(UroToday.com) The Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 held in Lugano, Switzerland was host to a session addressing the contemporary management of biochemically recurrent prostate cancer patients. Dr. Piet Ost discussed the timing of imaging in the biochemically recurrent setting.
Dr. Ost noted that imaging is a tool we all use, but few people know how to use it and, more importantly, know what to do with the results. Biochemical recurrence following radiotherapy is defined by any PSA increase >2 ng/mL, irrespective of the nadir value (Phoenix criteria).1 Conversely, following a radical prostatectomy, the EAU guidelines define biochemical failure as either:
- Persistent PSA, defined as a detectable post-operative PSA of ≥0.1 ng/ml, within 4 to 8 weeks of surgery
- Two consecutive PSA rises following prior undetectable levels.
- Most salvage radiotherapy trials use readings ≥0.1 ng/ml
In the setting of biochemical recurrence, it is important to ‘risk stratify’ these patients into low- and high-risk groups, as defined by the EAU in the table below.

Following a radical prostatectomy, ‘high risk’ biochemically recurrent patients are those with a PSA doubling time ≤1 year and/or pathologic Grade Group 4–5 disease. Following radiotherapy, high-risk patients are those with a time to biochemical failure of ≤18 months and/or biopsy Grade Group 4–5 disease. This risk stratification system helps guide the timing of imaging and subsequent treatment decision making.

Dr. Ost noted that current imaging tools in our arsenal include:
- Bone scintigraphy
- CT and MRI
- PET scans
This is accompanied by the following treatment tools:
- Systemic therapies
- Combination therapies
- Local therapies

Dr. Ost noted that the key here is to translate the relevant information provided by these imaging tools into meaningful treatment decisions.
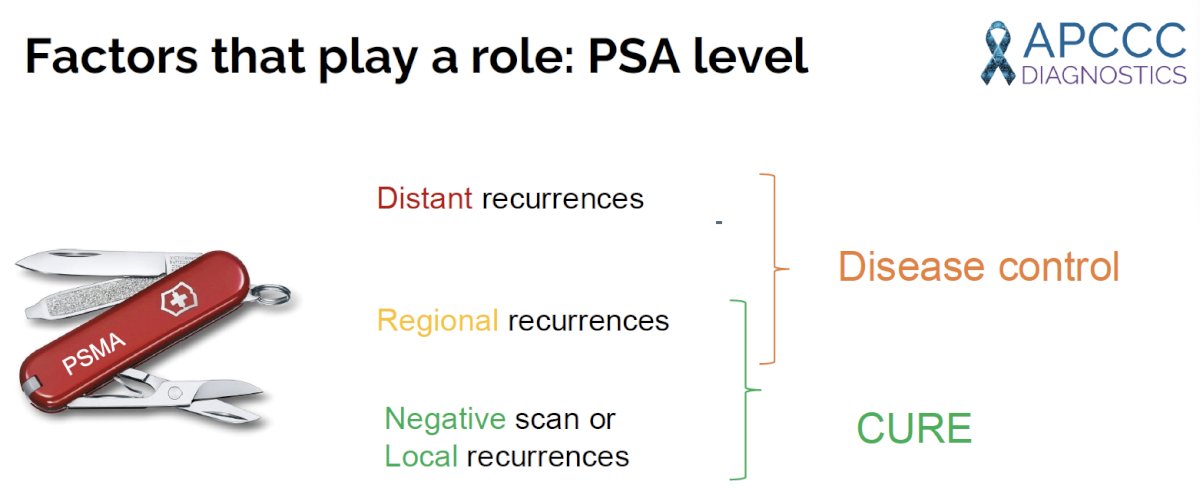
The ideal imaging tool is a versatile, ‘Swiss army knife’-like modality that provides granular, staging information to identify those with:
- Distant recurrences
- Regional recurrences
- Local recurrences only or negative scans
This is important, because, theoretically, those with negative scans or local-only recurrences may be treated with curative intent, whereas the treatment goal in those with distant recurrences shifts to ‘disease control’. Patients with regional recurrences represent an evolving, heterogeneous group that may be managed with either ‘curative’ or ‘disease control’ intent, depending on the clinical situation.
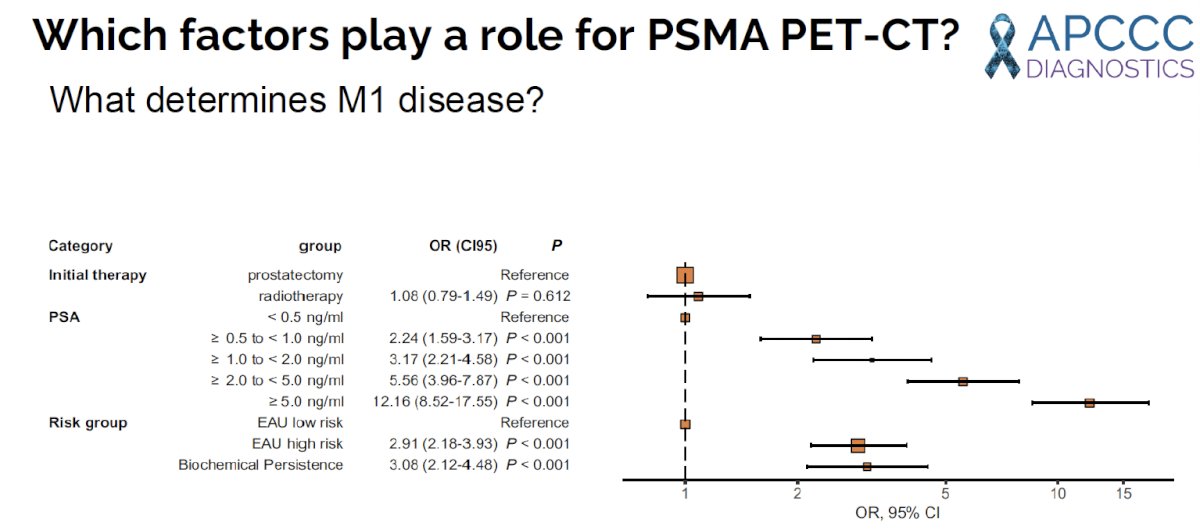
Thus, when ordering imaging for these biochemically recurrent patients, we need to consider the patient-level factors that predict the likelihood of detecting metastatic disease on imaging to optimize the yield of these scans and inform meaningful treatment decisions that may improve patient outcomes. With that in mind, what are the predictors of detecting M1 disease on PSMA PET/CTs? In 2022, Ferdinandus et al. evaluated 1,960 patients with biochemical recurrence or persistence following radical prostatectomy or radiotherapy and identified the following predictors of M1 disease on PSMA PET/CT:
- Higher PSA levels (PSA <0.5 ng/ml as reference):
- PSA 0.5–1 ng/ml: OR 2.2, p<0.001
- 1–2 ng/ml: OR 3.2, p<0.001
- 2–5 ng/ml: OR 5.6, p<0.001
- ≥5 ng/ml: OR 12.2, p<0.001
- Risk group (EAU low risk group as reference):
- EAU high risk: OR 2.9, p<0.001
- Biochemical persistence: OR 3.1
Illustrated in the image below is the distribution of PSMA PET positive disease among patients with EAU low risk biochemical recurrence, high risk biochemical recurrence, and biochemical persistence (high risk subgroup in the AUA risk classification):

Notably, 42% of patients in the high-risk group had M1 disease detected on imaging, compared to 32% of those with low-risk biochemical recurrence. Conversely, PET-detected N1 disease was more commonly present in the low-risk group (52% versus 33%). Negative PSMA PET scans were more frequently present in the high-risk group (25% versus 16%). Among those with biochemical persistence, M1, N1, and negative scans were noted for 40%, 38%, and 22% of patients, respectively.2
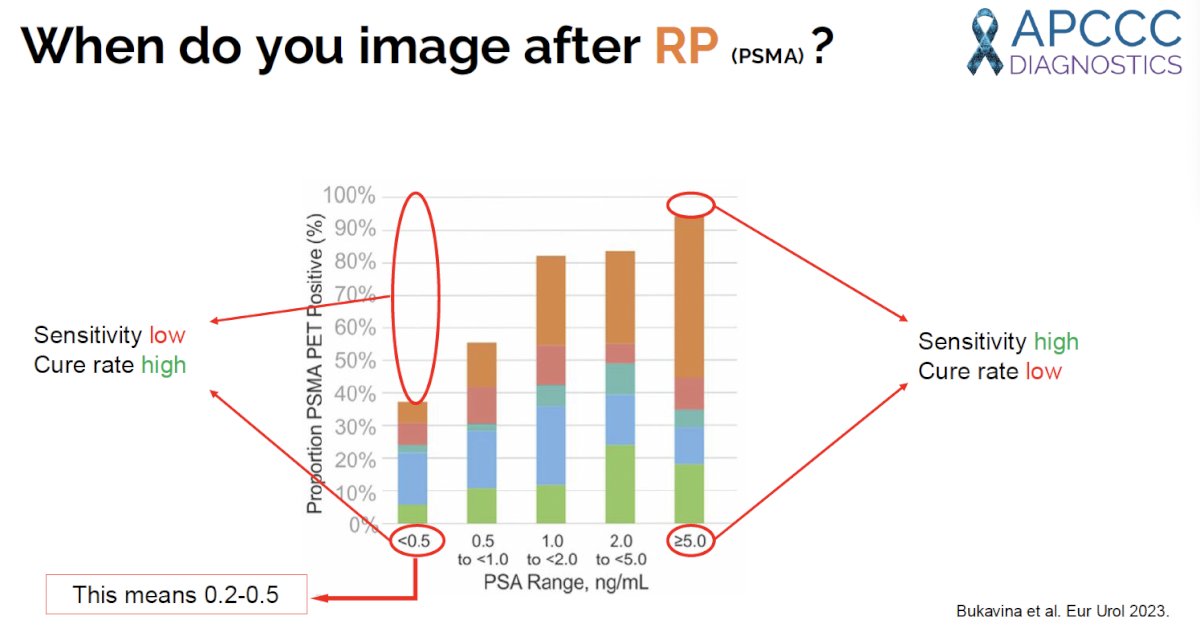
How does the diagnostic yield of a PSMA PET vary by serum PSA levels at imaging in post-radical prostatectomy patients? In a 2023 systematic review conducted by Dr. Ost and colleagues, the diagnostic yield of a PSMA PET for any sites of disease recurrence/persistence, including prostate bed recurrences (in green), at a PSA level <0.5 ng/ml was 38%. This increases to ~55% at a PSA range of 0.5–1 ng/ml, and subsequently >80% for serum PSA levels ≥1 ng/ml.3
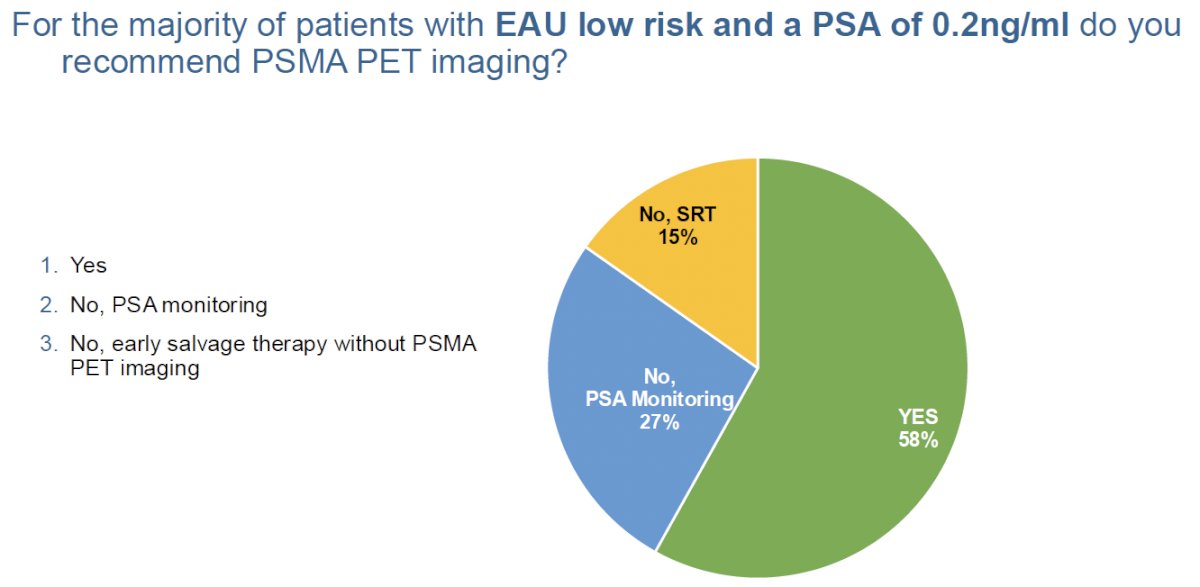
What are the experts’ consensus on the appropriate timing of imaging for these patients? Dr. Ost presented summary data from the 2024 APCCC report on the management of patients with advanced prostate cancer that was recently published in European Urology.4 When queried: “For the majority of patients with EAU low risk biochemical recurrence and a PSA of 0.2 ng/ml, do you recommend PSMA PET imaging?”, the majority (58%) responded with ‘yes’, with 27% recommending PSA monitoring and 15% favoring early salvage radiotherapy without PSMA PET imaging.
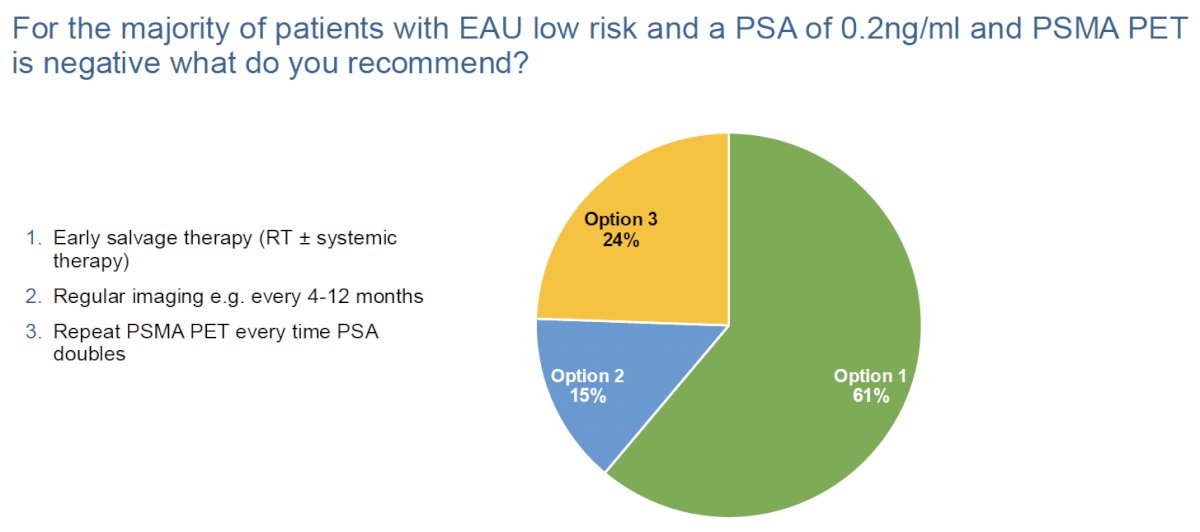
For the majority of patients with EUA low risk biochemical recurrence, a PSA of 0.2 ng/ml, and negative findings on PSMA PET, 61% recommended early salvage therapy with radiotherapy +/- systemic therapy. Other options that were recommended in this setting by the experts included repeating the PSMA PET once the serum PSA level doubles (24%) and regular imaging every 4–12 months (15%).
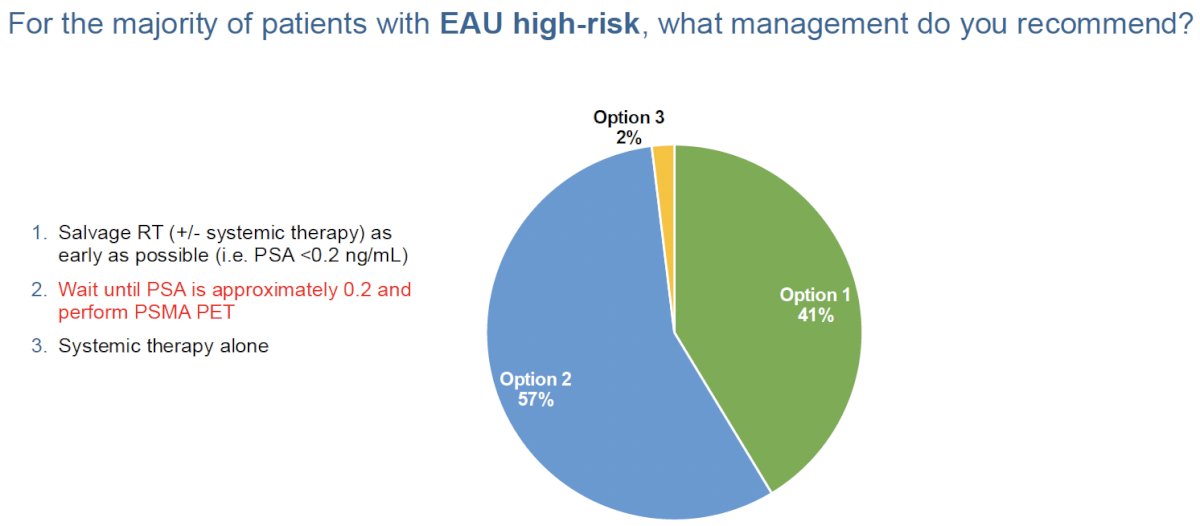
Shifting to the management of patients with EAU high-risk biochemical recurrence, 57% recommended waiting until the PSA is ~0.2 ng/ml and performing PSMA PET at that time, whereas 41% recommended salvage radiotherapy (+/- systemic therapy) as early as possible (i.e., PSA <0.2 ng/mL).
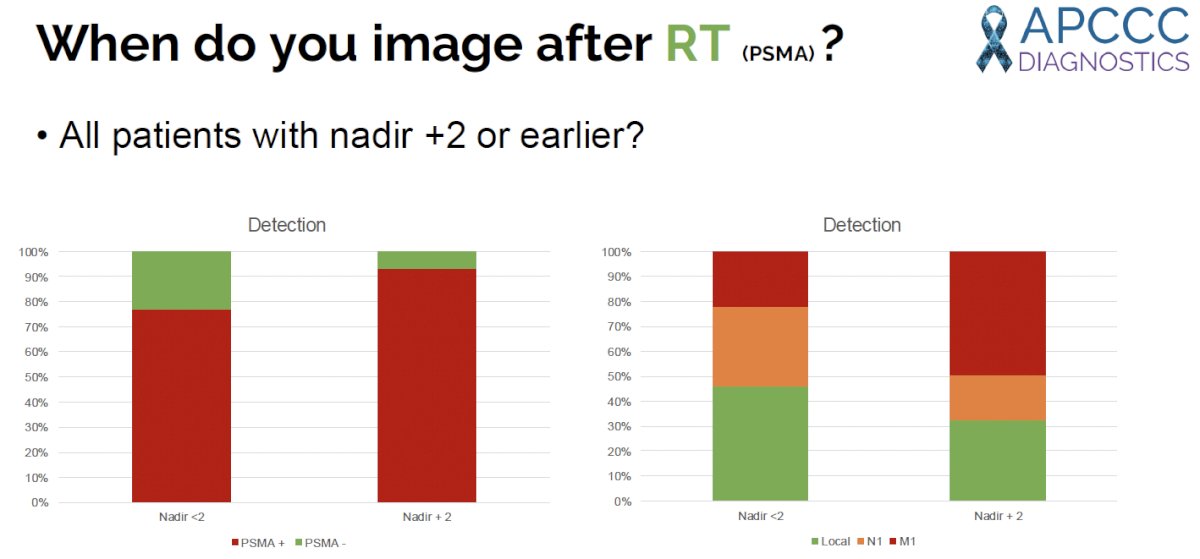
How does the serum PSA level in the post-radiotherapy biochemically recurrent setting influence the diagnostic yield of PSMA PET imaging? For patients with a PSA level <2 ng/ml above nadir, the detection rate was ~77%. This increases to ~93% in patients with a serum PSA level >2 ng/ml above nadir. The distribution of PET-positive findings among those with a positive scan also varied by PSA level, with patients in the PSA <2 ng/ml above nadir significantly more likely to have local disease (45% versus 32%) and N1-positive findings (31% versus 19%). Conversely, those with a serum PSA level >2 ng/ml above nadir were more likely to have M1 disease (49% versus 22%).
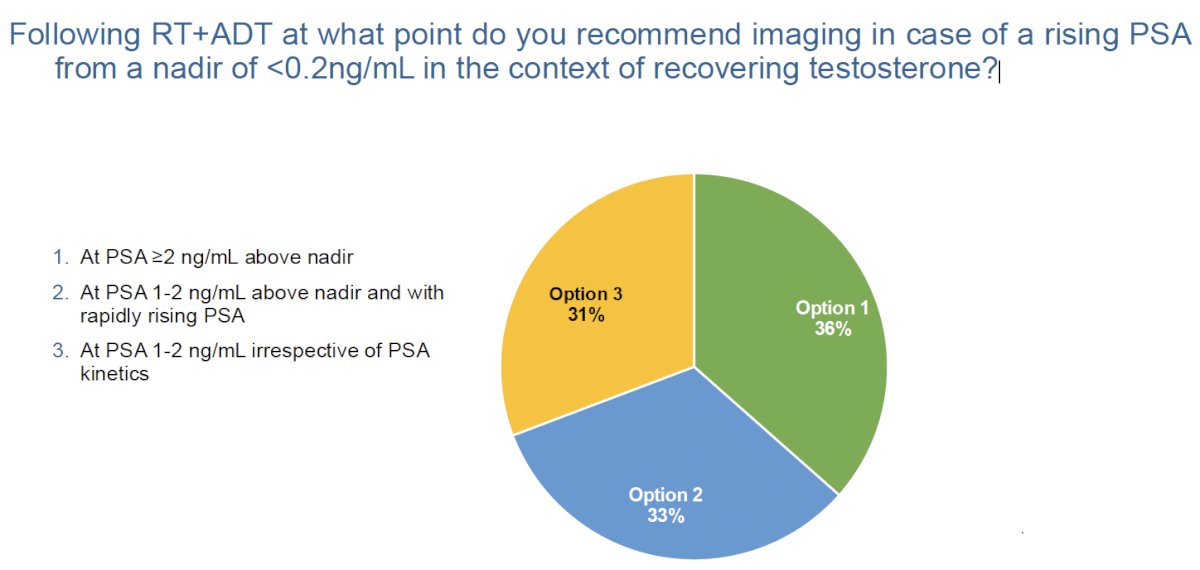
For eugonadal patients with a rising PSA following a nadir of <0.2 ng/ml post-radiotherapy + ADT, the experts were split regarding the optimal timing of imaging:
- 36% recommended waiting until the PSA was ≥2 ng/ml above nadir
- 33% recommended waiting until the PSA was 1–2 ng/ml above nadir, in the context of a rapidly rising PSA
- 31% recommended performing imaging at a PSA of 1-2 ng/ml, irrespective of PSA kinetics
Dr. Ost concluded his presentation with the following take home messages:
- Only perform imaging if the results will impact your management
- Use the most sensitive tool – PSMA PET/CT
- The probability of a positive scan in the biochemically recurrent setting is strongly correlated with the EAU risk grouping and serum PSA value at imaging
- Perform imaging at the following cut-offs:
- After radiotherapy: Nadir + 2 ng/ml (weak recommendation, per EAU guidelines)
- After radical prostatectomy: When PSA >0.2 ng/ml (strong recommendation)
Presented by: Piet Ost, MD, PhD, Associate Professor, Radiation Oncology, Faculty of Medicine and Health Sciences, University of Gent, Belgium
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Roach M3rd, Hanks G, Thames HJr, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys. 2006; 65: 965–974.
- Ferdinandus J, Fendler WP, Farolfi A, et al. PSMA PET Validates Higher Rates of Metastatic Disease for European Association of Urology Biochemical Recurrence Risk Groups: An International Multicenter Study. J Nucl Med. 2022; 63(1): 76-80.
- Bukavina L, Luckenbaugh AN, Hofman MS, et al. Incorporating Prostate-specific Membrane Antigen Positron Emission Tomography in Management Decisions for Men with Newly Diagnosed or Biochemically Recurrent Prostate Cancer. Eur Urol. 2023; 83(6): 521-533.
- Gillessen S, Turco F, Davis ID, et al. Management of Patients with Advanced Prostate Cancer. Report from the 2024 Advanced Prostate Cancer Consensus Conference (APCCC). Eur Urol. 2025; 87(2): 157-216.