(UroToday.com) The 2025 APCCC Diagnostics annual meeting featured a session on how to diagnose prostate cancer and a presentation by Dr. Gerhardt Attard discussing molecular tests at diagnosis for risk stratification, focusing on advanced prostate cancer. Dr. Attard started his presentation by providing a high level view of tumor DNA clinical next generation sequencing. He notes that the molecular taxonomy of prostate cancer is organized as neat groups of mutually exclusive genomic lesions, highlighting primarily “early events.” However, this is of limited utility for predicting the risk of death or metastases:
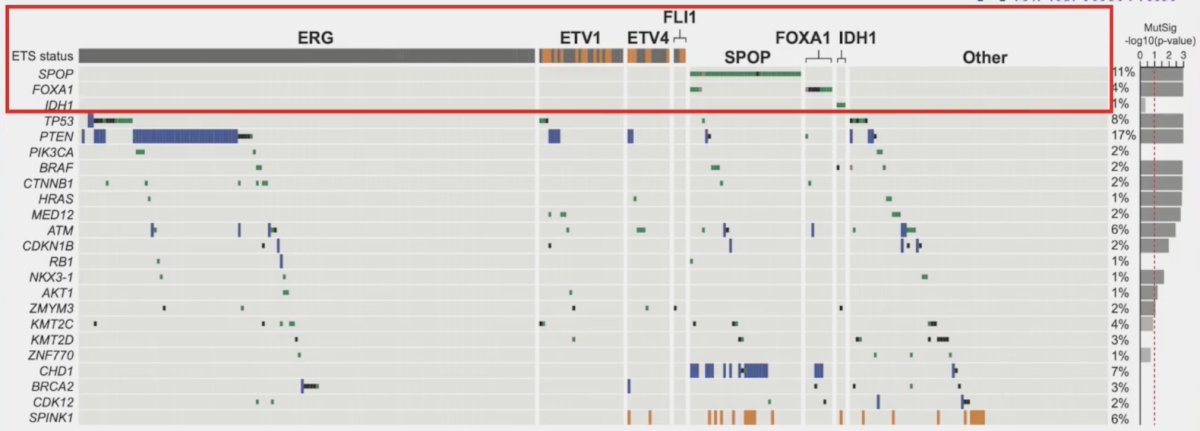
More specifically, Dr. Attard notes that the “bad actors” are historically TP53, PTEN, RB1, and BRCA2:

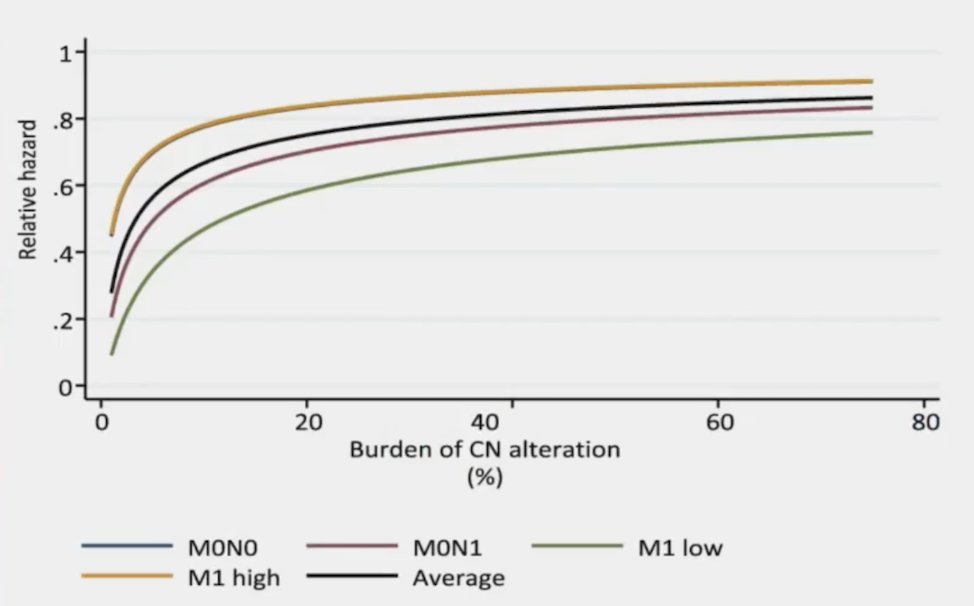
It is important to note that the genomic burden reaches a prognostic plateau across all prostate cancer disease spaces, typically at ~5-10% of the burden of CN alteration:1
Dr. Attard notes that clinical next generation sequencing does have its challenges, which include (i) a high failure rate, (ii) false negatives, (iii) under sampling (secondary to tumor heterogeneity), and (iv) missed deletions.
Dr. Attard highlighted that recent work from de Bono et al.2 suggests that PTEN loss by immunohistochemistry does not fully capture the AKT/PI3K-dependent tumors in mCRPC:

Dr. Attard also mentioned that work from the STAMPEDE platform on PTEN will be presented at ASCO and suggests that PTEN immunohistochemistry is prognostic in localized disease, but not in M1 disease.
Next, with regards to germline DNA testing, Dr. Attard emphasized that if there is at the very least one specific mutation we absolutely have to assess, it is BRCA alterations. BRCA testing is recommended for all high risk localized and M1 patients at diagnosis and can be combined with tumor testing. Subsequently, the results of germline testing should tailor management, and cascade testing of family members should be considered.
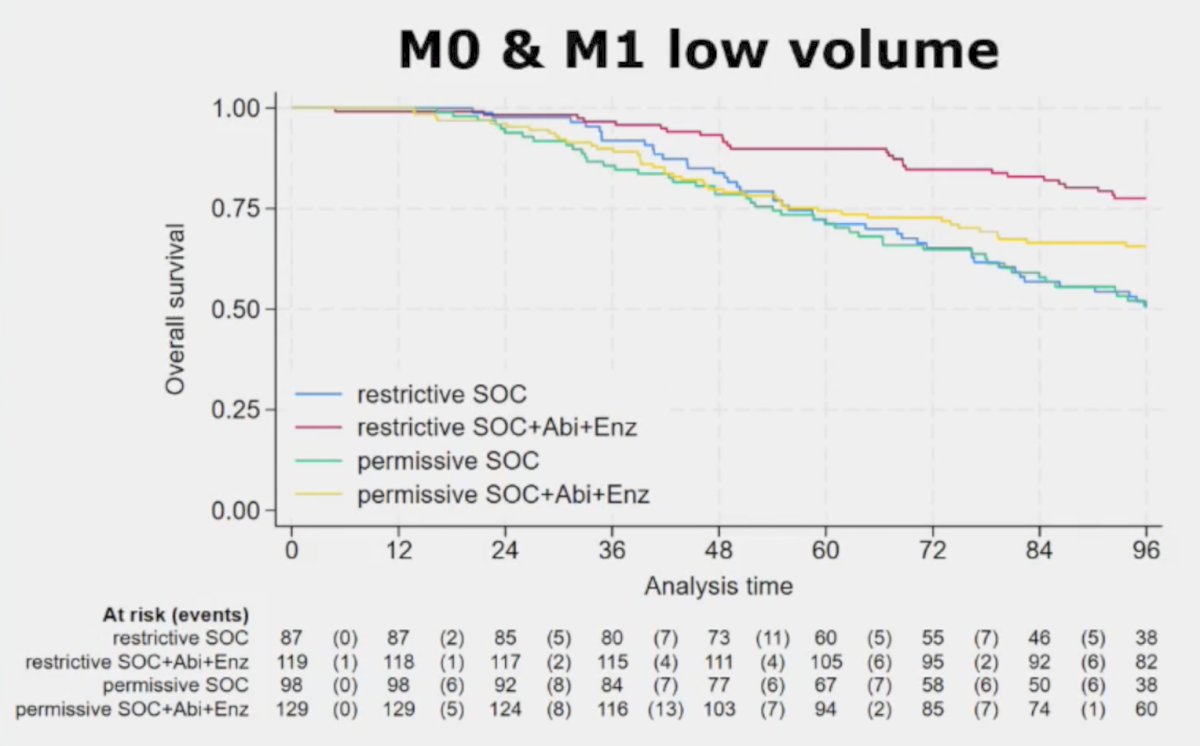
A less common, but potentially clinically relevant alteration is HSD3B1, with missense encoding adrenal permissive form of HSD3B1 generating a hyperactive 3BHSD1 enzyme. Recently presented work at GU ASCO 2025 by Sharifi and colleagues suggests that germline HSD3B1 polymorphisms may reduce the survival benefit of adding an androgen receptor pathway inhibitor to ADT in low volume and M0 advance prostate cancer, however, there was no association with overall survival in high volume disease (HR 1.14, 95% CI 0.78-1.67):
Dr. Attard then discussed mRNA profiles, emphasizing that mRNA signatures are associated with disease aggressiveness. The Decipher genomic classifier is prognostic across disease states, with no discernible prognostic difference for signatures capturing proliferation. However, the clinical impact of many signatures is context dependent:

In the STAMPEDE trial platform, Dr. Attard notes that data presented at ESMO 2024 by Grist and colleagues suggest that a high Decipher score identified patients more likely to benefit from docetaxel, with a biomarker-treatment interaction effect p-value of 0.039:

This was most notable in low volume patients, where the addition of docetaxel to ADT was associated with an overall survival benefit HR of 0.53 (95% CI: 0.32–0.88) in patients with high Decipher scores. Conversely, there was no significant overall survival benefit in the low-volume patients with lower Decipher scores who received treatment intensification with docetaxel (HR: 0.78, 95% CI: 0.47–1.30):

Decipher score was similarly predictive of an overall survival treatment benefit with docetaxel addition to ADT in high volume patients:

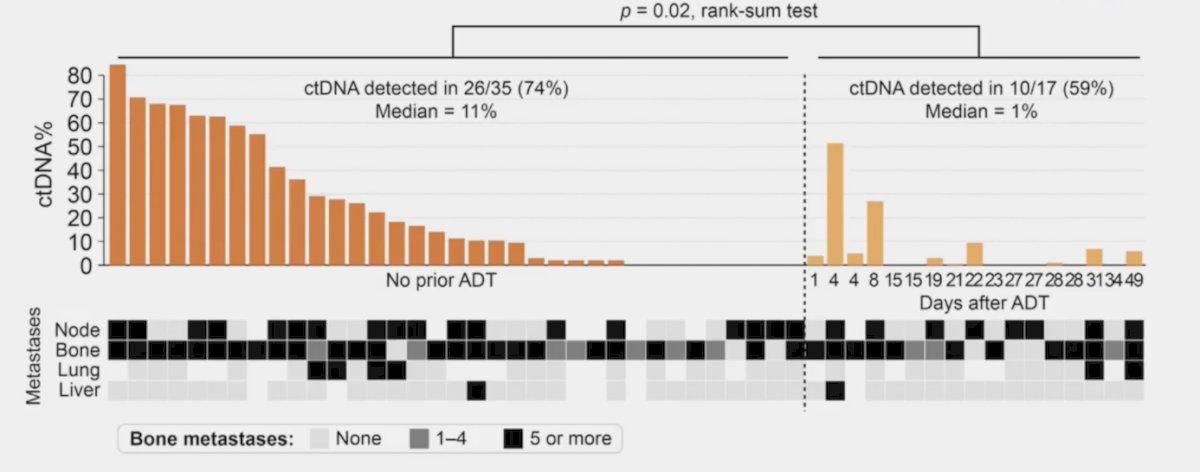
Finally, Dr. Attard briefly discussed blood tests, focusing on ctDNA at diagnosis. Work from Vandekerkhove et al.3 assessed ctDNA abundance at de novo mHSPC diagnosis among 53 newly diagnosed patients and whether ctDNA provides complementary clinically relevant information to a prostate biopsy. They found a median ctDNA fraction of 11% (range 0-84%) among untreated patients, but lower (1.0%, range 0-51%) among patients after short term ADT. TP53 mutations and DNA repair defects were identified in 47% and 21% of the cohort, respectively. Combined ctDNA and tissue analysis identified potential driver alterations in 94% of patients, whereas ctDNA or prostate biopsy alone was insufficient in 19 cases (36%):
At ESMO 2024, Horvath and colleagues presented the results of an ad hoc analysis of the ENZAMET trial evaluating the association between the lipid biomarker, PCPro, and clinical outcomes in mHSPC patients. The overall survival of PCPro-positive patients was not improved by enzalutamide treatment when compared to non-steroidal antiandrogen (median: 50 versus 49 months; HR 1.10, p = 0.69), unlike PCPro-negative patients (median: not estimable versus 70 months; HR 0.61, p < 0.0001), indicating that PCPro-positive patients may be resistant to enzalutamide therapy:

Dr. Attard concluded his presentation by discussing molecular tests at diagnosis for risk stratification, focusing on advanced prostate cancer, with the following take-home points:
- Tumor DNA sequencing is clinically informative for drug selection in mCRPC and may have a role in treatment selection at diagnosis
- Germline DNA testing for BRCA is recommended for all high risk and M1 patients (and could be combined with tumor testing)
- The current evidence suggests that mRNA profiling is superior to clinical features or genomics for predicting time to metastases or death
- ctDNA is currently of limited use at diagnosis
- The added value of molecular tests + novel imaging is currently uncertain
- There is ongoing work with European payers to accept Simon’s level 1B evidence in an attempt to avoid having to redo clinical trials
Presented by: Gerhardt Attard, MD, PhD, University College London Cancer Institute, London, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Grist E, Friedrich S, Brawley C, et al. Accumulation of copy number alterations and clinical progression across advanced prostate cancer. Genome Med. 2022 Sep 5;14(1):102.
- De Bono JS, He M, Shi Z, et al. Final overall survival and molecular data associated with clinical outcomes in patients receiving ipatasertib and abiraterone in the phase 3 IPATential150 trial. Eur Urol. 2025 Jan 29;S0302-2838(24)02771-4.
- Vandekerkhove G, Struss WJ, Annala M, et al. Circulating tumor DNA abundance and potential in de novo metastatic prostate cancer. Eur Urol. 2019 Apr;75(4):667-675.