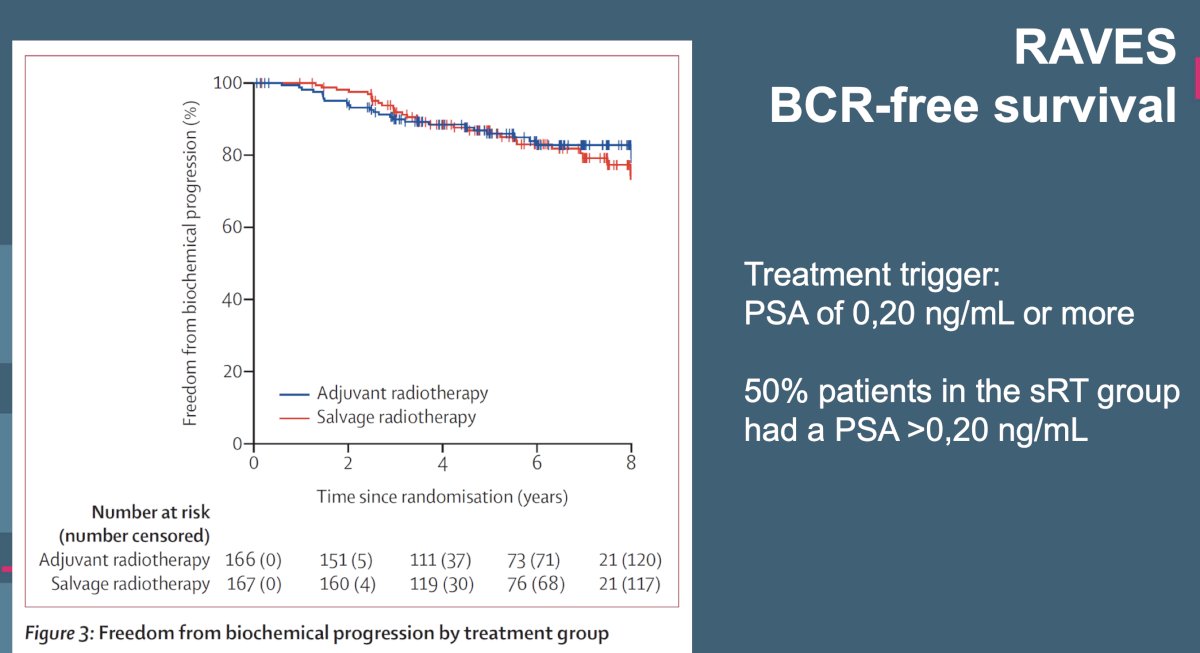
Also published concurrently, the GETUG-17 trial assessed the role of adjuvant versus early salvage radiotherapy in 424 patients within a similar framework to the other trials. Of note, all patients in this trial received androgen suppression for 6 months. Similar to the RAVES trial, the corresponding independent data monitoring committee recommended early termination of enrollment because of unexpectedly low event rates. At a median follow-up of 75 months, 54% of patients in the early salvage arm received radiotherapy. There was no significant difference in the primary study outcome of 5-year event-free survival: 92% (95% CI: 86 – 95) in the adjuvant arm and 90% (95% CI: 85 – 94%) in the early salvage arm (HR: 0.81, 95% CI: 0.48 – 1.36, p=0.42).13 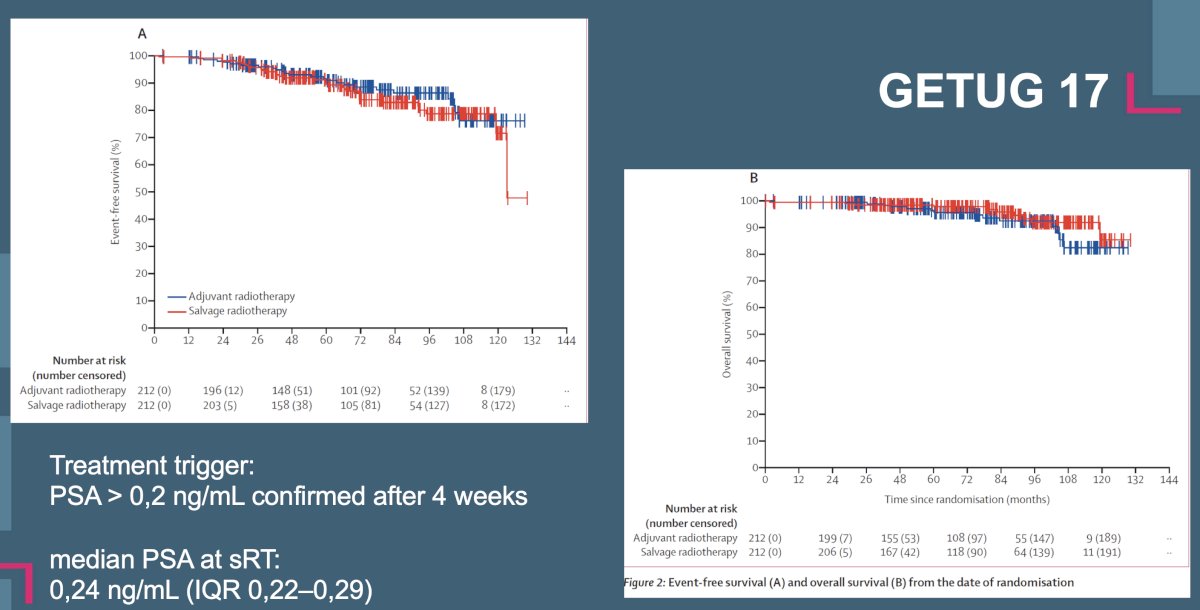
Dr. Walz concluded his presentation with the following take home messages:
- Biochemical recurrence remains a heterogenous clinical scenario
- Prior to treatment, estimate a patient’s life expectancy and consider the cancer’s potential for disease progression
- Offer close monitoring in patients at low risk of progression
- Early salvage treatment is preferred to adjuvant therapy in the majority of biochemically recurrent patients
- Improved treatment selection leads to improved clinical outcomes
Presented by: Jochen Walz, MD, Associate Professor in Urology and Head of the Department of Urology at the Institut Paoli-Calmettes Cancer Centre, Marseille, France
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:- Pound CR, Partin AW, Eisenberger MA, et al. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999; 281(17): 1591-7.
- Freedland SJ, Humphreys EB, Mangold LA, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA. 2005; 294(4): 433-9.
- Cookson MS, Aus G, Burnett AL, et al. Variation in the definition of biochemical recurrence in patients treated for localized prostate cancer: the American Urological Association Prostate Guidelines for Localized Prostate Cancer Update Panel report and recommendations for a standard in the reporting of surgical outcomes. J Urol. 2007; 177(2): 540-5.
- Boccon-Gibod L, Djavan WB, Hammerer P, et al. Management of prostate-specific antigen relapse in prostate cancer: a European Consensus. Int J Clin Pract. 2004; 58(4): 382-90.
- Amling CL, Bergstralh EJ, Blute ML, Slezak JM, Zincke H. Defining prostate specific antigen progression after radical prostatectomy: what is the most appropriate cut point? J Urol. 2001; 165(4): 1146-51.
- Roach M 3rd, Hanks G, Thames Jr H, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. 2006; 65(4): 965-74.
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2023; 389(16): 1453-65.
- Markowski MC, Chen Y, Feng Z, et al. PSA Doubling Time and Absolute PSA Predict Metastasis-free Survival in Men With Biochemically Recurrent Prostate Cancer After Radical Prostatectomy. Clin Genitourin Cancer. 2019; 17(6): 470-475.e1.
- Freedland SJ, Humphreys EB, Mangold LA, et al. Death in patients with recurrent prostate cancer after radical prostatectomy: prostate-specific antigen doubling time subgroups and their associated contributions to all-cause mortality. J Clin Oncol. 2007; 25(13): 1765–71.
- Tendulkar RD, Agarwal S, Gao T, et al. Contemporary Update of a Multi-Institutional Predictive Nomogram for Salvage Radiotherapy After Radical Prostatectomy. J Clin Oncol. 2016; 34(30): 3648-54.
- Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): a randomised, controlled phase 3 trial. Lancet. 2020; 396(10260): 1413-1421.
- Kneebone A, Fraser-Browne C, Duchesne GM, et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): a randomised, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020; 21(10): 1331-1340.
- Sargos P, Chabaud S, Latorzeff I, et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localised prostate cancer after radical prostatectomy (GETUG-AFU 17): a randomised, phase 3 trial. Lancet Oncol. 2020 ;21(10): 1341-1352.